
Abstract
Objective
The aim of the present study was to evaluate the impact of continuous ambulatory peritoneal dialysis (CAPD) on the lifestyle of elderly patients.
Patients and Methods
Aspects of health-related quality of life (QL) were studied in 48 patients (16 men, 32 women) in end-stage chronic renal failure (ESRF) undergoing CAPD at the Clinic of Nephrology, Clinical Centre of Serbia. The first group comprised 20 adult patients (8 men, 12 women; age range: 35 – 59 years). The second group consisted of 28 older adult patients (8 men, 20 women; age range: 65 – 75 years). Mean length of CAPD treatment was 5.2 years in the first group and 3.67 years in the second group. Fifteen QL variables were investigated: marital status, family relationships, working ability, sleep, tiredness, appetite, wound healing, hobby, sports, friendships, sexual activity, mood, travel, self management, and happiness.
Results
The results showed that, in the examined groups, marital status and relationships with family members weren't influenced at all by dialysis. In both groups, CAPD had a negative influence on ability to bear cold and to travel, but other life functions were not significantly affected. Elderly patients had a significantly worse appetite (p = 0.03, Fisher test) and mood (p = 0.045, Fisher test) than did younger adults. In other examined variables, no statistically significant differences were found between the groups.
Conclusions
Lack of large, statistically significant differences between the groups suggests that CAPD has an equal influence on quality of life in younger and older adult patients.
With the worldwide trend toward an aging general population, the number of elderly patients being treated with PD is also increasing. The aim of the present study was to assess the impact of continuous ambulatory peritoneal dialysis (CAPD) on the quality of life of elderly patients.
Patients and Methods
The study included 48 patients (16 men, 32 women) treated with CAPD at the Clinic of Nephrology, Clinical Centre of Serbia, in Belgrade, Yugoslavia. The inclusion criteria were
exclusive treatment with peritoneal dialysis, uncombined with another modality (that is, hemodialysis or transplantation), and
the intellectual and mental capacity to understand and answer the questionnaire.
Patients were allocated to one of two groups. The first group included 20 patients 35 – 59 years of age; the second group included 28 patients 65 – 75 years of age. Primary renal disease had a similar distribution in both groups: 25% glomerulonephritis, 20% diabetic nephropathy, 18% nephrosclerosis, 6% pyelonephritis, 5% endemic nephropathy, and 26% unknown origin. Only 10% of patients were receiving erythropoietin. Table 1 shows the general characteristics of the patients.
All patients were asked to complete an original questionnaire that was designed based on the Karnofsky Index (4), the Nottingham Health Profile (5), the Sickness Impact Profile (6), and the Kidney Disease Quality of Life. The questionnaire included 3 domains and 15 items: social (marital status, family relationships, working ability), physiologic (tiring, sleep, appetite, wound healing), and personal (travelling, sports, hobbies, friendships, sexual activity, mood, home maintenance, happiness). Working ability was assessed by the “circle method”: Patients were asked to imagine that full circle represented past working ability. They were then asked to mark the part of the circle that would correspond to present working ability (7). Marital status and family relationship data before treatment and at the present time were obtained using yes-or-no questions. All the other questions had four gradations in meaning: Yes, Mostly yes, Mostly no, and No.
Patient Characteristics
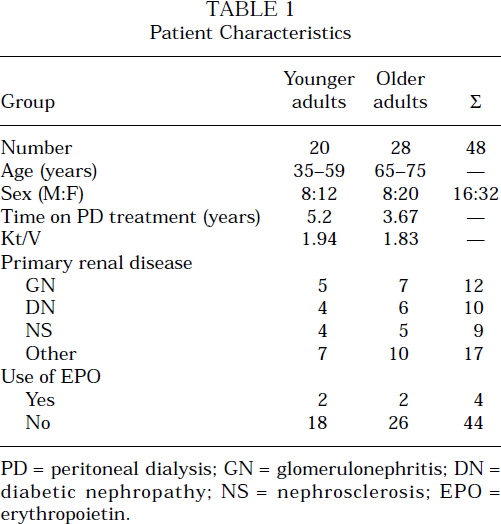
PD = peritoneal dialysis; GN = glomerulonephritis; DN = diabetic nephropathy; NS = nephrosclerosis; EPO = erythropoietin.
Data were analyzed using Fisher test, McNemar test, and Student t-test.
Results
Compared to the situation before commencement CAPD treatment, no changes were seen in marital status and family relationships in most patients. Changes were seen only in 3 elderly patients, owing to a change in marital status (having become widows or widowers). Those results were to be expected, keeping in mind the patriarchal organization and the strong tradition of preserving close family relationships in our region.
Working ability was diminished in both patient groups. Younger patients estimated present ability at an average of 50%, as compared to 100% before the illness. Elderly patients estimated present working ability at about 40%. In most younger patients [15 people (75%)], the decreased work ability resulted in shorter working hours or even in early retirement.
Most of the patients in both groups—15 (75%) in the younger group and 24 (86%) in the older group— reported tiring easily. No statistical difference was seen between the groups.
Most of the patients in both groups stated that they sleep well most of the time. None of the patients had noticed any changes in wound healing.
Some 71% of elderly patients (20 of 28) noticed worsening of appetite since the beginning of CAPD treatment. A statistically significant difference (p = 0.03) was seen between the groups, because only 5 younger patients (25%) reported a change in appetite in connection with the start of CAPD treatment (Figure 1).
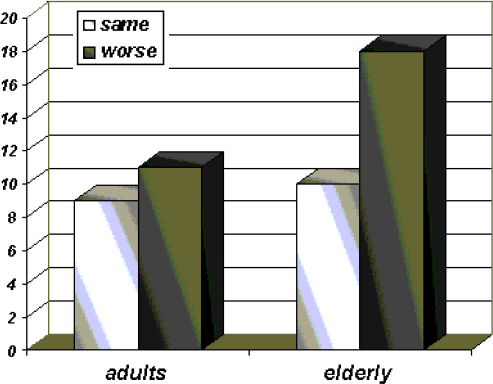
Appetite in the study patients (p = 0.03).
In the study, “travelling” was defined as “leaving home for a couple of days or more—meaning summer or winter holidays, excursions, weekends away, and so on.” No statistical difference was found between groups, because most patients in both groups stated that they travelled less than before. However, some of the younger patients who reported that they travelled less (4 of 17) blamed their financial situation and not the illness.
None of the elderly patients had practiced a sport even before their illness or the CAPD treatment, but 7 of the younger patients (35%) who had played football, basketball, or volleyball as recreation had ceased to do so since starting CAPD treatment. The difference between the groups was not statistically significant.
Only a few patients, 5 in the first group (25%) and 5 in the second group (18%) stated that they had some kind of a hobby: reading, fishing, writing poetry, playing chess, knitting, and embroidery. Two younger and three older patients continued to pursue their hobbies after the start of CAPD treatment. No statistical difference was seen between the groups.
About two thirds of patients in both groups [13 younger adults (65%) and 16 older adults (57%)] were still socializing with old friends, but an even larger number (15 younger adults (75%) and 17 older adults (61%)] were making new acquaintances easily—albeit mostly in hospital surroundings. No statistically significant differences were observed between the groups, although there was a tendency for younger patients to preserve old friendships and to make new ones more often than the older patients did. That finding is important, because social support may protect against some of the deleterious effects of the stress caused by a medical illness (8).
In contrast to the fact that most patients hadn't changed marital status and were satisfied with their marriage, only 6 younger adults (30%) and 5 elderly adults (18%) had satisfactory sexual relationships. The groups were not statistically significant in this regard, and those data correspond with the findings of other authors (3).
More then three quarters of the older patients [22 people (79%)] noticed that, since the start of CAPD, they were often in a bad mood. Only a few of the younger patients [5 people (25%)] observed a mood change (Figure 2). On that item, the difference between the groups was statistically significant (p = 0.045).
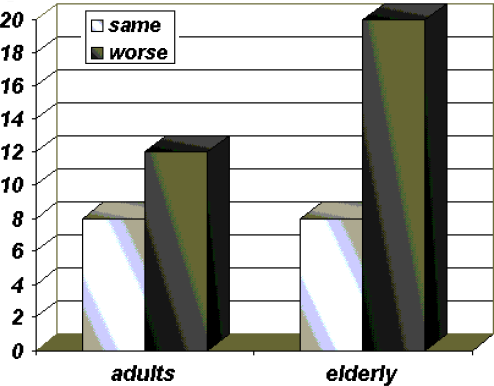
Mood in the study patients (p = 0.045).
It is important to note that all of the study patients stated that they were capable of caring for themselves and for their household. They indicated that they were in no need of extra help. It is also interesting that a greater number of the older patients [20 people (71%)] than of the younger ones [9 people (45%)] expressed satisfaction with their lives and considered themselves more or less happy.
Discussion
The interest in measuring quality of life in relation to health care has increased enormously in recent years, especially in chronic renal failure patients. Assessing quality of life in patients with end-stage renal failure could provide more accurate evaluation of the health of individuals or populations, and of the benefits and harms that may result from health care interventions. Such evaluations are even more important in end-stage renal failure care where advances are not uncommon and where alternative therapies to manage patients are available (3).
Because end-stage renal disease is a chronic disease that disproportionately affects vulnerable populations such as older people, the clinical and social problems affecting health-related quality of life are many (9). Understanding how disease complications affect a patient's everyday life is the purpose of health-related quality of life measurement. Obtaining reliable, valid quality-of-life data can assist patients and providers in making decisions about treatment modalities. Such data are therefore an important component in the advancement of disease treatment in the ESRF population (10).
Studies by authors outside of Serbia suggest that CAPD has an extremely positive impact on patients’ quality of life (11). For older patients with ESRF, CAPD is well tolerated and shows superiority over in-center hemodialysis (3). As for comparing the effect of CAPD on quality of life in older and younger patients, the results of previous studies are contradictory. Patients over the age of 65 have been reported to have a better quality of life as compared with younger patients, in part because of more and better coping mechanisms (3). However, another study reported that older patients were likely to have a worse quality of life because of greater incidence of depression and a greater number of psychosomatic complaints (12).
We found statistically significant differences only in appetite and mood, both of which were worse in elderly patients. Social support from friends, family, or significant others was omnipresent in our study patients and is of great importance. From a social viewpoint, it is very important that even elderly patients are capable of taking care of themselves and are independent in everyday life (excluding consideration of possible financial dependence). The fact that more older patients than younger ones considered themselves happy could be explained by the fact that the younger group, sentenced to lifelong illness and treatment, cannot consider themselves very lucky, while the older group can make an overall life evaluation judging by the things that they already have accomplished.
It is important to note that only about 10% of CAPD patients in Yugoslavia (including the patients in the present study) are receiving erythropoietin. Because other investigators showed that partial correction of anemia with erythropoietin significantly increases quality of life, functional ability, and physical working capacity, especially in younger patients, the lack of good anemia correction in our patients could also be a reason for the limited statistically significant differences (13,14,15).
Conclusion
End-stage renal failure and treatment complications affect the functional abilities of patients and limit their lifestyles. Peritoneal dialysis provides younger and older patients with a quality of life that varies little between the groups. That uniformity is important when the medical, psychosocial, and economic hardships that those patients withstand are considered.