
Abstract
Objective
Isoprene is the constitutive unit of isoprenoid lipids and sterols. However, it is also a potential toxic and carcinogenic agent. Recent findings of a marked and prolonged isoprene overproduction induced by hemodialysis sessions raises the question of isoprene behavior in patients on peritoneal dialysis.
Design
A study with repeated measures per patient and healthy control.
Setting
Nephrology and Dialysis Unit and Perugia University Medical School.
Patients
Sixteen consecutive patients on regular continuous ambulatory peritoneal dialysis (CAPD) were evaluated. Endogenous isoprene was analyzed using gas chromatographic assay of breath isoprene, collected at set times before and after dialysis fluid exchange.
Results
No significant variations were found in breath isoprene concentrations in the different samples from each patient, and levels were almost stable within the normal range of healthy controls.
Conclusion
These results show that CAPD, unlike hemodialysis, has little or no effect on isoprene and isoprenoid-related lipid turnover. This lack of increased endogenous isoprene synthesis, in addition to being a distinctive metabolic feature of CAPD, could have important pathophysiological and clinical implications.
Keywords
Extracorporeal dialysis, or hemodialysis (HD), and peritoneal dialysis (PD) — most often continuous ambulatory peritoneal dialysis (CAPD) — are two modalities of treatment for end-stage renal disease considered alternatives, even though there may be remarkable differences in efficacy, physiology, contraindications, and complications. Problem areas for dialysis patients include continuous versus intermittent dialysis, biocompatibility and safety of the procedure, contamination, adequacy in removing small and large solutes, hemodynamic stability, anticoagulation, long-term prognosis, and the incidence of some diseases, including myocardial infarction and cerebrovascular accidents, infections, amyloidosis, cancer. (1-11). Evaluating differences in changes associated with the type of dialysis may be of interest in pathophysiological and clinical settings.
A new metabolic aspect described to date only in HD patients is the increased breath isoprene exhalation observed in regular 4-hour (0800 hours, 1200 hours,) three-times-weekly maintenance HD (12). Breath isoprene was increased in all patients. The overproduction was HD-induced, became evident in the postdialysis period, and followed a biphasic pattern with significantly increased overproduction also persisting the morning after, on the non-HD day (13). This behavior pattern could have clinical and biological value because cells depend on isoprenoids derived from mevalonate for growth, differentiation, and maintenance of homeostatic functions (14); moreover, isoprene is thought to have carcinogenic and toxic effects (15-18). There are no data on the behavior patterns of breath isoprene during PD.
The aim of this study was to evaluate breath isoprene patterns in patients undergoing CAPD.
Patients and Methods
Patients
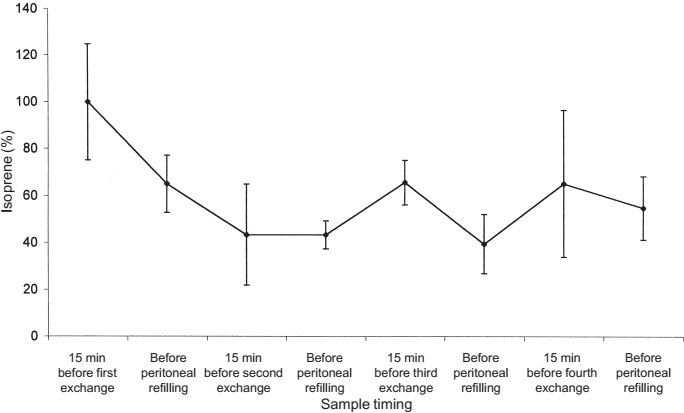
Sixteen consecutive patients (8 men and 8 women; mean ± SD age 62.2 ±13 years, range 29 – 77 years) on stable CAPD were evaluated. All patients were treated with standard PD solutions, with lactate as buffer and glucose as osmotic agent at different concentrations according to individual need. Mean duration of dialysis treatment was 30.4 ± 20.2 months (range 9 – 79 months). Each patient had 3 daytime exchanges and 1 nighttime exchange. Detailed information on the 16 patients included in the study is shown in Table 1.
Patients’ Clinical Variables
CIN = chronic interstitial nephritis; PKD = polycystic kidney disease; CGN = chronic glomerulonephritis; HNS = hypertensive nephrosclerosis.
Stay-Safe, Fresenius Medical Care Science and Product Consulting, Bad Homburg, Germany; Fres/S.S3/99, Fresenius; Dianectan S, Laboratoire Aguettan, Lyon, France; Baxter T, Baxter Healthcare Corp. (Renal division), McGaw Park, Illinois, USA; Bieffe, Bieffe Medital S.p.a., Milan, Italy; Periline, Haemopharm Health Care, Milan, Italy.
Breath Sampling and Isoprene Assay
Isoprene concentration in exhaled breath was determined by gas chromatographic analysis as reported elsewhere (12). Briefly, 1-L Tedlar bags (SKC Inc., Eighty Four, Pennsylvania, USA) were used for collecting breath. The first 500 mL was split off (dead space) and only the end of the alveolar breath was collected. New and used bags were purged by helium flow. All bags were tested before sampling. Fixed amounts of breath samples (100 mL) were absorbed on to a glass tube filled with preconditioned Carbosieve, Carbotrap, and Carbotrap C (Varian–Chrompack Italy, Turin, Italy) by suction pump (25/30 mL/min). Thermo desorption cold trap unit (TCT) samples tubes were placed on a TCT/purge and trap injection (PTI) CP 4001 injector (Varian–Chrompack) and processed automatically. A gentle preflush (53°C, 4 minutes, helium flow 15 mL/minute) was used to remove the remaining nonadsorbed gas. Water removal is required to avoid aluminum column deactivation and to prevent ice formation in the trap. During thermal desorption (280°C, 6 minutes, helium flow 15 mL/min), the desorbed compounds were concentrated in a cryogenic trap (–100°C) by liquid nitrogen. Finally, flash heating sent the volatiles to the Al2O3/KCl column (25 m, 0.32 mm, 5.0 μm; Varian–Chrompack). The temperature program was 50°C for 2 minutes, increased 8°C/minute to 190°C, and final isotherm 15 minutes. Helium pressure was 80 kPa by flame ionization detector (250°C). A software program (Mosaic, Varian–Chrompack) running on a personal computer was used to analyze chromatograms and integration peaks.
Sample Timing
Exhaled breath was collected from the 16 patients (group A) immediately before and after the drainage phase of the first two daytime exchanges, and at the end of the first and second hours of the dwell period between the two. In a previous study performed in HD patients, the first breath isoprene increase was detected at the end of dialysis, but became more evident half an hour later; therefore, in one subgroup of 6 patients (group A2), refilling after the first drainage was delayed for 30 minutes, after which another sample was collected. In a second subgroup of 4 patients (group A3), who were followed up for 24 hours, exhaled breath was also collected before and after the third and fourth exchanges.
Statistical Analysis
Data are reported as mean ±SD. Analysis of variance was done and significance of differences was assessed by t-test for paired data analysis; a p value less than 0.05 was assumed significant.
Results
In the first part of the study, breath isoprene concentration was evaluated in samples collected from the 16 patients in group A during the first morning cycle [i.e., before (time 0) and soon after the first peritoneal drainage; 1 and 2 hours after the first peritoneal refilling; and before and soon after the second peritoneal drainage]. Figure 1 shows breath isoprene concentrations at these different sample times. At time 0, isoprene concentration was 5.52 ± 2.25 nmol/L, that is, almost identical to the level found in healthy subjects with normal renal function in our laboratory [breath isoprene levels in 89 healthy controls ranged from 1.4 to 10.8 nmol/L (5.06 ± 2.24 nmol/L)]. Concentrations remained almost stable without significant variation over time in samples collected from the same patient.
Breath isoprene during continuous ambulatory peritoneal dialysis. Breath samples were collected immediately before first morning drainage (t0), soon after first morning drainage (t1), 1 hour after first peritoneal refilling (t2), 2 hours after first peritoneal refilling (t3), immediately before second drainage (t4), and soon after second drainage (t5). Isoprene levels are reported as mean ±SD; (n = 16).
Figure 2 shows no variations in isoprene concentration occurring in the 6 patients in group A2 after refilling was postponed for 30 minutes.
Breath isoprene during continuous ambulatory peritoneal dialysis with delayed refilling. In this subset of patients (group A2; n = 6), abdominal refilling after the first drainage was postponed 30 minutes, at which time an extra sample was collected (t1D). Isoprene levels are reported as mean ±SD.
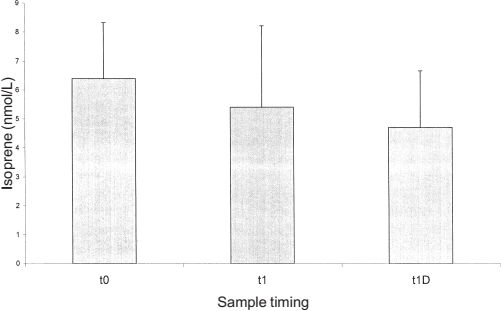
Finally, Figure 3 shows the behavior pattern in the 4 patients (group A3) in whom the breath isoprene concentration was measured in all four exchanges. Again, no significant differences were found, but there was a tendency toward a decrease during the diurnal hours in accord with the circadian rhythm of this hydrocarbon in normal subjects. Isoprene was not present in fluid used for dialysis and the isoprene concentration in ambient air was negligible (data not shown).
Time course of breath isoprene during continuous ambulatory peritoneal dialysis. In this subset of patients (group A3; n = 4), breath isoprene concentration was measured at specific time points for all four exchanges of the day. Isoprene levels are reported as mean percentage values ±SD.
Discussion
This is the first time that breath isoprene production has been evaluated in PD patients.
Breath isoprene levels were not significantly different from the normal healthy control values before, during, and after a peritoneal exchange. These findings suggest that, in CAPD patients, an isoprene endogenous overproduction does not occur, unlike in HD patients, in whom isoprene overproduction persists, for many hours after dialysis ends, in a biphasic behavior pattern with concentrations remaining high the next morning (a nondialysis day) (12,13).
The reasons for this different behavior are not known. An endogenous product of lipid metabolism, isoprene in man is believed to derive from the synthetic mevalonate pathway leading to sterols and isoprenoid lipids (Figure 4). This metabolic pathway appears to be strictly regulated at the level of mevalonic acid (MVA) (19-22), a low molecular weight, water-soluble substance, levels of which are increased in the plasma of uremic patients before a HD session and sharply reduced by HD (23).
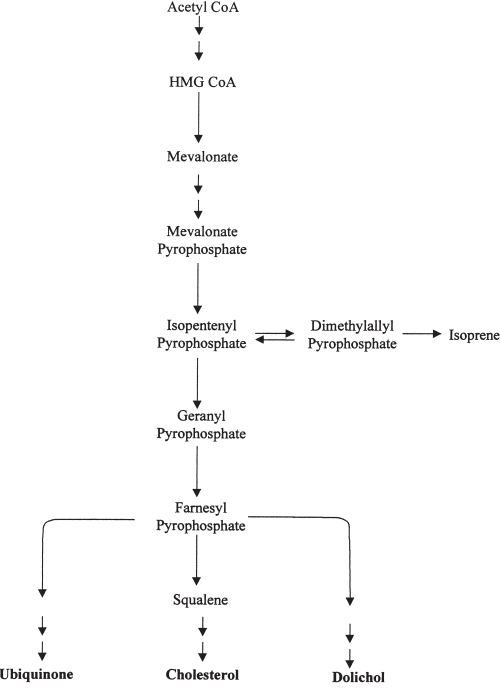
Branched pathway of mevalonate metabolism and isoprene biosynthesis.
On the contrary, isoprene (molecular weight 68.12, melting point –146°C, boiling point 34°C), a volatile liposoluble substance, is not removed by HD but is easily exhaled with alveolar air, in which it can be measured noninvasively by gas chromatography.
Differences in continuous and intermittent dialysis treatments probably play an important role in determining the different breath isoprene behavior pattern in HD and CAPD patients.
The first hypothesis is that, in a short space of time, HD removes great quantities of MVA, and consequently the MVA-regulated inhibitory mechanism, and initiates enzymatic induction mechanisms, which could result, after the end of the dialysis session, in the increased respiratory exhalation of isoprene in the biphasic behavior pattern described elsewhere (13). In CAPD patients, the slower and continuous removal of hydrosoluble isoprene precursors does not promote a clear isoprene overproduction.
Alternatively, intermediate mechanisms inducing isoprene overproduction may involve factors related to biocompatibility, to hemodynamic stress, or to other unknown factors associated with hemodialytic procedures per se.
Variations in alveolar respiration do not seem to play a major role in isoprene emission: in breath samples from dialyzed patients, no significant variations were found in alveolar levels of other volatile hydrocarbons (e.g., ethane, pentane, isopentane, propane, butane, and isobutane) (data not shown).
Whatever the causal mechanism(s), patients on HD, unlike those on CAPD, incur an increased isoprene biosynthesis and a prolonged overexposure consequent to repeated dialysis sessions.
Thus, variations in isoprene respiratory exhalation could reflect the effect of the dialysis session on lipid metabolism in uremic patients and could have repercussions in terms of cellular and cardiovascular physiopathology. High isoprene levels have been reported in patients with acute myocardial infarction (24). Furthermore, isoprene itself is acknowledged to have a possible direct pathogenic role. In fact, chemically, isoprene [H2C=CHC(CH3)=CH2] is an analogue of butadiene, which is reputed to be a toxic, mutagenic, and carcinogenic agent (15-17). In experimental models, even episodic exposure to isoprene has increased the incidence of various neoplasias, even many years after exposure (18). This hydrocarbon is thus the object of growing interest as a potentially harmful noxious agent for human beings.
In conclusion, the lack of an increase in isoprene levels during CAPD appears to be not only a distinctive feature of this type of dialysis, but also a metabolic phenomenon that deserves further investigation and that could be of remarkable physiological, clinical, and prognostic interest in these patients.
Footnotes
Acknowledgments
The authors thank Dr. Geraldine Anne Boyd for revising the English version of this paper, and Fortuna Gino Girolamo and Marinacci Giuliana for their technical expertise.