
Abstract
Background
A new genus in the family Flaviviridae has recently been discovered; it has provisionally been designated GBV-C/HGV. As determined by virologic techniques [reverse-transcription polymerase chain reaction (RT-PCR)], infection with GBV-C/HGV is frequent in renal transplant (RT) recipients and in patients on chronic hemodialysis (HD). The epidemiology of GBV-C/HGV infection in patients on peritoneal dialysis is scarce and mostly based on RT-PCR technology.
Purpose
We report on the prevalence (as detected by serologic and virologic techniques) and the risk factors for GBV-C/HGV infection in a cohort of patients on continuous ambulatory peritoneal dialysis (CAPD). We also tested a control group of blood donors.
Methods
Infection by GBV-C/HGV was assessed by serologic and virologic techniques. Cases of GBV-C/HGV viremia (GBV-C/HGV RNA) were detected by RT-PCR. Antibodies to the envelope protein of GBV-C/HGV (anti-E2 GBV-C/HGV antibody) were analyzed by serologic methods.
Results
We found a high frequency [17/85 (20%)] of GBV-C/HGV. The rates of GBV-C/HGV viremia and anti-E2 GBV-C/HGV positivity were 10.5% (9/85) and 10.5% (9/85) respectively. In most patients [17/18 (94%)], the presence of anti-E2 GBV-C/HGV antibody was associated with clearance of GBV-C/HGV from serum. No relationship was noted between anti-E2 GBV-C/HGV antibody (or GBV-C/HGV viremia) and age, sex, race, time on dialysis, anti-HCV antibody, HBsAg status, and anti-HIV positivity. The frequency of GBV-C/HGV infection in CAPD patients was much higher than that in blood donors, even if the difference did not approach statistical significance. No associations between GBV-C/HGV positivity and biochemical liver tests [aminotransferase and gamma glutamyl transpeptidase (GGT)] were apparent.
Conclusions
Infection by GBV-C/HGV as detected by RT-PCR and anti-E2 antibody was common in patients on CAPD and in controls alike. No association was seen between GBV-C/HGV and various demographic or clinical factors. The clinical significance of GBV-C/HGV in CAPD remains unclear. Larger investigations are in progress.
During the 1990s, two independent teams (1-2) detected presumed hepatitis agents provisionally designated hepatitis G virus (HGV) and hepatitis GB virus C (GBV-C). Those agents represent a new genus in the family Flaviviridae. The GBV-A and GBV-B viruses are similar to HGV, and GBV-C is highly homologous to HGV. To date, the association of GBV-C/HGV infection with clinical disease has not been convincingly demonstrated. A high prevalence of GBV-C/HGV infection in patients with fulminant (3-4), acute (5), and chronic hepatitis (6) and with normal renal function has been observed; however, several lines of evidence do not support a role for GBV-C/HGV in the pathogenesis of liver disease in humans (7).
The epidemiology of GBV-C/HGV infection in patients with end-stage renal disease (ESRD) was extensively addressed in reports published in the late 1990s (8-37). The frequency of GBV-C/HGV infection in the dialysis population is high (7). Transfusion requirement (8,9,14,18,19,21,32), time on dialysis (17,19,25,32), and renal transplantation (10) have been reported in association with GBV-C/HGV infection in some series. A link between GBV-C/HGV and HCV infection has been found by other investigators (9,11,32). The clinical significance of GBV-C/HGV infection in ESRD remains unclear (7). Most of the information on GBV-C/HGV infection in ESRD concerns chronic dialysis patients (8-22,26-36) and renal transplant recipients (23-25,31); few data are available concerning patients on peritoneal dialysis (36,37). In addition, many of the data points are based on reverse-transcriptase polymerase chain reaction (RT-PCR) analysis; serologic investigations are lacking.
The present report aims to address the epidemiology and clinical significance of GBV-C/HGV infection in a cohort of patients undergoing maintenance peritoneal dialysis. A virologic and serologic analysis is made.
Patients and Methods
Patients
The study included 85 patients (33 women and 52 men) undergoing continuous ambulatory peritoneal dialysis (CAPD) in two dialysis units in the Milan area. The mean age of the patients was 64.2 ± 13 years; 83 patients (97%) were Caucasian, and 2 (3%) were Asian. The median time on dialysis was 29 months (range: 1 – 213 months). The causes of ESRD were chronic glomerulonephritis (n = 27), hypertension and nephrosclerosis (n = 26), polycystic kidney disease (n = 8), diabetic nephropathy (n = 3), interstitial nephritis (n = 5), and renal disease of unknown etiology and others (n = 16). Of 81 patients, 6 (7.4%) underwent regular hemodialysis (HD) before CAPD. The median serum aspartate (AST) and alanine aminotransferase (ALT) levels were 17 U/L (range: 131 – 3 U/L) and 17 U/L (range: 168 – 4 U/L) respectively. The median value of GGT activity was 19 U/L (range: 282 – 6 U/L).
In the control group, we randomly included 136 healthy blood donors attending the blood transfusion unit at the Maggiore Hospital, Policlinico IRCCS, Milan, Italy. All of the donors were tested for anti-E2 GBV-C/HGV antibody, anti-HCV, and HBsAg; half (68/136) were analyzed for GBV-C/HGV viremia by RT-PCR.
Laboratory Measurements
All serum samples were promptly separated and stored at –20 C in aliquots until tests for GBV-C/HGV RNA and anti-E2 GBV-C/HGV antibody were made. A radioimmunoassay (Abbott Laboratories, Abbott Park, IL, U.S.A.) was used to test for HBsAg. Anti-HCV antibody was determined by a third-generation enzyme-linked immunosorbent assay (anti-HCV 3.0 ELISA: Ortho Diagnostic Systems, Raritan, NJ, U.S.A.) that detects antibodies derived from three distinct regions of the HCV genome. All tests were carried out and interpreted strictly in accordance with the manufacturers’ instructions. Spectrophotometry with standard automated analyzers was used to measure AST [also known as serum glutamic oxaloacetic transaminase (SGOT)] and ALT [also known as serum glutamic pyruvic transaminase (SGPT)]. The upper normal limits for AST and ALT were 46 IU/L and 40 IU/L respectively. Gamma glutamyl transpeptidase activity in serum was measured with common analyzers, the normal range being 11 – 50 IU/L.
Gbv-C/Hgv Viremia and Anti-E2 Gbv-C/Hgv Antibody
Extraction of RNA from serum and RT-PCR for GBV-C/HGV were carried out as previously reported (9). The nucleotide sequences were these:
NS5 region (positions 77–101 and 211–188): 5’ CTC TTT GTG GTA GTA GCG GAG AGAT 3’ and 5’ CGA ATG AGT CAG AGG ACG GGG TAT 3’
Region NCR (positions 101–120 and 285–267): 5’ CGC CCA AAA GGT GGT GGA TG 3’ and 5’ CGA CGA GCG TGA CGT CGG G 3’
Antibodies to the envelope protein of GBV-C/HGV (anti-E2) were detected with the immunoassay kit Anti-HGenv (Boehringer Mannheim, Mannheim, Germany). The test was carried out and interpreted strictly in accordance with the manufacturer's instructions.
Statistical Analysis
Serum aminotransferase levels were logarithmically transformed to obtain a normal distribution and then analyzed statistically. Univariate analysis used the Student t-test and the chi-square test with Yates correction, where appropriate. We performed multivariate analysis by a nominal logistic regression model. Age, sex, race, time on dialysis, HBsAg status, anti-HIV and anti-HCV positivity, underlying cause of ESRD, and AST and ALT levels were used as independent variables; positivity for GBV-C/HGV infection was assumed as the dependent variable. Statistical analyses were performed using the program JMP IN (1996: SAS Institute, Cary, NC, USA). A p value less than 0.05 was considered statistically significant.
Results
Table 1 shows the prevalence of subjects positive for HBsAg and anti-HCV in the study and control groups. Table 1 also reports the prevalence of GBV-C/HGV infection as detected by viremia and anti-E2 GBV-C/HGV antibody. In the study group, the frequency of GBV-C/HGV infection was 20% (17/85). Nine patients (10.5%) showed GBV-C/HGV viremia, and 9 (10.5%) showed anti-E2 GBV-C/HGV antibody. Only 1 patient (1.2%) simultaneously showed GBV-C/HGV viremia and anti-E2 GBV-C/HGV antibody. As Table 2 shows, no significant difference was seen between dialysis patients with and without signs of GBV-C/HGV infection on several demographic, clinical, and biochemical features. No significant differences were seen between GBV-C/HGV–positive and GBV-C/HGV–negative patients on CAPD with regard to numerous virologic parameters (Table 3). Table 4 reports the results of the multivariate analysis.
Nominal Logistic Regression Analysis
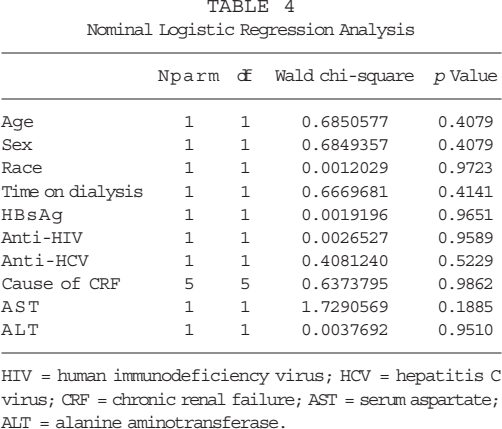
HIV = human immunodeficiency virus; HCV = hepatitis C virus; CRF = chronic renal failure; AST = serum aspartate; ALT = alanine aminotransferase.
Virologic Features of Patients Positive and Negative for GB Virus C/Hepatitis G Virus (GBV-C/HGV)
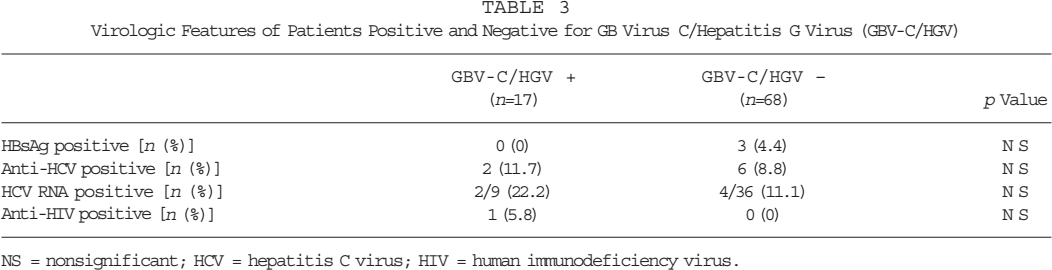
NS = nonsignificant; HCV = hepatitis C virus; HIV = human immunodeficiency virus.
Demographic and Biochemical Features of Patients Positive and Negative for GB Virus C/Hepatitis G Virus (GBV-C/HGV)
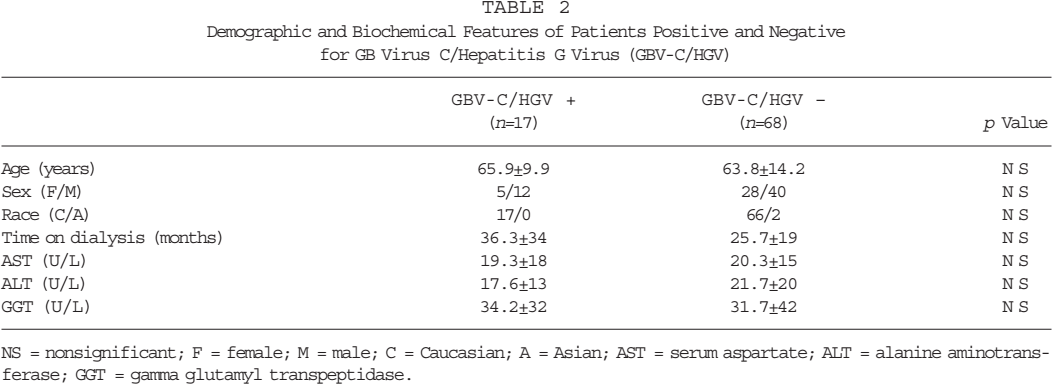
NS = nonsignificant; F = female; M = male; C = Caucasian; A = Asian; AST = serum aspartate; ALT = alanine aminotransferase; GGT = gamma glutamyl transpeptidase.
Hepatotropic Infections in Dialysis and Control Groups
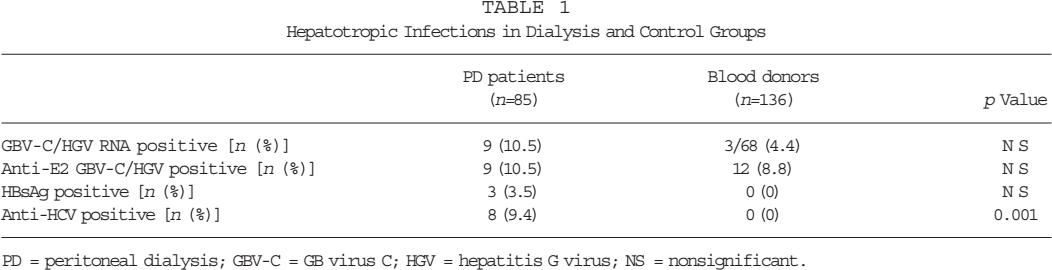
PD = peritoneal dialysis; GBV-C = GB virus C; HGV = hepatitis G virus; NS = nonsignificant.
The history of blood transfusion requirement was assessed in 48 of 85 patients (56%): 24 of the 48 (50%) had received blood transfusions. No significant difference was seen with regard to the frequency of GBV-C/HGV infection between patients with a positive history of transfusions and those without [25% (6/24) vs 20.8% (5/24),p = nonsignificant (NS)].
Discussion
We found a high prevalence (20%) of GBV-C/HGV infection in our series of CAPD patients. A rather high prevalence of GBV-C/HGV infection was also seen in the control group.
Patients on CAPD usually show a lower frequency of anti-HCV antibody as compared with patients undergoing center HD. The Lombardy Dialysis and Transplantation Registry (38), which surveyed 5633 patients undergoing maintenance dialysis in Lombardy, northern Italy, reported during 1998 a mean frequency of anti-HCV antibody of 24.3% (26% in hemodialysis patients and 13% in peritoneal dialysis patients). After implementation of screening of blood for anti-HCV, dialysis patients remained at risk of acquiring HCV only by nosocomial transmission; the risk is clearly higher in HD than in CAPD. By contrast, our investigation demonstrates a high frequency of HCV and GBV-C/HGV infection in patients on peritoneal dialysis. The one previous report on GBV-C/HGV infection in patients on CAPD treatment was made by Huang et al. (37), who also found a high prevalence of GBV-C/HGV infection in their CAPD patients (23.3% positive patients by RT-PCR only).
The high prevalence of GBV-C/HGV infection in our patients on CAPD has unclear mechanisms: no relationship was found between GBV-C/HGV infection and age, sex, race, duration of renal replacement therapy, or co-infection with HIV, HBV, or HCV. We found no relationship between prior history of blood transfusions and GBV-C/HGV infection. [Transfusion requirement appears to be an important risk factor for GBV-C/HGV transmission in HD (8,9,14,18,19,21,32).] Thus, the high spread of GBV-C/HGV among our CAPD patients is probably related to the high frequency of the virus in humans. [In the general population, GBV-C/HGV RNA is found in 2% and HCV RNA only in 0.5% (7).] Additional routes of GBV-C/HGV infection besides parenteral transmission likely exist.
In the present study, only 1 of 9 patients with GBV-C/HGV RNA in serum showed positivity for anti-E2 GBV-C/HGV antibody. That finding supports the initial finding, namely that anti-E2 GBV-C/HGV antibody and GBV-C/HGV viremia are mutually exclusive (39-40). It is possible that the 1 positive patient was going to clear the infection. The possibility of GBV-C/HGV viremia below the detection limit of RT-PCR cannot be excluded. The co-detection of anti-HCV antibody and HCV viremia is frequent in ESRD (41).
No association was seen between AST or ALT and GBV-C/HGV infection. The assessment of liver damage by biochemical tests among dialysis patients may be hampered by the low aminotransferase levels in that population (42,43). Guh and coworkers (43) recommended that the upper limit for AST and ALT levels in HD patients be below 20 UI/L. Detectable HCV RNA in serum by RT-PCR (44) or branched-chain DNA assay (45) is a strong and independent predictor of increased aminotransferase activity in the dialysis population. A recent report had suggested that the combined elevation of GGT and alkaline phosphatase in cryptogenic liver disease might represent a specific feature of the liver tropism of that agent (46). However, serum GGT levels were not significantly higher in GBV-C/HGV–positive patients than in GBV-C/HGV–negative patients in our series.
Some authors have concluded that the association between GBV-C/HGV and hepatitis in humans may be simply an epidemiologic finding with no causative association (47). The term “human orphan flavivirus” (HOFV) has recently been introduced to underline the prematurity of considering that agent in the group of “classical agents” of viral hepatitis (47). That understanding has not been shared by all authors (48). The clinical impact of GBV-C/HGV in humans and in ESRD is under active investigation and awaits further research.
Conclusion
We found a high prevalence of GBV-C/HGV infection both in CAPD patients and in controls. In only 1 patient were GBV-C/HGV viremia and anti-E2 GBV-C/HGV antibody co-detected, suggesting that GBV-C/HGV viremia is usually cleared in the absence of antiviral treatment. No significant link was seen between GBV-C/HGV and liver biochemical tests. The clinical significance of the presence of GBV-C/HGV infection in CAPD patients is still controversial. Prospective studies are in progress.