
Abstract

Icodextrin 7.5%, an iso-osmolar formulation of maltodextrin glucose polymer, is being used increasingly to enhance ultrafiltration during long dwells in continuous ambulatory peritoneal dialysis (CAPD) and automated peritoneal dialysis (APD) patients (1). Except for rare cutaneous hypersensitivity reactions, it is generally safe and well tolerated (2,3).
Recently however, a few cases of mild abdominal pain and sterile chemical peritonitis have been attributed to icodextrin (4-9). These reactions are characterized by mild abdominal discomfort, cloudy effluent only with icodextrin dialysates, dialysate hypercellularity with a predominance of macrophages and sterile cultures, and the absence of systemic symptoms (4-9).
In addition to our previously reported patient (5), we now report eight new cases, determine the prevalence of these reactions, and review all cases previously reported. It is indeed of great importance to recognize these peritoneal reactions secondary to icodextrin in order to avoid unnecessary antibiotic prescription, or even catheter removal, as previously reported (4).
Case Presentations (Table 1)
In our 3 centers, a total of 9 peritoneal dialysis (PD) patients have recently presented with abdominal discomfort and cloudy sterile effluents only with icodextrin. No rash, fever, or other hypersensitivity symptoms were present. Interestingly, all patients affirmed that dialysate progressively cleared during the day, under glucose solutions. Icodextrin had been prescribed for an average of 4.2 months (range 4 weeks to 17 months) before onset of the symptoms. Cell count in the effluent varied from 100 to 2390 WBC/μL, with a predominance of macrophages (range 27% – 82%). In Patient 5, there was a predominance of neutrophils and an excess of eosinophils. Although all dialysate cultures remained sterile, 7 patients were given antibiotics empirically because of suspicion of infectious peritonitis. In Patients 1 – 4, symptoms progressively subsided despite maintenance of icodextrin prescription. In one case (Patient 3), CAPD had to be subsequently interrupted because of the appearance of a pleuroperitoneal communication. In Patients 6 – 9, dialysate progressively cleared despite the maintenance of icodextrin; recurrence of transient cloudy icodextrin dialysates was noticed thereafter. In Patients 5 and 8, icodextrin had to be definitely withdrawn because of recurrence of abdominal pain; however, they remained on CAPD.
Prevalence
In our 3 centers, a total of 104 patients have been given icodextrin. Sterile peritoneal reactions occurred thus in 9/104 (8.7%). This prevalence is probably underestimated because of the absence of clinical symptoms in some patients and the nondetection of cloudy dialysates in some patients. This could be due to the fact that dialysate seems to be cloudy only in icodextrin effluents. The fact that, on APD, the presence of cloudy dialysates is less easily detected might explain the absence of description of these reactions in APD patients.
Literature Review
Few cases of sterile reactions to icodextrin have been reported so far. They are presented in Table 2.
Williams and Foggensteiner reported an episode of sterile peritonitis in 12 of 26 patients receiving single icodextrin exchange overnight an average of 135 (range 8 – 450) days after icodextrin was started (4). These patients typically presented with cloudy dialysate, no abdominal pain, and increased dialysate WBC count. All cultures were negative and there was no evidence of peritoneal or peripheral blood eosinophilia. The first 5 patients were given empirical antibiotherapy: in 2, cloudy dialysate resolved rapidly; one other had the PD catheter removed because of what was called refractory sterile “peritonitis”; and in the remaining 2, that had persistently cloudy dialysates for 7 days, withdrawal of antibiotics and a switch from icodextrin- to glucose-based dialysates led to normalization of the dialysate within 24 – 48 hours. The remaining 7 patients were switched to glucose without antibiotic prescription and the dialysate cleared within 1 or 2 exchanges. No evidence of manufacturing problems or endotoxins could be detected. Rechallenge with icodextrin in 5 patients led to the recurrence of cloudy dialysate within a few days (4).
Case Presentations
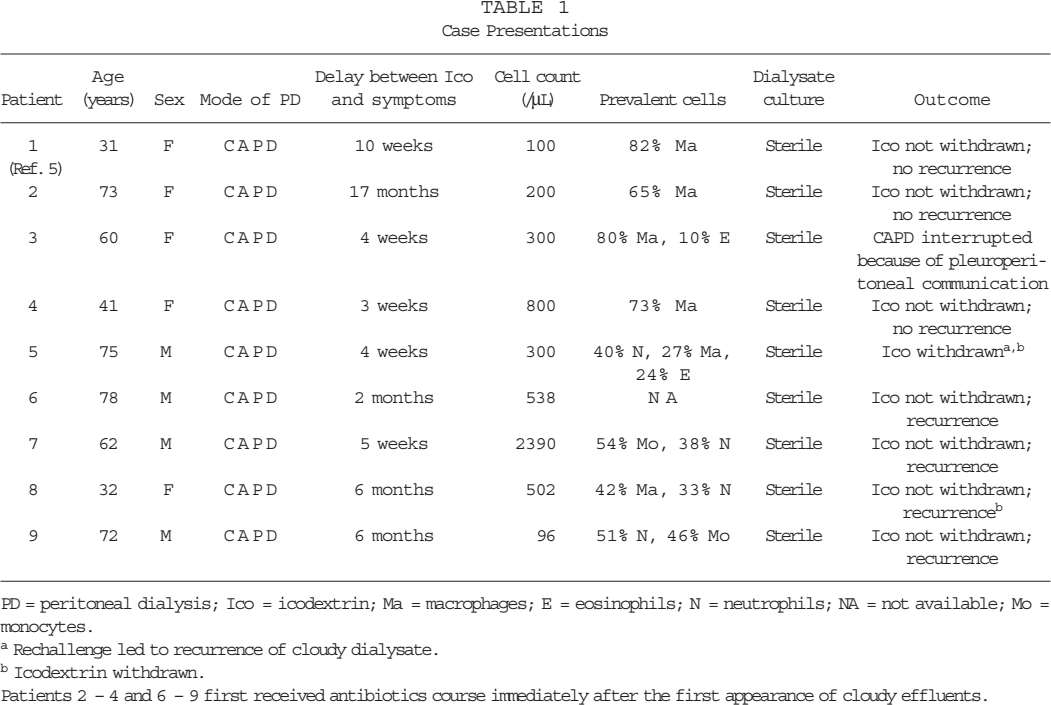
PD = peritoneal dialysis; Ico = icodextrin; Ma = macrophages; E = eosinophils; N = neutrophils; NA = not available; Mo = monocytes.
Rechallenge led to recurrence of cloudy dialysate.
Icodextrin withdrawn.
Patients 2 – 4 and 6 – 9 first received antibiotics course immediately after the first appearance of cloudy effluents.
Literature Review
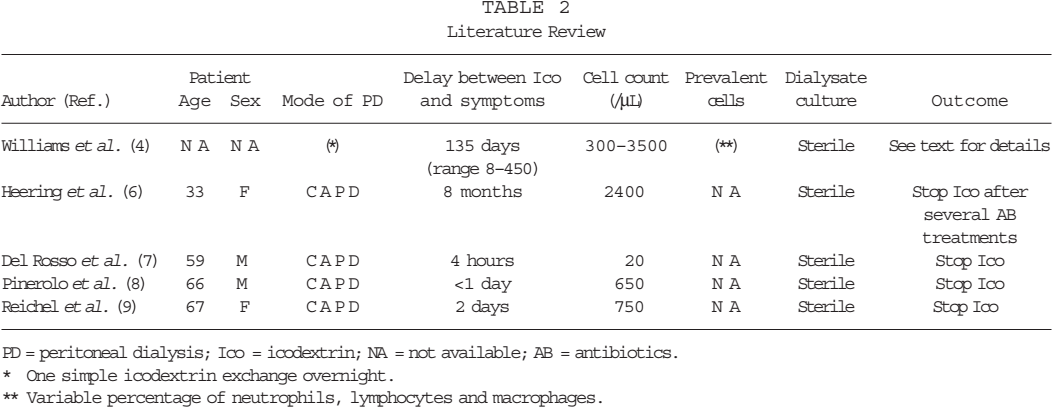
PD = peritoneal dialysis; Ico = icodextrin; NA = not available; AB = antibiotics.
One simple icodextrin exchange overnight.
Variable percentage of neutrophils, lymphocytes and macrophages.
Heering et al. reported a patient on CAPD with symptoms of “peritonitis” 8 months after icodextrin was started (6). Antibiotherapy led to rapid improvement of clinical symptoms, but the peritoneal WBC count remained high. Dialysate fluid was sterile. The antibiotic regime was changed several times, but the WBC count remained high (2400/μL). Icodextrin solution was interrupted a few days after discontinuation of antibiotic, resulting in a decrease in WBC count to 100/μL (6).
Del Rosso et al. reported a 59-year-old CAPD patient who complained of abdominal discomfort 4 hours after a first infusion of icodextrin, followed 3 hours later by chills and hyperthermia (38.3°C); icodextrin was drained out (7). Fluid effluent was sterile and WBC count was only 20/μL. The reaction settled within 1 day and icodextrin was withdrawn. A rechallenge a few months later led to the same reaction (7).
Pinerolo et al. presented a 66-year old CAPD patient who complained of abdominal pain, vomiting, and diarrhea a few hours after a first use of icodextrin, and had elevated WBC in the dialysate (8). With antibiotics, resolution of the symptoms and normalization of dialysate WBC count occurred within 24 and 72 hours, respectively. Dialysate culture was negative. Two months later, icodextrin was again prescribed and 5 hours after infusion, the patient developed the same symptoms: cloudy effluent and dialysate WBC count of 650/μL. Cultures remained negative (8).
Reichel et al. described a 67-year-old CAPD patient treated for Streptococcus agalactiae peritonitis with cefotaxime and gentamicin for 23 days (9). After discharge, icodextrin was initiated. Two days later, he was rehospitalized with cloudy effluent; the dialysate contained 750 WBC/μL. Because cultures were negative, icodextrin was discontinued. The dialysate WBC count quickly returned to normal without antibiotic treatment (9).
Discussion
Few cases of sterile reactions to icodextrin have been described. Delay between the initiation of icodextrin and first symptoms varies among patients, ranging from immediately (7,8) to several months after a first use (6). Patients usually present with mild abdominal pain or discomfort, without rebound or peritonism, fever, rash, or malaise (3,7). Dialysate cell count is usually abnormal, with a predominance of mononuclear cells (4,5). Effluent culture is always, and by definition, sterile.
A diagnosis of peritoneal reaction to icodextrin is of great importance to avoid unnecessary antibiotic prescription, or even catheter removal, as recently reported (4). The majority of the patients reported had indeed been initially diagnosed with infectious peritonitis.
Can these adverse reactions to icodextrin be attributable to the structural similarity between icodextrin and dextran, the latter structure being known to frequently induce anaphylactoid reactions (2)? Icodextrin solution contains molecules with molecular weight varying between 12 000 and 20 000 kDa. Since high molecular weight molecules have been documented to produce a better-sustained ultrafiltration by colloid osmosis (10), is there a tendency to manufacture higher molecular weight icodextrin molecules? A change in the production of icodextrin over time could explain the recent description of these peritoneal reactions despite the availability of icodextrin for more than 6 years. Additional questions have to be raised: First, is there an individual susceptibility? This hypothesis is more likely to explain the recurrence of symptoms in some patients than a potential contamination of the icodextrin bags. The second point deserving consideration is the management of these chemical reactions. Withdrawal of icodextrin may be necessary in cases of severe reactions (7). In such cases, a rechallenge could be hazardous. In cases of mild reactions, icodextrin could be continued, with the hope of a progressive reduction in symptoms as observed in some cases here. However, even if clinically tolerable, what will be the long-term consequences for the peritoneal membrane of recurrent chemical peritonitis under icodextrin? This latter point deserves careful evaluation through longitudinal peritoneal function tests and a peritoneal biopsy for any peritoneal catheter removed from patients that had been given icodextrin.