
Abstract

Editor:
We read with interest the article by Van Vlem et al. (1). Although the hypothesis stated by the authors is very attractive, we feel that major methodological inaccuracies account for the differences found in the different test conditions. In our opinion, two major mistakes have been made:
The premise of the study is that the 13C-octanoic acid breath test, validated in healthy subjects and patients with different gastrointestinal and hepatic diseases and metabolic abnormalities such as diabetes mellitus, is a valid test to be used in patients with severe chronic renal failure, and even in dialysis patients [both hemodialysis (HD) and peritoneal dialysis (PD) patients]. This is only true when “postgastric processing” of the 13 C-octanoic acid (2) is similar in these patients compared with normal subjects. But there are numerous pathophysiological processes present in dialysis patients that may interfere with this “postgastric processing”: (a) Ultrafiltration decreases plasma volume and thereby portal blood flow, hence inducing a shift from hepatic to muscle oxidation of octanoic acid. (b) Ultrafiltration decreases plasma volume and dialysis interferes with the bicarbonate pool. Both factors are very important for the dynamic exchange of 13CO2 with the fast and slow bicarbonate pool and the loss of the 13C marker via feces, urine, ultrafiltrate, and incorporation in the bone. (c) Metabolic acidosis also interferes with different cell functions. Therefore, it cannot be assumed that “postgastric processing” of 13C-octanoic acid is similar in dialysis patients compared with normal volunteers without doing validation studies (e.g., intraduodenal instillation studies of 13 C-octanoic acid in uremic patients with and without ultrafiltration, bicarbonate substitution). Moreover, in severe uremic patients, electrolyte disturbances (especially of cationic electrolytes) may delay gastric emptying since they may interfere with smooth muscle contractility. It was recently shown that a single dose of MgCl2 even in healthy volunteers provokes a dramatic decrease in gastric emptying rate, resulting in hampered protein digestion and lipolysis (3). The interpretation of gastric emptying without measuring (individually different) fluxes of calcium, potassium, and magnesium during dialysis is incorrect. All dialysis patients are subject to a multidrug regime, a lot of which may interfere with gastric emptying (e.g., beta-blockers, tranquilizers, sedatives, benzodiazepines), accumulate, are not metabolized after an overnight fast, and are dialyzed only partially.
The most obvious methodological flaw, however, is that the authors did not check their dialysis fluids for background enrichment of 13CO2. The advantage of 14C-labeled breath tests is that, in nature, no background 14C is present in the environment; this is not the case for 13C, since it is incorporated in many of plants by photosynthesis. Therefore, a lot of substrates are “contaminated” with 13C and, when using 13C-labeled breath tests, interference has to be checked from natural 13C enrichment of the test meal used (4), but also by other substances given before or during the breath test. A well-known exclusion criterion for 13C-labeled breath tests is concurrent intravenous solutions of glucose or bicarbonate. Also, the solutions used for HD (glucose-containing) and PD may be differently enriched, according to the substrates of glucose, amino acids, etc. used, and this may vary seasonally according to the crops used for making these substrates. This background 13C enrichment should be subtracted from the 13CO2 excretion curve obtained from the 13C-octanoic acid used to dope the test meal. We noted that 13CO2 excretion in the breath of PD patients not performing a 13C-octanoic acid breath test increased significantly after intraperitoneal administration of PD solutions (both glucose- and icodextrin-containing). This bias is influenced not only by the substrate used (e.g., glucose 1.36% vs icodextrin), but also by the permeability of the membrane (e.g., high vs low transporter) and dwell time. To quantify this bias on the gastric emptying parameters of a 13CO2 excretion curve obtained after a 13C-octanoic acid breath test in traditional standard test conditions, we added the mean 13C background enrichment of one 4-hour dwell of glucose 1.36% measured in 3 PD patients to a 13CO2 excretion curve of 2 normal subjects (Figure 1). As noted, there is a shift of the 13CO2 excretion curve, mainly in the descending part of the curve, that causes a substantial delay in the half emptying time (t½ shifts from 72 to 98 and from 79 to 118 minutes) and is remarkably similar to the differences measured by the authors in different articles (1,5,6). Therefore, we are convinced that the 13 C-octanoic acid breath test is not a valid test in HD and PD settings, and that the differences seen in this and previous reports (1,5,6) merely reflect differences in fluxes of 13 C-enriched substrates rather than differences in gastric emptying.
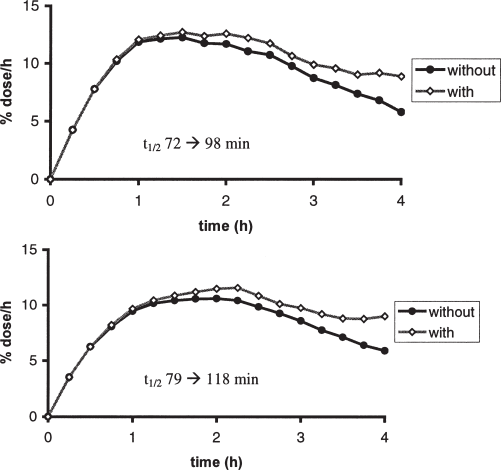
Effect of the addition of the mean 13C background of a 4-hour dwell of 2 L glucose 1.36% in 3 peritoneal dialysis patients on the 13CO 2 excretion curve in 2 normal healthy volunteers.
Part of the problems discussed in both paragraphs may be elucidated by showing 13CO2 excretion curves and individual gastric emptying data of several gastric emptying parameters (not only half emptying time, but also lag phase, gastric emptying coefficient). However, the addition of multiple interferences (see item 1) may be the cause of the wide variability noted in the half emptying time given by the authors.