
Abstract
← Background
In the first half of the year 2001, an unusually large number of culture-negative peritonitis episodes occurred in Center A. One patient noticed that his culture-negative antibiotic-resistant peritonitis promptly cleared after inadvertently stopping the use of icodextrin-containing dialysate, but recurred immediately after using icodextrin again. This observation led to the recognition of eight contemporaneous cases of icodextrin-induced culture-negative peritonitis in Center A, and identification of three additional cases in Center B.
← Design
Case studies in 12 patients.
← Setting
Peritoneal dialysis unit of a university hospital and an affiliated unit (Center A), and a second university hospital (Center B).
← Patients
12 patients on peritoneal dialysis presenting with culture-negative peritonitis.
← Results
At presentation, abdominal pain was absent or mild and dialysate leukocyte counts were moderately elevated (approximately 100 – 1500 cells/mm3). Differentiation of the dialysate leukocytes showed a low fraction of neutrophils (approximately 35%). In eight cases, the evidence that the peritonitis was caused by icodextrin was very strong (the clinical picture and laboratory results mentioned above, unresponsiveness to antibiotic therapy, cure after withdrawal of icodextrin, relapse after rechallenge); in 3 patients, the evidence was strong (as in the cases mentioned above, but no rechallenge was performed). Stopping icodextrin promptly relieved the symptoms and normalized the dialysate leukocyte counts. After rechallenge, a relapse invariably occurred, usually within a few days. In one case, the evidence was circumstantial.
← Conclusion
Our findings are compatible with icodextrin-induced peritonitis. This entity is characterized by mild abdominal pain at presentation, a moderate dialysate leukocytosis with a low fraction of neutrophils in the differential count, and resistance to antibiotic treatment. Speculations about the pathogenesis of this type of peritonitis include chemical peritonitis due to a contaminating substance or hypersensitivity to icodextrin.
Methods
Peritoneal Dialysis Therapy
Patients were treated in the dialysis unit of the University Medical Centre Utrecht and in the affiliated dialysis unit of the Dianet Foundation Utrecht (Center A), or in the dialysis unit of the University Hospital “Dijkzigt” in Rotterdam (Center B). They used the twin-bag system (Baxter Healthcare, Deerfield, Illinois, USA) when on continuous ambulatory peritoneal dialysis (CAPD). Patients on continuous cycling peritoneal dialysis (CCPD) used the HomeChoice cycler from Baxter Healthcare. The regular dialysate was glucose-based (Dianeal PD-1 or PD-4; Baxter Healthcare SA, Castlebar, Ireland). The icodextrin 7.5% solution (Extraneal; Baxter Healthcare SA) was used in patients with poor ultrafiltration during the long dwells, or as an alternative for glucose-containing solutions in patients with diabetes mellitus or marked weight gain.
Diagnosis and Treatment of Peritonitis
In Center A, peritonitis is diagnosed when two of the following three items are present: abdominal pain, cloudy dialysate, and a positive dialysate culture. A dialysate leukocyte count of more than 100 cells/mm3 is considered elevated. In Center B, peritonitis is diagnosed when both of the following items are present: dialysate leukocyte count above 100 cells/mm3 (> 50% neutrophils on differential) and a positive dialysate culture. Peritonitis treatment in Center A consists of intraperitoneal (IP) administration of cephalothin in patients less than 40 years old. In patients more than 40 years old, PD is temporarily interrupted and meropenem is given intravenously (IV) (500 mg/day) in addition to intracatheter administration in a small volume of saline (125 mg in 25 mL NaCl 0.9%). Depending on the culture results, PD is resumed with IP cephalothin (skin organisms or negative culture) or PD is interrupted for another week while continuing meropenem treatment (enteral organisms). The rationale of this protocol is discussed elsewhere (4). In Center B, peritonitis is treated with vancomycin 2000 mg IP every 5 to 7 days during 2 to 3 weeks, and ceftazidime 125 mg/L in each bag.
Culture Techniques
In Center A, peritoneal dialysate is collected in blood culture bottles (BacT/Alert; Organon Teknika, Durham, North Carolina, USA). Specimens are cultured for 7 days. Negative bottles are subcultured on rich media for fastidious organisms and fungi. Positive bottles undergo Gram staining, subculture on appropriate media, and identification of cultured bacteria and susceptibility testing, in addition to being subcultured on SDA media for fungi. In 3 patients, a broad-range bacterial polymerase chain reaction (PCR) was performed on dialysate to search for bacterial DNA.
In Center B, peritoneal dialysate is collected in blood culture bottles (Bactec Plus, aerobic and anaerobic; Becton, Dickinson and Co., Sparks, Maryland, USA). Specimens are cultured for 5 days. Positive bottles undergo Gram staining and are subcultured on appropriate media for identification of cultured bacteria and susceptibility testing.
Results
Characteristics of patients with sterile peritonitis are shown in Table 1. All except Patients 9 and 12 had used icodextrin for more than 6 months. Details of peritonitis episodes are reported in Table 2. Dialysate leukocyte counts and differentiation of the leukocytes at presentation are shown in Figure 1. Figure 2 shows changes in the dialysate leukocyte count after stopping icodextrin when this was studied in detail.
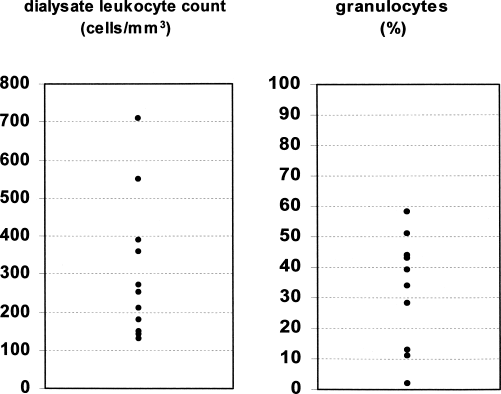
Dialysate leukocyte counts and differentiation in patients with icodextrin-induced peritonitis. For the sake of clarity, the highest dialysate leukocyte count of 1800 cells/mm3, observed in Patient 3, was omitted from the graph.
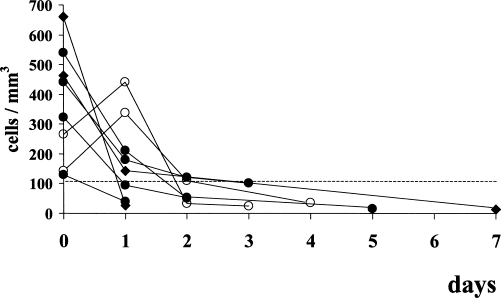
Time course of the fall in dialysate leukocyte count after discontinuation of icodextrin on eight occasions. The open circles indicate Patients 5 and 6, who did not receive antibiotics at presentation at all but who were treated by stopping icodextrin alone. In these patients, the dialysate leukocyte count increased further 1 day later, but then fell to normal values. The dotted line indicates the upper limit of normal of the dialysate leukocyte count.
Case Characteristics
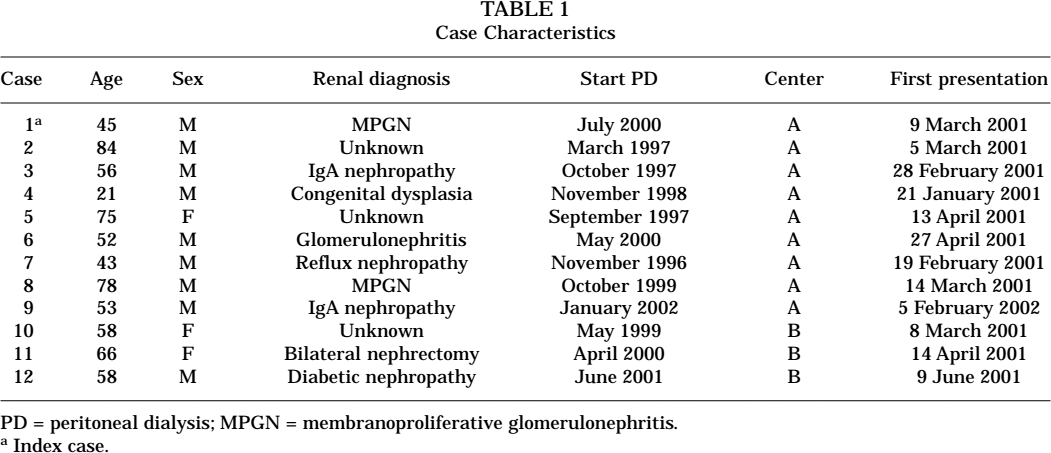
PD = peritoneal dialysis; MPGN = membranoproliferative glomerulonephritis.
Index case.
Characteristics of Icodextrin-Related Peritonitis Episodes
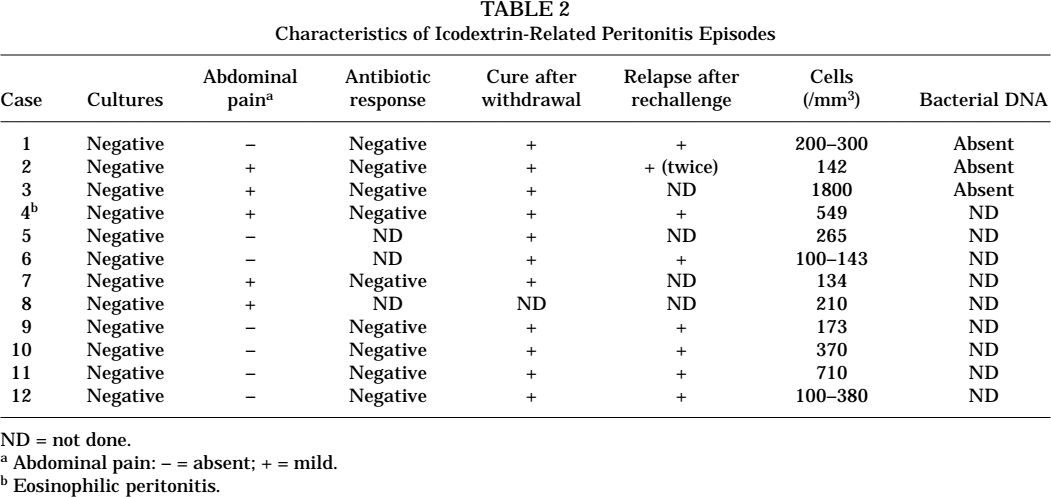
ND = not done.
Abdominal pain: – = absent; + = mild.
Eosinophilic peritonitis.
Case 1
The index case presented with cloudy dialysate without abdominal pain. Cultures were negative and the peritonitis did not respond to antibiotics. Later, abdominal pain occurred and the patient was admitted. Antibiotics were switched and the patient seemed to improve. For unknown reasons, however, icodextrin was discontinued during admission and after discharge. Several days after discharge (dialysate leukocyte count < 100/mm3), the patient started using icodextrin again. Four days later, a relapse of his peritonitis was documented (dialysate leukocyte count 500– 1000/mm 3). The patient then suggested that his peritonitis was caused by icodextrin. After stopping icodextrin, the dialysate became clear and the dialysate leukocyte count fell to 10/mm3. He refused another rechallenge with icodextrin.
Case 2
The dialysate leukocyte counts for this patient are shown in Figure 3. The antibiotic regimen was changed twice but dialysate leukocytosis and abdominal pain persisted. All cultures remained negative. Because Case 1 suggested the possibility of icodextrin-induced peritonitis, icodextrin was stopped. One day later, the abdominal discomfort disappeared and the dialysate leukocyte count subsequently normalized. Rechallenge with icodextrin was performed twice and on both occasions abdominal pain and dialysate cloudiness reappeared.
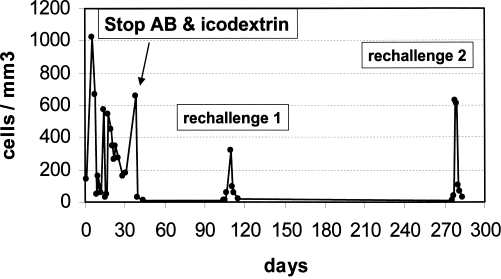
Changes in dialysate leukocyte count in Patient 2. Different antibiotics were given from day 1 to day 40. A first rechallenge with icodextrin took place on day 106, after obtaining baseline leukocyte counts on the previous 2 days; rechallenge promptly resulted in an increased leukocyte count. A second rechallenge was performed on day 277, with the same result.
Case 3
In this patient, the dialysate leukocyte count at presentation was more elevated (1800/mm3) than in the other cases. His culture-negative antibiotic-resistant peritonitis was cured by stopping icodextrin. No rechallenge was performed.
Case 4
This patient was the only one with eosinophilic peritonitis (approximately 90% of the dialysate leukocytes were eosinophilic granulocytes). His antibiotic-resistant peritonitis episode cleared after stopping icodextrin. Eosinophilic peritonitis recurred after rechallenge with icodextrin.
Case 5
In this patient, a tentative diagnosis of icodextrin-induced peritonitis was made at presentation and no antibiotics were given. Icodextrin was discontinued and the dialysate leukocyte count normalized. Rechallenge with icodextrin could not be performed because the patient died 1 month later due to an unrelated condition.
Case 6
A tentative diagnosis of icodextrin-induced peritonitis was made at presentation and no antibiotics were given. The peritonitis cleared rapidly after withdrawal of icodextrin. Two weeks after reintroduction of icodextrin, the patient was admitted with cloudy dialysate (leukocyte count 202/mm3, 39% neutrophils) and severe abdominal pain. Because he appeared ill, bacterial peritonitis was considered and antibiotic therapy was started. A skin rash developed during meropenem treatment. After switching to ciprofloxacin, he developed severe granulocytopenia and died from sepsis 5 weeks later. All initial dialysate cultures remained negative. In retrospect, this patient probably had a relapse of icodextrin-induced peritonitis.
Case 7
This patient had a culture-negative peritonitis with a low initial dialysate leukocyte count and minimal abdominal pain. The leukocyte count remained slightly elevated despite antibiotic therapy. The antibiotic was switched and the peritonitis appeared to subside. Later, however, this patient reported that he had experienced several episodes of cloudy dialysate and mild abdominal pain after the initial episode. Because it had come to his attention that we considered the possibility of icodextrin-induced peritonitis, he stopped using icodextrin. After this, intermittent cloudy dialysate and abdominal pain disappeared. In retrospect, this patient probably had icodextrin-induced sterile peritonitis. He refused a rechallenge with icodextrin.
Case 8
This patient reported on previous occasions that his dialysate was sometimes slightly cloudy. The dialysate leukocyte count was indeed found to be elevated once (210/mm3, culture negative) but was normal again several days later. No specific measures were taken. Several months later, he was admitted with mild abdominal pain and paralytic ileus. Although the dialysate leukocyte count was 180/mm3, the diagnosis “peritonitis” was not considered and no antibiotics were given. Ischemic bowel disease was suspected and a laparotomy was performed, but no abnormalities were found. He died suddenly 4 days after surgery. In retrospect, this patient probably also had icodextrin-induced sterile peritonitis.
Case 9
This man noticed cloudy effluents almost immediately after he started using icodextrin. He had no abdominal pain. No antibiotics were given. Because of poor ultrafiltration during long dwells with glucose-based dialysate, he continued to use icodextrin. One month later, however, he reported abdominal pain and the leukocyte count rose to 1180/mm3. Icodextrin was stopped, the abdominal pain disappeared, and the leukocyte count normalized. Rechallenge with icodextrin induced a relapse of sterile peritonitis.
Case 10
This patient, treated in Center B, had cloudy dialysate without abdominal pain for several months. A course of antibiotics had no effect. Cultures were negative and icodextrin was continued. After recognition of the entity of icodextrin-induced peritonitis in Center A, icodextrin was stopped, after which the dialysate leukocyte count normalized. Rechallenge with icodextrin increased the dialysate leukocyte count to 480/mm3 (7% neutrophils).
Case 11
This patient presented with cloudy dialysate. The dialysate leukocyte count remained elevated despite antibiotic therapy. Severe abdominal pain developed, which prompted removal of the peritoneal catheter. After temporary hemodialysis, a new catheter was implanted and CAPD was resumed using a schedule including icodextrin. After this, the leukocyte counts were elevated again for the next month and cultures were all sterile. When the abdominal pain became severe again, antibiotics were given without effect. After stopping icodextrin, however, the dialysate leukocyte count normalized and abdominal pain disappeared. Rechallenge with icodextrin induced a relapse of sterile peritonitis.
Case 12
This patient started icodextrin 4 days after commencing CAPD. During the next 2 months, the leukocyte counts were determined on 4 occasions. They ranged between 100 and 380/mm3 (13% neutrophils). Abdominal pain was absent and cultures remained negative. Later, however, mild abdominal pain developed, which prompted antibiotic therapy, but the dialysate leukocyte count remained elevated. It normalized only after stopping icodextrin. Repeat exposure to icodextrin induced a relapse of culture-negative peritonitis.
Discussion
We report 12 cases of culture-negative peritonitis that were related to the use of icodextrin-containing dialysate in patients on PD. Typical were abdominal pain that was usually mild or sometimes even absent and a relatively low dialysate leukocyte count without a predominance of neutrophilic granulocytes. The course was undulating with intermittent abdominal pain and dialysate cloudiness without a consistent response to antibiotics (see Figure 3). Stopping icodextrin led to resolution of the peritonitis within days (Figure 2), whereas a relapse was invariably induced after rechallenge. The absence of positive dialysate cultures, the failure to detect bacterial DNA by broad-range bacterial PCR (3 patients), and the unresponsiveness to antibiotics virtually excluded infectious causes.
Although cutaneous adverse effects of icodextrin have been well described (5-9), reports on peritoneal reactions to this dialysate are scarce. In 1999, Pinerolo et al. described a patient that developed abdominal pain and dialysate leukocytosis after his very first dwell with icodextrin-containing dialysate (10). Dialysate cultures were negative and the dialysate leukocyte count was mildly elevated (650/mm3). Symptoms disappeared within 24 hours after icodextrin infusion and the dialysate leukocyte count normalized after 72 hours. Re-exposure to icodextrin induced the same abnormalities, again during the first dwell. Del Rosso et al. reported a similar case (11). These cases, in which peritonitis appeared after the first contact with icodextrin, are compatible with an acute icodextrin-induced chemical peritonitis. Montagnac et al. reported a possible case of icodextrin-related sterile peritonitis in a patient on long-term icodextrin therapy (12), but interpretation of this case is difficult because extensive intra-abdominal pathology was present in the patient described in this report. More recently, Heering et al. (13) and Reichel et al. (14) each reported a case of culture-negative peritonitis in patients several months on icodextrin. In both cases, dialysate leukocytosis disappeared after stopping icodextrin and appeared again after rechallenge. As in our cases, none of the cases reported above were accompanied by skin abnormalities.
Most cases of culture-negative peritonitis in our patients on icodextrin clustered in the first half of 2001 (see Table 1). Only one new case of culture-negative peritonitis was observed beyond July 2001. This strongly suggests that some transient change in the composition of the icodextrin solutions supplied by the manufacturer during this period caused chemical irritation of the peritoneum. Outbreaks of sterile peritonitis that were attributed to dialysate contamination by either endotoxin (2) or acetaldehyde (3), which could be traced to specific dialysate lots, have indeed been reported. At the consumer level, we could not find an obvious relation between batch numbers and the occurrence of sterile peritonitis, but at the level of the producer, this is still under investigation.
The lack of new cases of icodextrin-related peritonitis may, of course, also be due to the fact that all patients apparently at risk of developing this complication stopped using icodextrin. Hence, causes other than direct toxicity of components of the icodextrin-containing dialysate should be considered. Hypersensitivity to icodextrin was suggested to cause cutaneous reactions to icodextrin but direct proof is lacking (9). We have not performed additional studies that could clarify whether hypersensitivity played a role in causing icodextrin-induced peritonitis. One of our patients (Case 4) had eosinophilic peritonitis, and another (Case 1) had transient blood eosinophilia, suggesting that type I hypersensitivity could have played a role in these patients. Interestingly, Heering et al. showed that icodextrin in high concentrations induced “lymphocyte stimulation” in vitro in lymphocytes of their patient, and suggested that peritoneal immunocompetent cells could be activated by icodextrin (13).
Some patients received vancomycin during some time of their treatment. This agent has been reported to cause chemical peritonitis after IP administration (15). It is unlikely that this drug was the cause of peritonitis in our cases. None of the patients that presented with culture-negative peritonitis was recently exposed to vancomycin. Moreover, in some patients, the peritonitis cleared after stopping icodextrin while they still received vancomycin.
We suggest that the possibility of icodextrin-induced peritonitis should be considered in patients on PD that present with peritonitis and that use icodextrin, particularly when abdominal pain is mild and the leukocyte count is relatively low. However, dialysate leukocytosis is not always very pronounced in the first bag drained, even in patients with proven bacterial peritonitis. Hence, it is always prudent to investigate dialysate from one or more subsequent exchanges before concluding that the dialysate leukocyte count is indeed only moderately elevated. Another helpful feature is that the proportion of neutrophilic granulocytes in the differential count is relatively low: in our series, usually approximately 30% (range 2%– 58%). This is below the figure of 50%, which is considered diagnostic of bacterial and fungal peritonitis (16). Note, however, that in our experience the proportion of neutrophilic granulocytes is usually well over 80%– 85% in cases of proven bacterial peritonitis.
Although icodextrin-induced peritonitis often was clinically mild, chronic peritoneal inflammation may nevertheless have detrimental effects on the long-term function and integrity of the peritoneal membrane. In addition, recognition of icodextrin-induced peritonitis is important because it can protect patients from the adverse effects of unneeded antibiotic treatment (Case 6), surgery (Case 8), and catheter removal (Case 11).