
Abstract

A limiting factor in long-term peritoneal dialysis (PD) is the progressive reduction in the dialytic efficiency of the peritoneal membrane (1). Indeed, histological studies in both humans and animals reveal that chronic PD results in fibrosis of the peritoneal membrane (2,3). In a short-term study in continuous ambulatory peritoneal dialysis (CAPD) patients, we demonstrated that intraperitoneal administration of a glycosaminoglycan, sulodexide, improves the efficiency of PD (4). Furthermore, in an experimental model of peritoneal fibrosis, the subcutaneous administration of sulodexide partly restored/prevented morphological and functional derangement of the peritoneum (5).
Sulodexide is also available as an oral formulation that, if effective, would maximize patients’ compliance and reduce microbiological risk. This small explorative open trial was carried out (1) to investigate whether sulodexide by oral administration is effective on peritoneal permeability in PD patients, (2) to investigate the effect of sulodexide on peritoneal interleukins because of their role in peritoneal fibrogenesis and defenses, and (3) as a dose- and range-finding study in order to select sulodexide dosage for larger controlled trials.
Patients and Methods
Six patients (3 women, age 46 – 65 years) were randomly selected from patients on long-term CAPD (49 – 62 months) that had not had more than one peritonitis episode and none in the 6 months before the study. End-stage renal failure was due to chronic glomerulonephritis in all cases. No patients had diabetes mellitus, liver insufficiency, thrombocytopenia, or known sensitivity to glycosaminoglycans and/or heparin. All patients gave written informed consent to participate.
Throughout the study, the scheduled dialysis program consisted of four 2000-mL bags containing (mmol/L) sodium 136.0, potassium 2.0, chloride 104.7, calcium 1.75, magnesium 0.38, lactate 37.5, and glucose 83.3, except in the nightly bag, which contained 111.1 mmol/L glucose.
After a 30-day run-in period, patients assumed orally, at monthly increasing dosages, sulodexide (Vessel 2 forte, 25 mg/capsule; Alfa Wassermann SpA, Bologna, Italy), a highly purified preparation containing an 80% endogenous-like, fast-moving heparin fraction (iduronyl-glycosaminoglycan sulfate) with a high affinity for antithrombin, and a 20% dermatan sulfate fraction, with affinity for heparin cofactor 2. The duration of the study was 5 months and patients assumed sulodexide 25 mg/day (one capsule in the morning), followed at monthly intervals by 50 mg (1 capsule every 12 hours), 75 mg (2 + 1 capsules), 100 mg (2 + 2 capsules), and, during the last 30 days, 125 mg (3 + 2 capsules) for 30 days each.
During the 5-month intervention period, oral fluid and protein intake (1.2 g/kg body weight) and every other drug treatment were kept constant. Blood for laboratory evaluations was taken after an overnight fast following discharge of the nightly bag. Patients’ coagulation, hydration status, blood pressure, and residual renal function (by creatinine clearance) were monitored monthly. Peritoneal fluid samples were collected from all dialysis exchanges on 2 consecutive days immediately before starting the intervention period (T0) and on the last 2 days of every 30-day dosage interval. Net ultrafiltration was determined by weight as the difference between drained and infused fluid volume. Samples of the drained dialysate were stored at –80°C until use.
Urea was measured using the urease enzymatic method, creatinine using creatininase, glucose using glucose oxidase, and albumin by turbidimetry using a specific anti-albumin antibody. The dialysate-to-plasma (D/P) ratios for urea, creatinine, and albumin, and the glucose drained dialysate-to-unused fluid (D/D0) concentration ratio were calculated. In 4 patients, in drained dialysate samples collected in 2 days at T0 and at the end of the 50- and 100-mg sulodexide dosage periods, interleukin (IL)-1β, IL-6, and IL-8 were determined using a commercial kit (Immulite; DPC, Los Angeles, California, USA).
Data are expressed on a per day basis calculated as mean and SD of values obtained on 2 consecutive days. Statistical analysis was performed using the analysis of variance for repeated measures, and the Newman–Keuls test was used for multiple comparisons.
Results and Discussion
This study demonstrates that sulodexide is able to ameliorate peritoneal efficiency also by the oral administration of the agent. Actually, as shown in Table 1, it induced a significant increase in D/P urea, starting from the lower dosage (approximately 10% more, p = 0.0174), but the highest increase was observed at the end of the 125 mg/day dosage (T5) (approximately 20% more, p = 0.003); D/P creatinine also increased during sulodexide treatment, but progressively reached the maximal value at T5 (approximately 20% more, p = 0.009). In both cases, no evidence of plateau was observed, suggesting that the maximal effect was probably not reached. Sulodexide induced a significant decrease in peritoneal albumin loss, starting from the dosage of 75 mg/day, as noticed by the reduction in D/P albumin (approximately 50% less, p < 0.05), apparently reaching a plateau phase. On the contrary, there was no statistically significant effect of the drug on ultrafiltration or D/D0 glucose, although an increasing trend could be observed for the glucose gradient dissipation ratio D/D0 (p < 0.06).
Effect of Increasing Dosages of Oral Sulodexide on Peritoneal Function Parameters and Interleukins
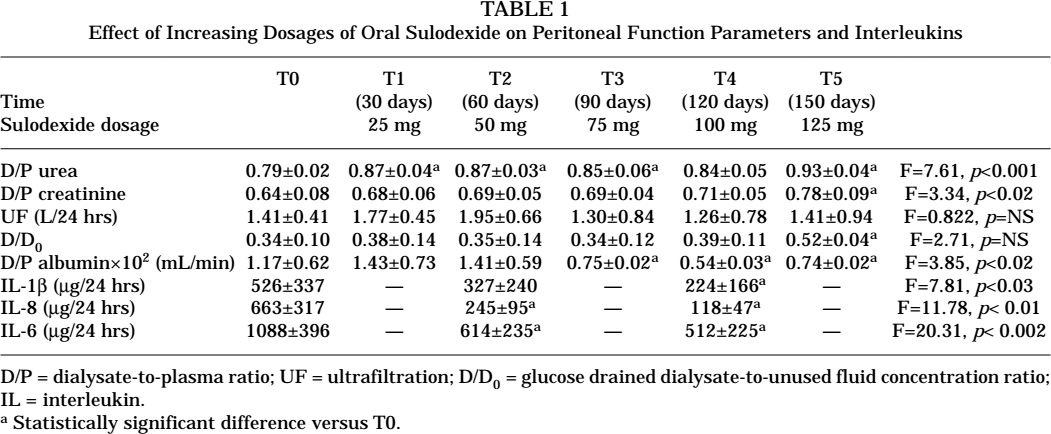
D/P = dialysate-to-plasma ratio; UF = ultrafiltration; D/D0 = glucose drained dialysate-to-unused fluid concentration ratio;
IL = interleukin.
Statistically significant difference versus T0.
Although we did not plan to have either a control group or a laboratory control after a fixed washout period, when we looked for values of peritoneal function in the regular follow-up of the investigated patients (on average 6 – 8 weeks after the trial end), peritoneal parameters had come back to their baseline or were intermediate between the T0 and the T5 values, thus suggesting that the above variations were actually due to the sulodexide treatment.
It is not easy to fit in a common framework all the peritoneal transport data obtained in this study. While it is obvious that sulodexide affects permeability to urea and creatinine in a parallel manner, it is puzzling why permeability to glucose, another small molecule, does not reflect similar changes and, on the contrary, discloses an opposite, albeit not-significant trend. Lack of effect of intraperitoneal glycosaminoglycans (namely, heparin) on glucose peritoneal absorption has recently also been demonstrated in a nonuremic rat model of PD (6). Since specific mechanisms [i.e., a glucose-transporter-1 (GLUT-1)–mediated transport] may be involved in glucose transport in the peritoneum, we speculate that sulodexide has a peculiar effect on them, and thus a distinct effect on the dissipation of the glucose gradient. Indeed, it has been shown in mesangial cell culture that sulodexide downregulates the synthesis of GLUT-1 (Cha DR, Korea; personal communication). Since it is known that, at the usual glucose concentrations, GLUT-1 works at its maximal rate, reduction of the number of GLUT-1 transporters may reduce glucose transport through cells, possibly explaining our findings.
In general, although some improvement could be seen as early as the end of the first dosage, it seems that high sulodexide dosages (> 50 mg/day) are probably necessary to induce clinically significant variations in most peritoneal functions. This is in line with the recent observation obtained in the Di.N.A.S. Trial in patients with diabetic nephropathy in which only patients treated with doses higher than 50 mg/day oral sulodexide had a significant reduction in albuminuria (7). Interestingly, in the Di.N.A.S. Trial, a clear relationship between the effect on albuminuria and the duration of sulodexide treatment was obvious. Indeed the higher prevalence of responders was observed after the 4-month treatment, following a progressive increase that started from the first month of sulodexide treatment. Due to the present experimental design, we cannot dissect the role of sulodexide dosage over the duration of treatment in determining peritoneal permeability modifications, but we deem that the latter also had some impact.
Both experimental studies and the Di.N.A.S. Trial give direct and indirect evidence respectively that glycosaminoglycans, namely sulodexide, exert a remodeling activity on the extracellular matrix and basement membrane. On the other hand, in an experimental model of peritoneal fibrosis, we demonstrated that this agent has a protective effect on both structural and functional peritoneal alterations (5). Thus, sulodexide contributes favorably to remodeling a deranged peritoneal membrane. We speculate that the administration of sulodexide to PD patients interferes with mechanisms involved in peritoneal derangement and promotes favorable remodeling of the peritoneal membrane. Since this process obviously has a lingering effect, it may require a longer duration than that used in the present study to determine the full appearance of all expected peritoneal functional modifications (i.e., changes in D/D0 and ultrafiltration). Furthermore, since remodeling may have a different impact on the cell compartment (which is mostly relevant in small molecule permeability) and on the extracellular matrix compartment [which is mostly relevant in large anionic molecule (protein) permeability], it is not surprising to observe a different time course of the sulodexide activity on different peritoneal permeability parameters, namely D/P albumin versus D/Ps of small molecules.
With reference to the remodeling activity of sulodexide, the effect of the drug on cytokines is interesting. Actually, a statistically significant and dose-dependent reduction of IL-6, IL-8, and IL-1β in the dialysis fluid was induced by sulodexide (Table 1). Interleukin-1β and IL-6 are known to induce collagen biosynthesis and fibroblast/mesangial cell proliferation (8,9), which strongly supports a role for these cytokines in the sclerogenic peritoneal response to chronic inflammatory stimuli. Interleukin-1β is also a potent inflammatory cytokine that orchestrates an inflammatory response to a number of acute and chronic stimuli (10,11). Therefore, the activities of sulodexide on ILs might be important in explaining the functional effects observed in PD patients during oral treatment with this agent.
On the other hand, the inhibition of IL by sulodexide might, in theory, favor peritonitis or worsen the course of peritonitis, the very serious complication of PD. We do not have any evidence whether this risk is real rather than theoretical. What we can say is that, in our limited and short-term experience with the present investigation, but particularly in the previous one in which the probably more risky intraperitoneal administration of sulodexide was employed (16 patients, 1 month treatment) (4), there were no peritonitis episodes. No other adverse effect was observed. In particular, the patients’ hydration status, residual renal function, blood pressure, and coagulation indices remained constant during the study (data not shown), and the patients’ ordinary therapy (diuretics, antihypertensive agents, etc.) did not require changes. No patients had coagulation disorders, hemorrhages, or side effects throughout the study.
In conclusion, this study shows that oral treatment with sulodexide in uremic patients on long-term CAPD improves some functional peritoneal membrane parameters. Whether sulodexide therapy may be a strategy effective in stopping peritoneal dialytic failure needs to be demonstrated by larger, controlled long-term trials. The present study suggests that higher dosages of sulodexide are probably necessary, and that 200 mg/day could be more appropriate for a systemic effect, as in the Di.N.A.S. study in a different clinical condition (7).
Footnotes
Acknowledgment
We thank Dr. A. Budakovic for help in the statistical evaluation of data.