
Abstract
Objective
We investigated the clinical condition and complications of patients on peritoneal dialysis (PD) and on hemodialysis (HD) for more than 12 years.
Design
This retrospective review was carried out in the renal unit of the Tung Wah Hospital, Hong Kong.
Patients and Methods
Of 103 HD and 341 PD patients who started dialysis before 1990, 14 HD and 22 PD patients were dialyzed for more than 12 years. We evaluated basic demography at the 12th year of dialysis and at the most recent follow-up, and assessed the prevalence of cardiovascular disease, bone disease, dialysis-related amyloidosis (DRA), and acquired cystic disease (ACD). Outcomes and mortality were recorded.
Results
The 36 patients in the study included 22 women and 14 men. The PD patients were older (p = 0.021) and had lower levels of serum phosphate and calcium × phosphate product. Only 3 patients were diabetic. Cardiovascular disease was present in 30 patients (83.3%), the most common types being ischemic heart disease (IHD, n = 11) and left ventricular hypertrophy (LVH, n = 22). Symptomatic DRA was found in 13 patients (36.1%), more commonly in the HD group (p = 0.014). Bone disease was present in 32 patients (88.9%), with parathyroidectomy being more frequently performed in the PD patients (p = 0.048). Symptomatic ACD occurred in 5 patients (13.9%). At the most recent follow-up, 26 patients were still on dialysis, 3 patients had undergone renal transplantation, and 7 patients had died, the causes of death being sudden death (n = 3), cerebrovascular accident (n = 1), chest infection (n = 2), and peritonitis (n = 1). Patient survival was similar in the PD and HD groups. Age at commencement of dialysis predicted mortality (p = 0.012), but mode of dialysis, sex, and presence of diabetes mellitus did not.
Conclusions
Long-term survival is possible for both dialysis modalities (PD and HD), particularly for young, non diabetic patients. Symptomatic DRA is less common in PD patients, but the prevalence of other long-term complications is similar for both groups. Cardiovascular-related problems remain the leading cause of death.
Keywords
Patients and Methods
We included in our study all patients who commenced dialysis before 1990 and whose total dialysis duration in our dialysis program was more than 12 years. We retrieved demographic, clinical, dialysis, and biochemical data for those patients at the 12th year of dialysis and at their most recent follow-up. The censoring date was 30 June 2002.
The dialysis data retrieved included dialysis regime, dialysis adequacy (Kt/V), normalized protein equivalent of nitrogen appearance (nPNA), and (for PD patients) peritoneal transport characteristics. From clinical records, we retrieved information about complications related to long-term dialysis, including cardiovascular disease, bone disease, DRA, and acquired cystic disease (ACD). Clinical outcomes and causes of death were documented. Left ventricular hypertrophy (LVH) was defined by either echocardiographic or electrocardiographic criteria.
Continuous variables are expressed as mean ± standard deviation or median and range. The chi-square test, Fisher exact test, Student t-test, Mann–Whitney test, and univariate analysis using a general linear model were used where appropriate. Cox regression analysis and Kaplan–Meier survival analysis were used to investigate potential predictors of death and of long-term patient survival. Data were analyzed using the SPSS software program, version 10.0 (SPSS Inc., Chicago, IL, U.S.A.), and p values of less than 0.05 were accepted as statistically significant.
Results
Dialysis
At Tung Wah Hospital, 444 patients started dialysis before 1990 (HD = 103, PD = 341). A total of 36 patients (HD = 14, 13.6%; PD = 22, 6.5%) were dialyzed for more than 12 years. Among those 36 patients, 3 (8.3%) had diabetes; 22 (61.1%) were female and 14 (38.9%) were male; and the mean age was 52.51 ± 9.82 years. Table 1 shows the demographic and clinical data.
Baseline Characteristics of Patients at the 12th Year of Dialysis
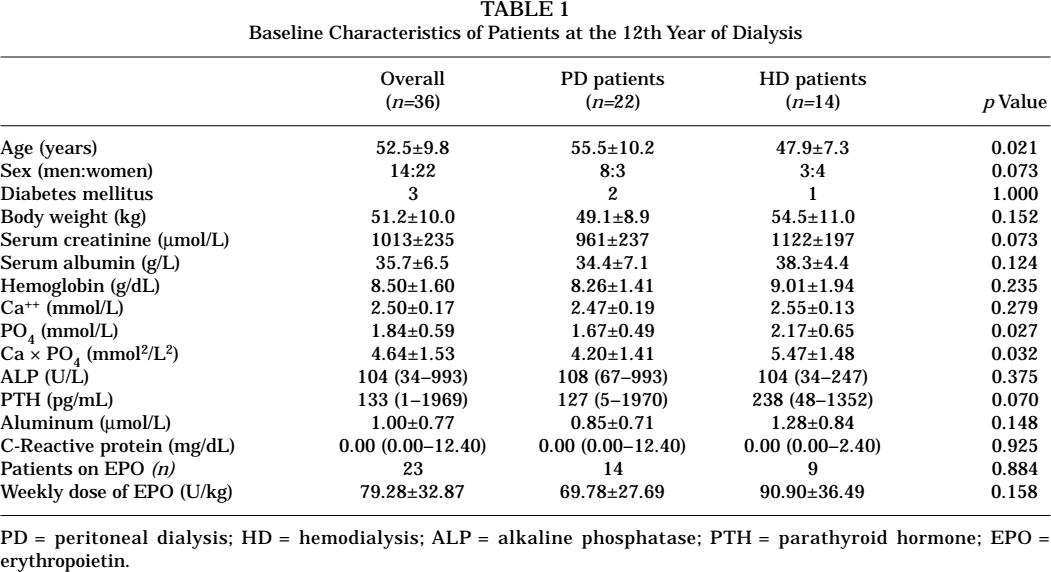
PD = peritoneal dialysis; HD = hemodialysis; ALP = alkaline phosphatase; PTH = parathyroid hormone; EPO = erythropoietin.
The PD patients were older and had lower levels of serum phosphate and calcium × phosphate product as compared with the HD patients. Erythropoietin (EPO) was administered in 23 patients (63.9%) at a mean weekly dose of 79.28 ± 32.87 U/kg, and mean hemoglobin was 8.50 ± 1.60 g/dL. The doses and proportions of patients on EPO were similar in the PD and HD groups.
At the 12th year of dialysis, PD patients were using 6.44 ± 0.86 L of PD fluid daily and had a total weekly Kt/V of 1.89 ± 0.28 and a daily UF of 1021 ± 476 mL. Ten patients were low-average transporters, 7 were high-average transporters, and 4 were high transporters. Transport status was not available for 1 patient. The dialysate-to-plasma ratio (D/P) of creatinine at 4 hours was 0.68 ± 0.10, and the final-to-initial dialysate concentration (D4/D0) of glucose was 0.39 ± 0.07. For HD patients, the total weekly Kt/V was 3.49 ± 0.55. All PD and HD patients were anuric.
Long-Term Complications
At the 12th year of dialysis, 30 patients (83.3%) had cardiovascular disease, the most common types being left ventricular hypertrophy (LVH) in 22 patients (73.3%) and ischemic heart disease (IHD) in 11 patients (36.7%). All patients with IHD presented with angina related to exertion or HD, and 2 patients required coronary artery bypass graft (CABG) at the 11th and 13th year of dialysis. The prevalence of cardiovascular involvement was similar in the PD and HD groups (p = 1.000). Hypertension was found in 29 of the 36 long-term patients (80.6%), with similar prevalence in the PD and HD groups. Table 2 summarizes these data.
Prevalence of Long-Term Complications at the 12th Year of Dialysis
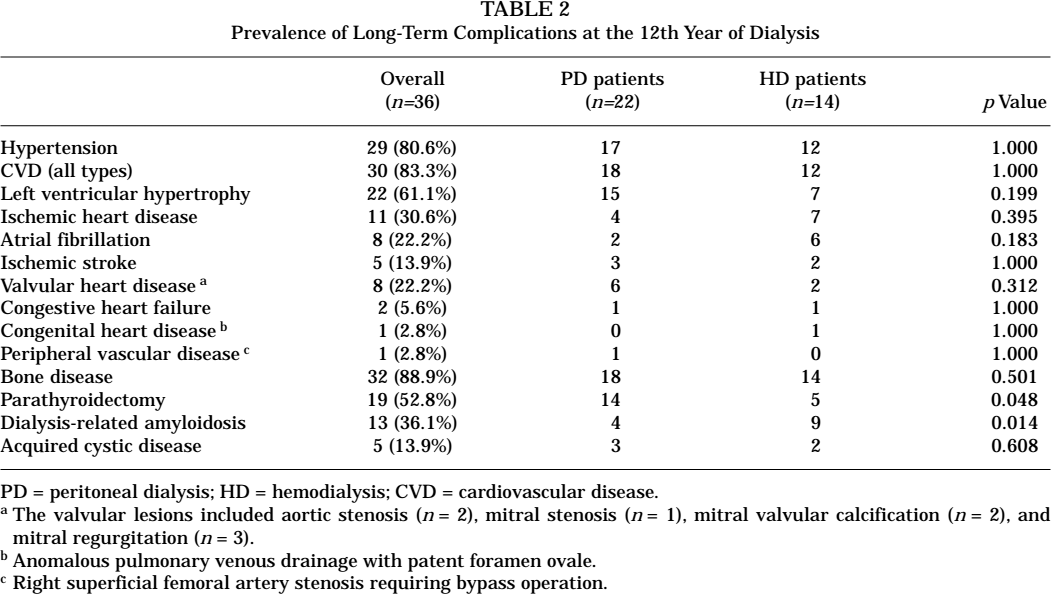
PD = peritoneal dialysis; HD = hemodialysis; CVD = cardiovascular disease.
The valvular lesions included aortic stenosis (n = 2), mitral stenosis (n = 1), mitral valvular calcification (n = 2), and mitral regurgitation (n = 3).
Anomalous pulmonary venous drainage with patent foramen ovale.
Right superficial femoral artery stenosis requiring bypass operation.
Symptomatic DRA was present in 13 patients (36.1%), more commonly in HD patients (p = 0.014, Table 3). The duration of dialysis at presentation with DRA was 142 ± 38 months. Hand numbness from carpal tunnel syndrome (CTS) was the most common presentation (n = 13), followed by joint swelling (n = 2) and tongue enlargement (n = 1). All cases of CTS were confirmed by nerve conduction study. In 10 patients, DRA was diagnosed on clinical grounds; in 1 patient, it was diagnosed by magnetic resonance imaging; and in 2 patients, it was diagnosed by biopsy (tongue biopsy in 1 patient, and biopsy of flexor retinaculum in 1 patient). Intractable CTS led to tendon release operations in 4 patients (30.8%).
Characteristics of Patients at the Most Recent Follow-Up
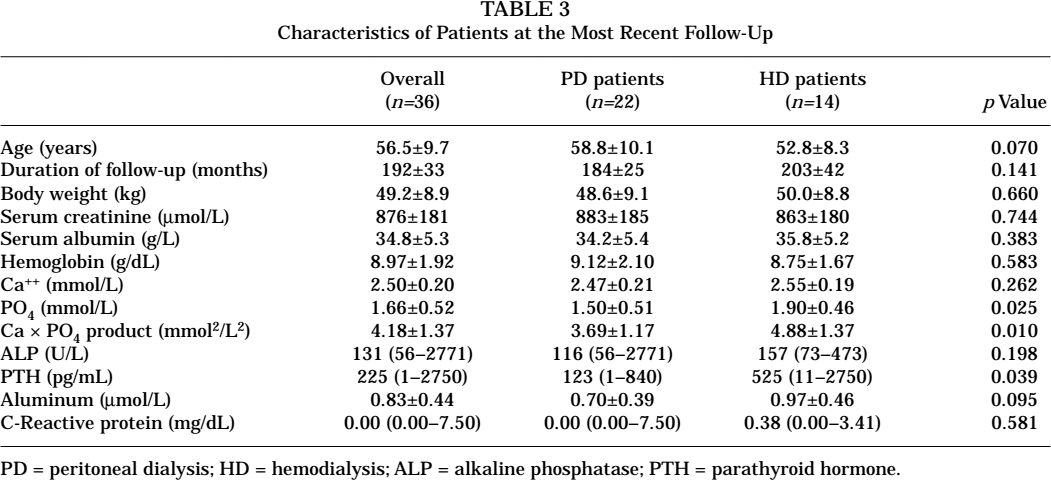
PD = peritoneal dialysis; HD = hemodialysis; ALP = alkaline phosphatase; PTH = parathyroid hormone.
Bone disease was evident in 32 patients (88.9%; PD = 18, HD = 14, p = 0.501) with relevant radiologic features from a skeletal survey. Bone biopsy was performed in 7 of those patients. The radiologic features of bone disease included changes of secondary hyperparathyroidism and osteomalacia—namely, subperiosteal resorption, pepper-pot skull, rugger-jersey spine, brown tumors, looser zones, and pseudofractures. Biopsy findings included osteitis fibrosa (n = 4), osteitis fibrosa with aluminum bone disease (n = 1), osteomalacia (n = 1), and adynamic bone disease (n = 1). Another 4 patients had aluminum bone disease diagnosed by positive desferrioxamine test without bone biopsy. Fracture occurred in 3 patients (fractured hip = 2, fractured rib = 1). Parathyroidectomy was more frequently performed in PD patients (p = 0.048, Table 2). As for bone biochemistry, baseline serum phosphate level and calcium × phosphate product were significantly different between PD and HD patients. Moreover, at the 12th year of dialysis, a trend toward a lower parathyroid hormone (PTH) level was observed in the PD patients (Table 1).
Only 5 patients (13.9%) had documented ACD. Of those, 3 patients (PD = 2, HD = 1) had symptomatic ACD with loin pain and gross hematuria. The ACD was confirmed by ultrasonography, and bleeding was controlled by conservative means. The ACD in the other 2 patients (PD = 1, HD = 1) was detected by ultrasonography done for other reasons. On follow-up, no patients had evidence of malignant change. Kidney ultrasonography was not performed for other patients. Underestimation of the real prevalence of ACD is therefore very likely, and the percentage of ACD in the whole group of patients could not be determined. Table 2 summarizes the prevalence of all long-term complications.
Clinical Outcome
At 30 June 2002, 26 patients were still on dialysis (PD = 13, HD = 13), 3 patients had undergone renal transplantation, and 7 patients had died. The causes of death included sudden death (n = 3), cerebrovascular accident (n = 1), chest infection (n = 2), and peritonitis (n = 1).
The most recent weekly Kt/V values were 2.13 ± 0.72 for PD patients and 3.95 ± 0.79 for HD patients. Most biochemical parameters were similar at the most recent follow-up, but levels of serum phosphate, calcium × phosphate product, and PTH were significantly lower in the PD patients (Table 3).
For survival beyond the 12th year of dialysis, age at commencement of dialysis was the only significant predictor of death (relative risk: 1.281; p = 0.012; 95% confidence interval: 1.057 to 1.553). Mode of dialysis (p = 0.178), sex (p = 0.129), and the presence of diabetes mellitus (p = 0.887) were not predictive of death.
Discussion
Our series showed that only a small proportion of patients were dialyzed for more than 12 years. Compared with our previous series on PD patients with an average dialysis duration of 40.2 months, long-term PD patients in the present series had similar clinical characteristics (Kt/V, dialysis regime, and serum albumin), but most were low-average transporters rather than high-average transporters (1). That finding is not surprising, given that peritoneal transport characteristics significantly affect both patient and technique survival (2).
Complications of long-term dialysis were found to be quite prevalent in both HD and PD patients. With regard to cardiovascular complications, most patients had evidence of IHD and LVH by the 12th year of dialysis. Two patients required CABG for treatment of underlying severe IHD after 11 and 13 years of dialysis. On subsequent follow-up, the most common causes of death were still cardiovascular-related. Apart from conventional cardiovascular risk factors, patients on dialysis were predisposed to cardiovascular disease for a variety of reasons, including chronic low-grade inflammation (3) and high calcium × phosphate product (4).
Deposition of β2-microglobulin in body tissues, leading to DRA, is a well-recognized complication of long-term dialysis. We observed that 40% of patients had symptomatic DRA after a mean duration of approximately 14 years on dialysis; however, the real prevalence of DRA should be much higher, because a large proportion of cases are expected to be subclinical. In the present series, symptomatic DRA was less common in PD patients at the 12th year, suggesting that DRA might present later among PD patients. However, definitive conclusions regarding the effect of dialysis modality on DRA cannot be drawn, because some of the patients changed their mode of dialysis during the follow-up period. It has been suggested that PD may be associated with better clearance of β2-microglobulin, resulting in a lower prevalence of DRA than that seen with HD, but the histologic prevalence of DRA was found by others (5-7) to be similar for patients on different modes of dialysis. Further clarification is needed to delineate the clinical spectrum of DRA for PD and HD patients in the context of long-term dialysis.
Bone disease diagnosed by radiologic means was relatively common in our series as compared with other series (8). However, only a small proportion of patients underwent bone biopsy to confirm the type of renal osteodystrophy. We also noted that HD patients had higher PTH, serum phosphate levels, and calcium × phosphate product both at the 12th year of dialysis and at the most recent follow-up. Those findings may be attributable to a less favorable effect of HD on long-term bone and phosphate metabolism, but they may also be related to a higher incidence of parathyroidectomy in PD patients. The superiority of one dialysis modality over the other with regard to bone and phosphate metabolism is uncertain.
Only a few patients had symptomatic ACD, and none developed renal neoplasm as a complication. Once again, the real prevalence is most likely underestimated, and the prevalence of ACD is expected to be very high in patients on long-term dialysis.
With regard to survival after 12 years, more mortality occurred in PD patients. However when mortality was adjusted for age, the survival rate was not significantly different between the PD and HD groups. A much bigger sample size may be needed to compare the effect of the two modalities on survival after 12 years.
Conclusions
Long-term survival is possible for HD and PD patients alike—particularly young, non diabetic patients. Apart from an age difference, PD patients at their 12th and subsequent years of follow-up had lower levels of serum phosphate, calcium × phosphate product, and PTH. The prevalence of long-term complications such as cardiovascular disease, bone disease, ACD, and DRA were quite similar in PD and HD patients, although PD patients seemed to present later with DRA. Cardiovascular-related problems remained the leading cause of death in the PD and HD groups alike.