
Abstract
Background
Ultrafiltration failure (UFF) is a major complication of peritoneal dialysis (PD). It can occur at any stage of PD, but develops in time and is, therefore, especially important in long-term treatment. To investigate its prevalence and to identify possible causes, we performed a multicenter study in The Netherlands, where patients treated with PD for more than 4 years were studied using a peritoneal function test (standard peritoneal permeability analysis) with 3.86% glucose. UFF was defined as net UF < 400 mL after a 4-hour dwell.
Results
55 patients unselected for the presence or absence of UFF were analyzed. Mean age was 48 years (range 18 – 74 years); duration of PD ranged from 48 to 144 months (median 61 months); UFF was present in 20 patients (36%). Patients with and without UFF did not differ in age or duration of PD. Median values for patients with normal UF compared to patients with UFF were, for net UF 659 mL versus 120 mL (p < 0.01), transcapillary UF rate 3.8 versus 2.1 mL/minute (p < 0.01), effective lymphatic absorption 1.0 versus 1.6 mL/min (p < 0.05), mass transfer area coefficient (MTAC) for creatinine 9.0 versus 12.9 mL/min (p < 0.01), dialysate-to-plasma ratio (D/P) for creatinine 0.71 versus 0.86 (p < 0.01), glucose absorption 60% versus 73% (p < 0.01), maximum dip in D/P sodium (as a measure of free water transport) 0.109 versus 0.032 (p < 0.01), and osmotic conductance to glucose 3.0 versus 2.1 μL/min/mmHg (p < 0.05). As causes for UFF, high MTAC creatinine, defined as > 12.5 mL/min, or a glucose absorption > 72%, both reflecting a large vascular surface, a lymphatic absorption rate (LAR) of > 2.14 mL/min, and a decreased dip in D/P sodium of < 0.046 were identified. Most patients had a combination of causes (12 patients), whereas there was only a decreased dip in D/P sodium in 3 patients, only high MTAC creatinine in 1 patient, and only high LAR in 2 patients. We could not identify a cause in 2 patients. Both groups had similar clearances of serum proteins and peritoneal restriction coefficients. However, dialysate cancer antigen 125 concentrations, reflecting mesothelial cell mass, were lower in the UFF patients (2.79 vs 5.38 U/L).
Conclusion
The prevalence of UFF is high in long-term PD. It is caused mainly by a large vascular surface area and by impaired channel-mediated water transport. In addition, these patients also had signs of a reduced mesothelial cell mass, indicating damage of the peritoneum on both vascular and mesothelial sites.
Keywords
Ultrafiltration failure (UFF) is a serious complication of peritoneal dialysis (PD) that can result in the necessity of prescribing fluid restriction and using higher dialysate glucose concentrations, short-cycle PD, or incidental UF with a hemodialyzer. Sometimes it is the end of PD treatment. Although UFF can occur in any stage of PD, it may develop over time (1,2) and is, therefore, especially important in long-term PD. The exact prevalence of UFF in patients treated with PD for a longer period is not known. Heimbürger et al. have reported a prevalence of 31% for patients treated with PD for more than 6 years (3) and, in a Japanese long-term study, dropout because of UFF was as high as 51% after 6 years (4). Both studies were based on clinical signs of UFF and not on a standardized test.
The definition of UFF has been under discussion over the past years. Some applied a clinical definition: the inability to remain at a certain dry weight and the use of more than two hypertonic bags per day have been considered as UFF (5-7). Others used a definition based on a standardized exchange and considered UFF to be present, for instance, when there was negative net UF with a 1.36% glucose dwell (8,9). The International Society for Peritoneal Dialysis committee on UFF advised performing a standardized test with 3.86% glucose, and considered a net UF of less than 400 mL after a 4-hour dwell as UFF (10). A cross-sectional study in a small number of PD patients, using the 400 mL/4 hours on 3.86% glucose definition, reported a prevalence of 23% (9).
To elucidate the prevalence of UFF in long-term PD patients, based on the current definition of less than 400 mL net UF after a 4-hour test with 3.86% glucose, we performed a study in as many as possible unselected patients on PD in The Netherlands, who had been treated for more than 4 years. The prevalence of UFF in this population was investigated, as were differences in membrane characteristics in patients with and without loss of UF capacity. A possible role of chronic inflammation in the development of UFF was studied by measurement of C-reactive protein (CRP) and albumin. In addition, the causes of UFF were analyzed for each patient.
Methods
With the help of The Netherlands Registry of patients on renal replacement therapy (RENINE), the dialysis centers where patients were treated with PD for more than 4 years could be identified. The nephrologists of these centers were approached to ask the patients to cooperate in this study. When the patients gave informed consent, a standard peritoneal permeability analysis (SPA), with 3.86% glucose in a 4-hour dwell, was performed by a team of three well-trained trial nurses, either in the Academic Medical Center in Amsterdam, or in the centers where the patients were treated.
The analyzed SPAs were performed between October 1996 and December 2000. All patients used commercially available, glucose-based dialysis solutions (Dianeal; Baxter BV, Utrecht, The Netherlands; or StaySafe; Fresenius BV, Nieuwkuijk, The Netherlands), some of them in combination with a glucose polymer (Extraneal; Baxter BV). None of the included patients had peritonitis during the test or during the 4 weeks preceding the test. Patients were considered to have UFF when net UF after 4 hours was less than 400 mL. The protocol was approved by the Committee for Medical Ethics of the Academic Medical Center of the University of Amsterdam.
Procedure
The SPA was performed during a 4-hour dwell period, as described previously (11). The test was done with 3.86% glucose, using the volume the patient was used to. The test dwell was preceded and followed by a rinsing procedure with 3.86% glucose to avoid possible effects of the residual volume before the test, and to calculate the residual volume after the test. Dialysate samples were taken before instillation and at several time points during the test. Blood samples were taken at the beginning and at the end of the test period. A volume marker, dextran 70, 1 g/L (Hyskon; Medisan Pharmaceuticals AB, Uppsala, Sweden), was used to calculate fluid kinetics. To prevent a possible anaphylactic reaction to dextran 70, dextran 1 (Promiten; NPBI, Emmercompascuum, The Netherlands) was injected intravenously before instillation of the test bag (12).
Measurements
Total dextran was determined by means of high performance liquid chromatography (13). Creatinine and urate were measured by enzymatic methods (Boehringer Mannheim, Mannheim, Germany). All electrolytes were determined using ion-selective electrodes. Glucose was measured by the glucose oxidase-peroxidase method, using an AutoAnalyzer (SMA-II; Technicon Instruments, Terrytown, New York, USA). Beta 2-microglobulin was determined with a microparticle enzyme immunoassay (MEIA) with an Imx system (Abbott Diagnostics, North Chicago, Illinois, USA). Albumin, IgG, and alpha 2-macroglobulin were all measured by nephelometry (BN 100; Behring, Marburg, Germany) with commercial antisera (Dakopatts, Glostrupp, Denmark); CRP was measured immunoturbidimetrically.
Dialysate cancer antigen 125 (CA125), used as a marker of mesothelial cell mass, was determined by a commercial MEIA, using a monoclonal antibody against CA125 (Abbott Laboratories), validated for use in dialysate in our laboratory (14).
Calculations
All calculations were performed as previously described by Pannekeet et al. (11).
Fluid Kinetics
Transcapillary ultrafiltration (TCUF) and lymphatic absorption were assessed with the intraperitoneally administered volume marker dextran 70. Transcapillary UF was calculated from the dilution of the volume marker by subtracting the initial intraperitoneal volume (IPV) from the theoretical IPV (when both lymphatic absorption and sampling would not have been present) at any time point. The convective loss of dextran 70 during the dwell was used to calculate the effective lymphatic absorption rate (ELAR). The term “effective” is used because a clearance is employed to estimate a flow, similarly to the effective renal plasma flow as measured by the clearance of para-aminohippuric acid (15).

in which the difference between the instilled (i) and recovered (r) dextran mass is divided by the geometric mean of the dialysate concentration. Using the convective loss of dextran during the dwell from the peritoneal cavity, both by direct uptake into the lymphatics that drain the peritoneal cavity and by transmesothelial transport to calculate the ELAR, implies that all pathways of lymphatic drainage from the peritoneal cavity, including both subdiaphragmatic uptake and interstitial lymphatic drainage, are included in the definition of the ELAR.
Residual volume (RV) was determined by the following equation, in which rs is the rinsing solution, ts is the test solution, V is volume, and C is concentration (16):

Dialysate-to-plasma ratio (D/P) of sodium was calculated as the dialysate sodium concentration divided by the plasma sodium concentration; ΔD/P sodium is the difference between the initial D/P sodium and the lowest D/P sodium (usually after 2 hours). A correction for Na+ diffusion from the circulation to the dialysate, known to cause blunting of the decrease in D/P Na+, was made, as described previously (17), using the mass transfer area coefficient (MTAC) of urate. The calculated sodium concentration in dialysate due to diffusion can then be subtracted from the measured concentration at any time point, resulting in the actual Na+ sieving. Osmotic conductance to glucose was calculated as

where Lp is the liquid permeability of the peritoneum, S is the surface area, and σ is the reflection coefficient (18). The UF coefficient LpS can be calculated using

where TCUFRmax is the maximal transcapillary UF rate as present in the first minute of the dwell. This can be calculated using the Lineweaver-Burke plot, that is, the linear regression between the reciprocal values of the TCUF obtained during the SPA and the reciprocal of time (15). ΔP is the hydrostatic pressure gradient, Δ&PI; is the colloid osmotic pressure gradient, and ΔO is the crystalloid osmotic pressure gradient (18). For ΔP, a value of 9 mmHg was used (19). The colloid osmotic pressure in plasma, &PI;, was calculated in each patient using


In these equations SA represents serum albumin (in grams/liter), 68 000 is the molecular weight of albumin, and the factor 1000 converts osmoles to milliosmoles. The capillary colloid osmotic pressure was determined by the serum plasma albumin for 75%. To this value, 0.4 mOsm was added because of the Gibbs–Donnan equilibrium (20). For Δ&PI;, a σ of 1 is assumed. For glucose, the reflection coefficient σ was calculated for each patient, using the equation

in which αe is the solute radius and r the pore radius. To calculate these parameters, the solute radius of glucose and the small (rS) and large (rL) pore radii of the peritoneal membrane are needed. The solute radius of glucose was previously determined as 3.12 Å (19).
For assessment of the pore radii, we used computer simulations as previously described by Rippe and Stelin (21). In this model, the pore sizes were varied to obtain the best fit between estimated and measured solute clearances (19,22). The average reflection coefficient for both solutes across the peritoneal membrane consists of the sum of the reflection coefficients of each pore set, weighted by their respective fractional UF coefficient (αC for the transcellular pores, αS for the small pores, and αL for the large pores). The values reported by Rippe et al. (21) were used: αC = 0.015, αS = 0.929, and αL = 0.056.
With the calculated reflection coefficients, the actual UF coefficient LpS and the osmotic conductance to glucose were determined for both patient groups.
Solute Transport
Peritoneal handling of low molecular weight solutes was expressed as MTAC and D/P ratios. The MTAC represents the maximal theoretical diffusive clearance of a solute at t = 0, before transport has actually started. In this study, we used the Waniewski model (24). Glucose absorption was calculated as the difference between the amount of glucose instilled and the amount recovered relative to instilled.
Protein clearances were calculated from the amount of protein in the effluent. The intrinsic permeability to macromolecules can be functionally characterized by the peritoneal restriction coefficient (rc). This is the slope of the power relationship between the clearance of serum proteins and their free diffusion coefficient in water (Dw) (25,26):

in which “a” is a constant. All transport parameters were corrected for body surface area and expressed per 1.73 m2.
Analysis of the Causes of UFF
To analyze the causes of UFF in each patient, we used the reference values for peritoneal function tests with 3.86% glucose, obtained in a previous study (27). When a value was outside the 95% confidence interval, it was considered abnormal. The maximum values for the different causes of UFF were as follows: 12.5 mL/min/1.73 m2 for MTAC creatinine, 0.86 for D/P creatinine, 72% for glucose absorption, 2.14 mL/min/1.73 m2 for ELAR, 409 mL for residual volume, and 0.046 for the maximum dip in D/P sodium (after correction for diffusion).
Statistical Analysis
Results are expressed as median values and ranges, because most data were distributed asymmetrically. The Mann–Whitney U-test was employed for the comparison of patients with and patients without UFF.
Results
Patients
RENINE selected 123 patients who had been treated with PD for more than 4 years in the 13 centers cooperating in the study. From this group, 55 patients underwent a SPA. The other 68 patients could not participate because of death (10 patients), transplantation (7 patients), transfer to hemodialysis (8 patients), or patient's refusal to cooperate (24 patients) or their nephrologist's refusal to cooperate (10 patients) for various reasons (e.g., severe comorbidity, psychological factors, participation in other studies). The rest of the eligible patients were not included because of logistical problems. The patients who did not participate were not different from the investigated group with respect to age, sex, and duration of PD.
The investigated patients had a mean age of 48 years (range 18 – 74 years). The duration of PD therapy ranged from 48 to 144 months, median 61 months. The frequency distribution for the duration of PD is shown in Figure 1. Causes of renal failure were chronic glomerulonephritis (18 patients), renal vascular disease (9 patients), polycystic kidney disease (4 patients), diabetic nephropathy (3 patients), congenital kidney disease (2 patients), interstitial nephritis, bilateral nephrectomy (cancer), scleroderma (all in 1 patient each), and unknown in 16 patients.
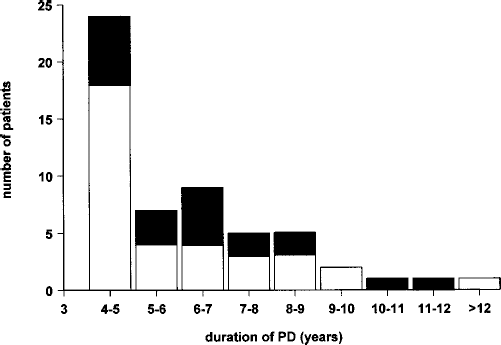
Frequency distribution of the number of patients with (black boxes) and without (open boxes) ultrafiltration failure and the duration of peritoneal dialysis (PD; months).
Transport Characteristics
Among the 55 patients, 20 had net UF < 400 mL after a 4-hour dwell with 3.86% glucose (36%). Patient characteristics for the groups with and without UFF are given in Table 1. Patients with peritoneal membrane failure used significantly more hypertonic or icodextrin exchanges per day than the patients with normal UF. The intraperitoneal fluid profiles for both groups are given in Figure 2.
Clinical Characteristics of the Groups With and Without Ultrafiltration Failure (Medians and ranges are given.)
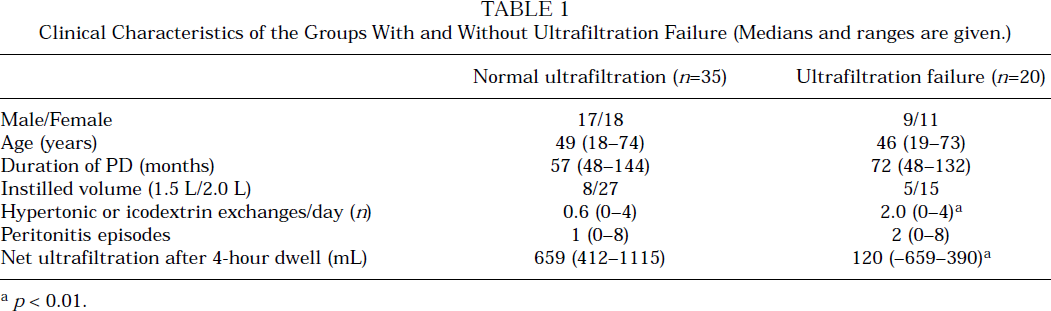
p < 0.01.
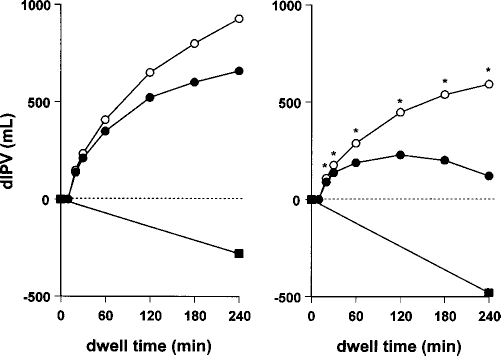
Fluid profiles of the patients with normal ultrafiltration (UF) (left panel) and with UF failure (right panel). Transcapillary UF (open circles), lymphatic absorption (closed squares), and net UF (closed circles) are plotted against time. Asterisks mark values that were significantly different for UF failure patients than for the patients with normal UF. dIPV = change in intraperitoneal volume during the dwell.
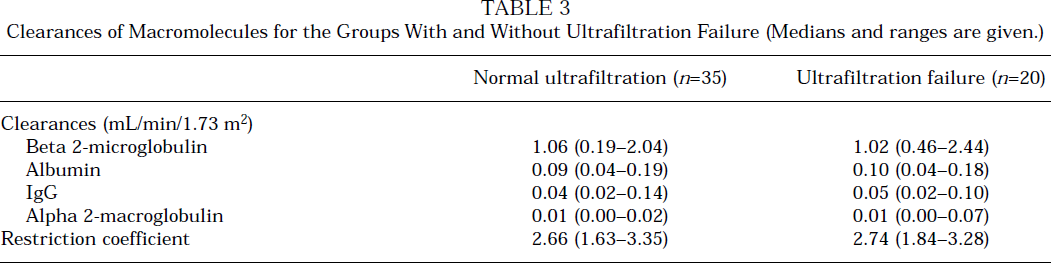
Peritoneal transport parameters are given in Table 2. Patients with UFF had significantly higher MTAC creatinine, D/P creatinine, and glucose absorption than those without UFF. In addition, they had a higher ELAR. The maximum dip in D/P sodium was lower in the patients with UFF than in those without UFF. The UF coefficient LpS was not different for patients with normal UF (0.076 mL/min/mmHg, range 0.02 – 0.33) compared to those with UFF (0.063 mL/min/mmHg, range 0.02 – 0.21), p = 0.26. However, the reflection coefficient for glucose, σ, was significantly lower in patients with UFF than in patients with normal UF (0.025 vs 0.034, p = 0.02). In addition, the osmotic conductance to glucose was lower in the patients with peritoneal membrane failure compared to those with normal net UF (2.1 vs 3.0 μL/min/mmHg, p < 0.05). Neither the residual volume for both groups nor the clearances of macromolecules and the restriction coefficient showed significant differences (see also Table 3).
Peritoneal Transport Characteristics for the Groups With and Without Ultrafiltration Failure (Medians and ranges are given.)
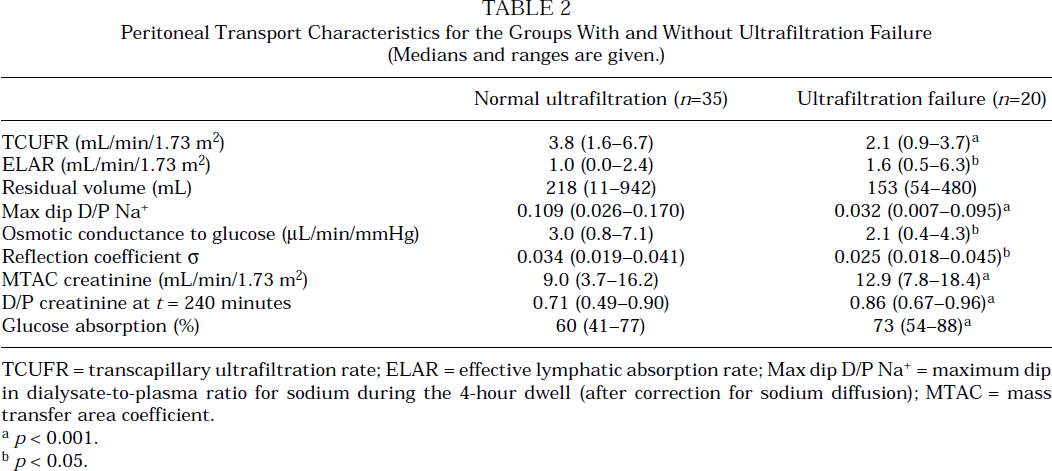
TCUFR = transcapillary ultrafiltration rate; ELAR = effective lymphatic absorption rate; Max dip D/P Na+ = maximum dip in dialysate-to-plasma ratio for sodium during the 4-hour dwell (after correction for sodium diffusion); MTAC = mass transfer area coefficient.
p < 0.001.
p < 0.05.
Clearances of Macromolecules for the Groups With and Without Ultrafiltration Failure (Medians and ranges are given.)
Mean dialysate CA125 concentration in all 55 patients was 4.71 U/L, but it was significantly lower in the patients with UFF compared to those with normal UF (2.79 vs 5.38 U/L, p = 0.02).
For the patients with normal UF, the median serum value for albumin was 34.3 g/L (21.0 – 43.3 g/L) and CRP was 4.5 mg/L (< 3 – 68 mg/L). This was not statistically different from the values for the patients with UFF: 32.8 mg/L (21.0 – 39.9 mg/L, p = 0.1) for albumin and 7.0 mg/L (< 3 – 134 mg/L, p = 0.3) for CRP. No correlations were found between MTAC creatinine and inflammation parameters, or between net UF and albumin or CRP levels
Analysis of the Causes of Uff
The 20 patients with UFF were analyzed individually for the cause of UFF. Six patients had only one cause of UFF: a decreased dip in D/P sodium (3), a high MTAC creatinine (1), or a high ELAR (2). Nine patients had two causes: a combination of high MTAC creatinine with a decreased dip in D/P sodium (7) or with a high ELAR (2). In 2 patients, 3 causes were found (high MTAC creatinine, high ELAR, and a decreased dip); 1 patient also had large residual volume. In 2 patients, no cause of UFF could be identified. No relation was found between the cause of UFF and the duration of PD, as shown in Figure 3.
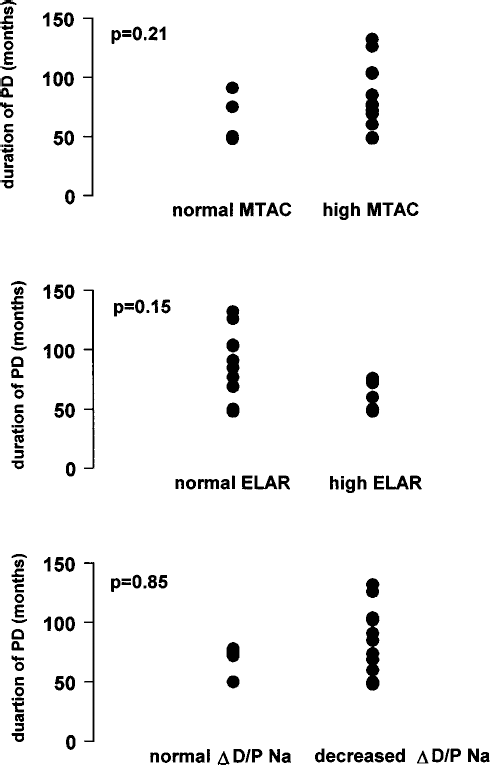
Causes of ultrafiltration failure in 18 patients in relation to duration of peritoneal dialysis (PD). No significant correlation was found. MTAC = mass transfer area coefficient; ELAR = effective lymphatic absorption rate; D/P = dialysate-to-plasma ratio.
Discussion
The present study provides evidence for the clinical observation that UFF is an important complication of long-term PD. Its prevalence was 36% in 55 patients selected only on the basis of duration of PD. This group is probably representative of the whole population of long-term patients, because those who did not participate were not different with respect to age, gender, and duration of PD.
Fluid overload is an important problem in PD patients, especially when residual urine production is absent. It may be caused by high fluid intake, inappropriate PD prescription, noncompliance, or a low drained volume. The latter can be due to mechanical problems, such as catheter dislocation or subcutaneous leakages, or to peritoneal membrane failure. When the diagnosis of UFF is based on a clinical definition, all the above causes of overhydration are included, which might lead to overdiagnosis. Underdiagnosis is also possible when, for instance, a patient with impaired UF due to membrane failure remains in a good hydration status because of strict adherence to severe salt and fluid restriction. When a standardized dialysis dwell is used, as in the present study, a low drained volume can be caused by either mechanical problems or peritoneal membrane failure. Non membrane-related causes, such as catheter dislocation or subcutaneous leaks, were ruled out in this study. In general, membrane-related causes of UFF consist of a large vascular surface area, assessed by MTAC creatinine, a rapid effective lymphatic absorption, and an impaired free water transport. A very rare cause, an extremely small vascular surface area as in, for example, a case of adhesions, where only a limited part of the peritoneum is available as a dialysis membrane (28,29), was not detected in our study population. The presence of a large vascular peritoneal surface area leads to rapid absorption of the dialysis solution and thus to fast disappearance of the osmotic gradient (30). A high peritoneal fluid absorption rate (3,31) leads to a decrease in the drained volume and an impaired conductance to glucose (e.g., peritoneal water channel dysfunction or low peritoneal UF coefficient) (32-34), resulting in UFF. A combination of factors may also be present.
In the present study, the group of patients with UFF used significantly more hypertonic exchanges per day than did the group with normal UF, indicating that clinical signs of fluid overload must have been present. However, in the group of patients with normal UF, some patients were using more than one hypertonic exchange per day, whereas, in the patients with UFF, some did not use any hypertonic exchange. This implies that a clinical definition of UFF can lead to overestimation, as well as underestimation, of the diagnosis UFF.
The UFF patients showed higher transport rates for small solutes (65% of the patients), measured as high MTAC creatinine, high D/P creatinine, and high glucose absorption. This is in accordance with previous publications where small-solute transport parameters were found to be increased in long-term patients, especially when they suffered from UFF (3,35,36). In addition, the UFF patients had higher ELARs (35% of the patients) and a decreased maximum dip in D/P sodium (65% of the patients). Most patients had a combination of etiological factors. The combination of a large vascular surface area with an absence of the dip in D/P sodium was the most frequent one. The osmotic conductance to glucose is the product of the UF coefficient (LpS) and the reflection coefficient σ. In the present study, the patients with UFF had significantly lower osmotic conductance to glucose, owing to a lower reflection coefficient. This lower reflection coefficient indicates impaired channel-mediated water transport. It is speculative whether the absence of dip in D/P sodium in this group is a consequence of the lower net UF, caused by rapid absorption of the osmotic agent due to the large vascular surface area, or an entity by itself. The fact that 3 patients had no other cause of UFF than impaired free water transport implies that water channel dysfunction is an isolated factor in its etiology. In a previous study, three different groups of PD patients with a fast transport status (high MTAC creatinine) were analyzed. It was found that patients with fast transport status in long-term PD had significantly lower maximum dip in D/P sodium than patients with similar MTAC creatinine during continuous ambulatory PD peritonitis and patients with fast transport in the first months of PD (37). These results imply that decreased aquaporin-mediated water transport is especially important in long-term PD. Suggestions about challenging the water channel transport with an even more hypertonic dialysis solution have been made (38), but it is questionable how hypertonic this solution should be and whether it would be ethical to use such solutions for investigational purposes.
The relation between the occurrence of UFF in long-term PD and peritonitis incidence was investigated previously. The results were equivocal. Most publications showed no direct relation (3,5,39), although some authors have found a relation with late peritonitis episodes, recurrent infections, or peritonitis clusters (2). In the present study, the incidence of peritonitis in the patient groups with and without UFF was similar. This suggests that, in long-term PD, peritonitis does not play a major role in the development of UFF. An alternative explanation could be that the patients with frequent peritonitis episodes had been transferred to other renal replacement therapies because of UFF before they reached the inclusion criterion of 4 years of PD treatment.
Over past years, much attention has been given to chronic inflammation as a predictor of outcome in dialysis. An elevated CRP level at the start of dialysis was found to correlate to higher mortality (40,41). The results of previous investigations on possible relationships between peritoneal transport status and serum parameters of inflammation were equivocal. Chung et al. reported inflammation to be correlated with fast transport status in the first year of PD (42). However, Wang and co-workers did not find a correlation between transport rates and states of chronic inflammation (43). In the present study, the inflammation parameters serum albumin and CRP were investigated. No difference was found between the groups with and without UFF, nor was there a correlation between transport status and the different inflammation markers. A possible explanation for this may be that effects of chronic inflammation on peritoneal transport are overshadowed by the anatomical changes after years of PD. An alternative explanation could be that the patients with the highest inflammation parameters had already dropped out of PD treatment because of morbidity and mortality.
Cancer antigen 125 can be used as a marker of mesothelial cell mass and cell turnover in stable, noninfectious PD patients. A negative trend with duration of PD, described previously (44), is consistent with the reported cell loss observed in peritoneal biopsies (45). Although mesothelial cells are not considered involved in peritoneal transport, loss of the protection of the mesothelial cell layer can probably influence the damage to the endothelial cell layer. The finding in the present study that long-term patients with UFF had lower CA125 levels than those with normal UF is therefore more likely a sign of damage to the peritoneum than a causative factor of UF by itself.
It can be concluded that the prevalence of UFF is high in long-term PD patients. It is caused mainly by a combination of a large vascular surface area and by impaired free water transport. In addition, long-term patients with UFF had signs of reduced mesothelial cell mass, indicating damage to the peritoneum, at both vascular and mesothelial sites.