
Abstract
Peritonitis is a well-known cause of mortality in peritoneal dialysis (PD) patients. We carried out a retrospective study to disclose the clinical spectrum and risk profile of peritonitis-related mortality. We analyzed 693 episodes of infectious peritonitis suffered by 565 patients (follow-up 1149 patient-years). Death was the final outcome in 41 cases (5.9% of episodes), peritonitis being directly implicated in 15.2% of the global mortality and 68.5% of the infectious mortality observed. In 41.5% of patients with peritonitis-related mortality, the immediate cause of death was a cardiovascular event. Highest mortality rates corresponded to fungal (27.5%), enteric (19.3%), and Staphylococcus aureus (15.2%) peritonitis. Multivariate analysis disclosed that the baseline risk of peritonitis-related mortality was significantly higher in female [relative risk (RR) 2.13, 95% confidence interval (CI) 1.24 – 4.09, p = 0.02], older (RR 1.10/year, CI 1.06 – 1.14, p < 0.0005), and malnourished patients (RR 2.51, CI 1.21 – 5.23, p = 0.01) with high serum C-reactive protein (s-CRP) levels (RR 4.04, CI 1.45 – 11.32, p = 0.008) and a low glomerular filtration rate (RR 0.75 per mL/minute, CI 0.64 – 0.87, p < 0.0005). Analysis of risk after a single episode of peritonitis and/or subanalysis restricted to peritonitis caused by more aggressive micro-organisms disclosed that overall comorbidity [odds ratio (OR) 1.21, CI 1.05 – 1.71, p = 0.005], depression (OR 2.35, CI 1.14 – 4.84, p = 0.02), and time on PD at the time of the event (OR 1.02/month, CI 1.00 – 1.03, p = 0.02) were other predictors of mortality.
In summary, the etiologic agent is a definite marker of peritonitis-related mortality but gender, age, residual renal function, inflammation (s-CRP), malnutrition, and depression are other significant correlates of this outcome. Most of these risk factors are common to cardiovascular and peritonitis-related mortality, which may explain the high incidence of cardiovascular event as the immediate cause of death in patients with peritonitis-related mortality.
Many studies have explored the prognostic spectrum of PD-related peritonitis (4-15), in most cases emphasizing the relevance of factors such as the etiologic agent(s), the severity of the initial clinical presentation, or the efficacy of different therapeutic approaches. Hospitalization, peritoneal catheter loss, and technique failure, with dropout to hemodialysis (HD), are the most frequently quoted serious consequences of these infections, while direct peritonitis-related mortality has generally been considered as a most severe but secondary outcome, due to the relatively low incidence of this event. On the other hand, few studies have analyzed the specific clinical spectrum of peritonitis-related mortality (3,16) and the association of this outcome with baseline or single-episode-related risk factors other than the etiologic agent or the immediate clinical aggressiveness of the infection. It is conceivable that the many debilitating conditions that frequently concur in dialysis patients may contribute to defining the outcome of PD-related peritonitis, but this possibility has been insufficiently studied.
We performed a retrospective study to assess the clinical spectrum and risk profile of peritonitis-related mortality in a wide population of patients undergoing PD in a single center for a period exceeding 18 years.
Population and Method
We analyzed retrospectively the information recorded in an extensive prospective database of patients undergoing PD in our unit between 1 January 1986 and 31 March 2004, with the aims of establishing the incidence, clinical spectrum, and risk profile for peritonitis-related mortality during the aforementioned period.
Study Population
During the study period, 565 patients underwent PD therapy in our unit. Their main baseline characteristics are displayed in Table 1. Total follow-up was 1149 patient-years (range 1 – 125 months).
Baseline Characteristics of the Study Population. Values expressed as [n (%)] unless otherwise.
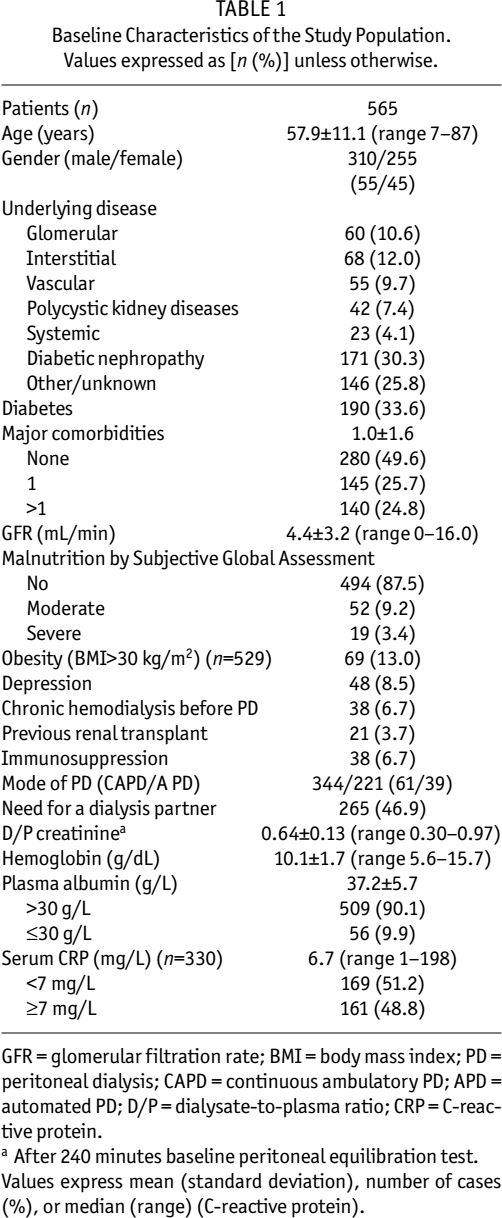
GFR = glomerular filtration rate; BMI = body mass index; PD = peritoneal dialysis; CAPD = continuous ambulatory PD; APD = automated PD; D/P = dialysate-to-plasma ratio; CRP = C-reactive protein.
After 240 minutes baseline peritoneal equilibration test. Values express mean (standard deviation), number of cases (%), or median (range) (C-reactive protein).
All patients used standard continuous ambulatory PD (CAPD) or automated PD systems. Y-set systems were progressively introduced starting in 1987, and only 36 patients (6.4%) used traditional spike systems for CAPD exchanges at any time during follow-up.
Definition of Variables
We defined “peritonitis-related mortality” as the death of a patient due to any immediate cause but under one of three circumstances:
During the course of a clinically active peritonitis (persistent abdominal pain and/or turbid dialysate);
During the week following complete clinical, bacteriologic, and cytological remission of an episode of peritonitis;
In the case of a refractory peritonitis demanding catheter removal, before hospital discharge for reinitiation of regular dialysis therapy (PD or HD).
Peritoneal dialysis-related peritonitis was diagnosed according to standard criteria. The term “complicated peritonitis” was used generically to include any episode of infectious peritonitis deserving an approach beyond simple antibiotic therapy. We diagnosed “refractory peritonitis” in the presence of persistent clinical activity and/or bacteriologic positivity after 5 days of appropriate antibiotic therapy. The definition of “enteric peritonitis” was based on bacteriologic criteria: growth in dialysate of one or more anaerobic intestinal bacteria and/or at least two micro-organisms characteristic of intestinal flora (including Enterobacteriaceae, Enterococcus spp, and yeasts, among others).
The determinant role of the etiologic agent on peritonitis-related mortality may compound any strategy of analysis of risk factors for this complication of PD. Trying to overcome this methodological limitation, we performed a specific subanalysis restricted to episodes of peritonitis caused by more aggressive micro-organisms, which were grouped under the term “severe peritonitis.” We included in this subset fungal (primary or secondary) and enteric peritonitis, as well as infections caused by mycobacteria, Staphylococcus aureus, and Pseudomonas aeruginosa and related bacteria.
Treatment of Peritonitis
Our protocol of empiric antibiotic therapy for PD-related peritonitis has been based on intraperitoneal ciprofloxacin during the past 16 years, and has been described in detail elsewhere (17). During follow-up, antibiotic therapy may be modified according to bacterial antibiotic sensitivity and clinical course. Management of complicated peritonitis includes catheter removal in case of fungal (immediate) or refractory peritonitis. Indication for exploratory laparotomy during enteric peritonitis is individualized, based on clinical presentation and/or diagnostic workup (including routine abdominal computed tomographic scan). These criteria remained stable during the study follow-up.
Strategy of Analysis
The analysis was carried out over two secondary data files based on patients and individual episodes of peritonitis respectively. The first was used to establish the baseline risk profiles for presenting at least one episode of infectious peritonitis (any type) or severe peritonitis, and for peritonitis-related mortality. The second file allowed mathematic modeling of the risk of death associated with a single episode of peritonitis (any) or severe peritonitis.
The baseline variables considered for analysis included age, gender, underlying renal disease, diabetes mellitus, mode of PD (assignment according to intention-to-treat criteria in case of change), partial or complete incapacity for self-dialysis (requiring a dialysis partner), peritoneal transport characteristics at the start of PD [as estimated from dialysate-to-plasma ratio (D/P) of creatinine after 240 minutes in a standard peritoneal equilibration test (PET)], glomerular filtration rate (GFR; estimated from mean renal clearance), major comorbidities, malnutrition [standard Subjective Global Assessment (SGA)], obesity (body mass index > 30 kg/m2), depression (ongoing antidepressant therapy at the start of PD therapy), procedure other than conservative therapy (HD, previous renal transplant), previous or current immunosuppressive drug therapy, and hemoglobin, plasma albumin (by automatic analyzer), and serum C-reactive protein (s-CRP) levels (by immunoturbidimetry; Roche Diagnostics, Mannheim, Germany). The comorbidity score was applied as the sum of all the major comorbidities (both cardiovascular and non-cardiovascular) present at the time of initiation of PD therapy, without correction for severity. Depression and malnutrition received specific attention and were not computed in the general comorbidity score. Given the low prevalence of severe malnutrition, moderate and severe malnutrition were grouped as one binary variable (present/absent).
For the analysis of risk after a single episode of peritonitis, some baseline variables, including age, accumulated comorbidity, mode of PD, malnutrition, obesity, antidepressant and immunosuppressive therapy, and hemoglobin and albumin values, were updated to the last control available before the event. Other variables considered for this part of the analysis included time on PD at the time of the event, etiologic agent, baseline peritoneal cell count, and some basic clinical markers of aggressiveness (hospital admission, peritoneal catheter removed, laparotomy performed, relapse, superinfection, and simultaneous exit-site infection).
All variables were available for study in at least 95% of the cases, with the exceptions of D/P creatinine (n = 323), GFR (n = 508), body mass index (n = 529), and s-CRP (n = 330).
Statistics
Univariate statistical analysis was based on Student's t-test (unpaired data), chi-square distribution, analysis of variance, and Mann–Whitney's test. The multivariate approach included Cox's proportional hazard model (patient-based risk profiles) and logistic regression analysis (peritonitis-based risk profiles). In the former case, patients were censored in case of renal transplant, loss to follow-up, or death due to causes other than peritonitis (peritonitis-related mortality). The strategy of multivariate analysis included creating a best-fit model for the explored event and then introducing other variables, alone or in combination, to obtain adjusted estimations of the independent relative risk (RR; Cox's model) or odds ratio (OR; logistic regression) associated with these secondary variables. Statistical analysis was produced with the help of the SPSS 12.0 software (SPSS Inc., Chicago, Illinois, USA).
Results
General Overview
We recorded 733 episodes of peritonitis during follow-up, but 40 cases were excluded from analysis due to noninfectious etiology (eosinophilic, chemical, icodextrin). The incidence of peritonitis declined progressively during the study follow-up (Figure 1), but the absolute number of infections increased during the same period due to the growing number of patients undergoing PD in our unit (20 patients treated in 1986, compared with 123 in 2003). The etiologic spectrum of infectious peritonitis and the corresponding accumulated mortality rates are presented in Table 2. The distribution of peritonitis by etiologic agent was relatively homogeneous in time, with the exceptions of Staphylococcus aureus infections (21 of 46 episodes before the end of 1990, when mupirocin was introduced for treatment of carriers) and enteric peritonitis, which, for unclear reasons, had a peak incidence during the period 1998–2000. Figure 2 depicts the time courses of global and peritonitis-related mortalities. Our criteria for the diagnosis of severe peritonitis was met in 159 episodes of peritonitis (including 18 superinfections by yeasts) suffered by 127 patients.
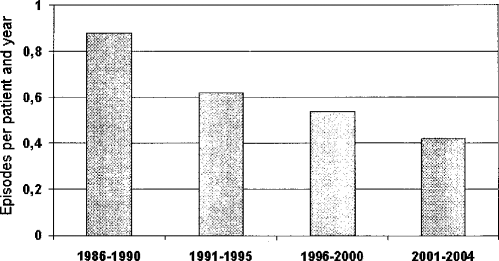
Time course of the incidence of peritonitis during the study period.

Accumulated global and peritonitis-related mortality rates in different phases of follow-up.
Etiologic Agents of Peritonitis. Values expressed as [n (%)].
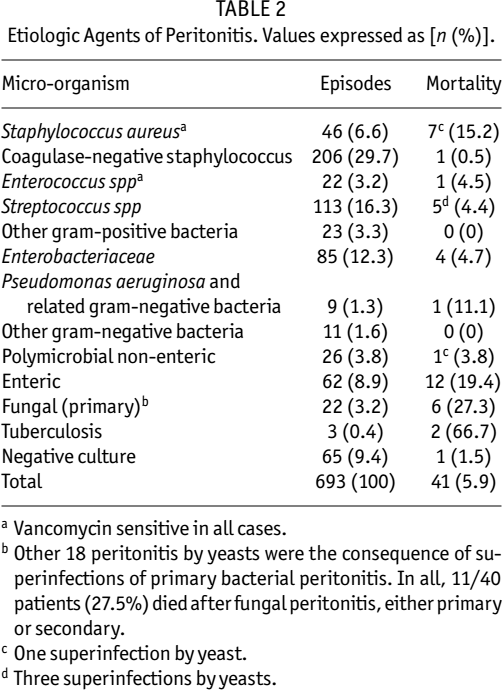
Vancomycin sensitive in all cases.
Other 18 peritonitis by yeasts were the consequence of superinfections of primary bacterial peritonitis. In all, 11/40 patients (27.5%) died after fungal peritonitis, either primary or secondary.
One superinfection by yeast.
Three superinfections by yeasts.
Risk of Presenting Peritonitis
Only 267 patients (47.3%) remained free of peritonitis by the end of their follow-up. Univariate analysis of the baseline risk profile for presenting at least one episode of peritonitis disclosed that this event was more likely in older patients (mean age 60.1 years if peritonitis, compared with 55.3 if no peritonitis, p < 0.001) undergoing CAPD (56.4% presented peritonitis, compared with 46.4% of patients undergoing automated PD, p = 0.012), needing a dialysis partner (58.0% with peritonitis, compared with 47.5% of patients able to perform self-dialysis, p = 0.012), previously treated with HD (71.1% had peritonitis, compared with 51.1% of patients with PD as first renal replacement therapy, p = 0.014), with a poorer GFR (mean 3.9 vs 4.9 mL/minute, p = 0.001), lower hemoglobin levels (mean 9.9 vs 10.2 g/dL, p = 0.03), higher s-CRP levels (median 10.3 vs 5.2 mg/L, p = 0.001 Mann–Whitney), and a longer follow-up on PD therapy (mean 32.2 vs 16.0 months, p < 0.001); other variables were not significant (NS).
The baseline risk of suffering at least one instance of severe peritonitis appeared to be higher in women (26.0% suffered severe peritonitis, compared with 14.6% of males, p = 0.001), older patients (mean age 60.3 vs 57.2 years, p = 0.07), needing a dialysis partner (25.2% had severe peritonitis, compared with 14.9% of patients able to perform self-dialysis, p = 0.003), previously treated with HD (42.1% compared with 18.5% of patients coming from conservative therapy, p = 0.001), with more comorbidities (mean 1.2 vs 0.9 per patient, p = 0.013), poorer GFR (mean 3.2 vs 4.7 mL/min, p = 0.001), a depressive background (31.3% compared with 18.6% of non-depressed patients, p = 0.016), lower hemoglobin levels (mean 9.6 vs 10.2 g/dL, p = 0.02), higher baseline s-CRP levels (median 12.2 vs 6.5 mg/L, p = 0.06 Mann–Whitney), and a longer follow-up on PD therapy (mean 32.9 vs 22.0 months, p < 0.001); other variables were NS.
The results of multivariate analysis of the risk profiles for presenting at least one episode of peritonitis or severe peritonitis are presented in Table 3. A baseline s-CRP level ≥7 mg/L carried a relative risk of 1.62 (95% confidence interval 1.10 – 2.38, p = 0.015) of presenting at least one episode of peritonitis during follow-up.
Spectrum of Peritonitis-Related Mortality
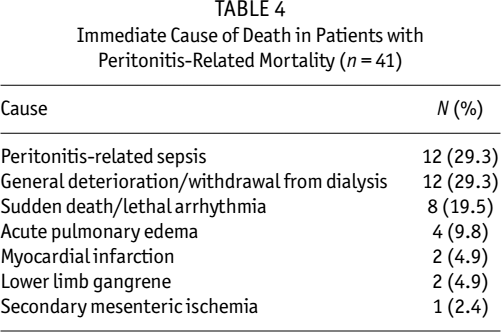
In all, 41 patients died as a consequence of peritonitis. In 24 cases (58.5%), peritonitis was considered the main cause of death; in 13 other cases (31.7%), the infection had a clearly significant role as a cause of death but other previous conditions, including dementia/failure to thrive (n = 9), cardiovascular disorders (n = 4), and neoplastic/ischemic abdominal disease (n = 4), contributed significantly to the final outcome. Finally, in 4 other cases (9.8%), the role of peritonitis was uncertain but probably not determinant as a cause of death. Table 4 displays the immediate circumstances of death in the 41 patients who suffered peritonitis-related mortality. Remarkably, the immediate cause of demise was a cardiovascular event in 41.5% of the cases. Six patients died suddenly during the course of a HD session during the days following removal of the peritoneal catheter.
Baseline Risk Profile for Presenting at Least One Episode of Infectious Peritonitis (All) or Severe Peritonitis. Multivariate Analysis.
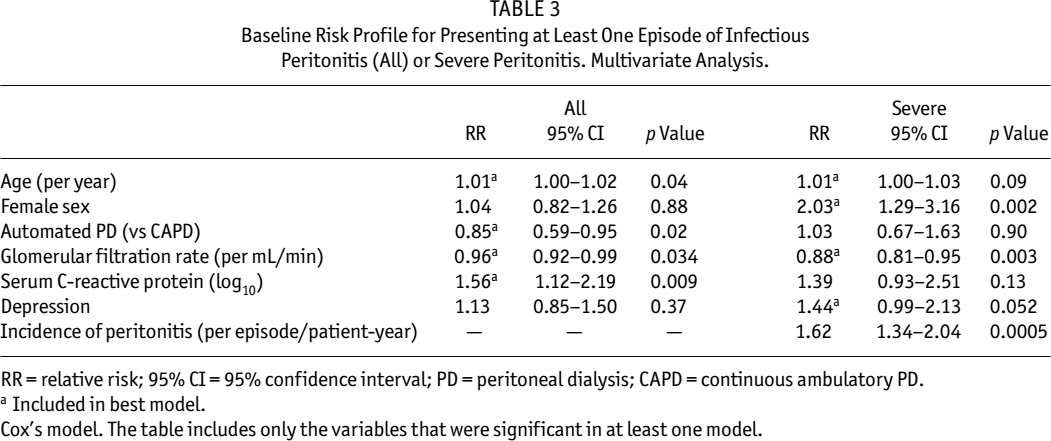
RR = relative risk; 95% CI = 95% confidence interval; PD = peritoneal dialysis; CAPD = continuous ambulatory PD.
Included in best model.
Cox's model. The table includes only the variables that were significant in at least one model.
Immediate Cause of Death in Patients with Peritonitis-Related Mortality (n = 41)
Baseline Risk Profile of Peritonitis-Related Mortality
Table 5 depicts the main baseline characteristics of patients with peritonitis-related mortality, compared with survivors and patients dying for reasons other than peritonitis. The results of multivariate analysis of the baseline risk profile for peritonitis-related mortality are presented in Table 6. A baseline s-CRP level ≥7 mg/L portended a RR of 4.04 (95% confidence interval 1.45 – 11.32, p = 0.008) of peritonitis-related mortality.
Baseline Risk of Peritonitis-Related Mortality: Comparison with Patients Dying from Other Causes and Survivors. Univariate Analysis.
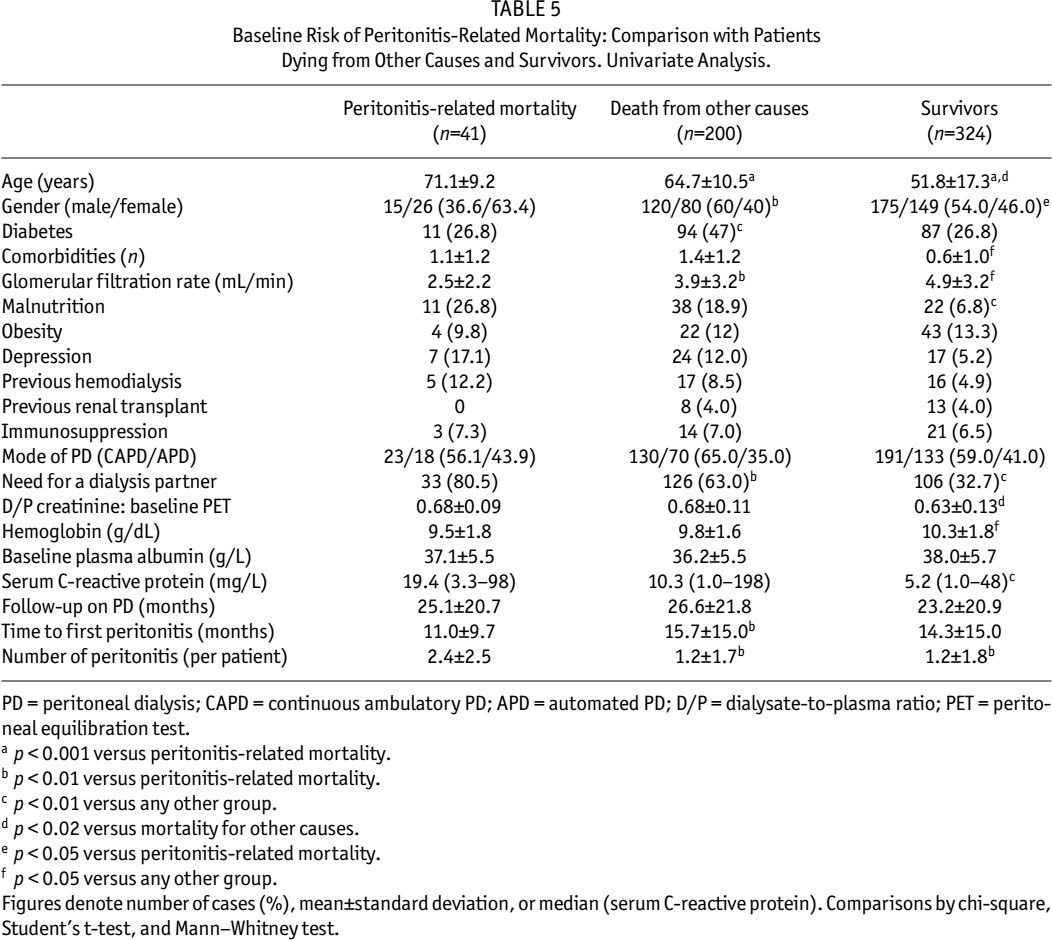
PD = peritoneal dialysis; CAPD = continuous ambulatory PD; APD = automated PD; D/P = dialysate-to-plasma ratio; PET = peritoneal equilibration test.
p < 0.001 versus peritonitis-related mortality.
p < 0.01 versus peritonitis-related mortality.
p < 0.01 versus any other group.
p < 0.02 versus mortality for other causes.
p < 0.05 versus peritonitis-related mortality.
p < 0.05 versus any other group.
Figures denote number of cases (%), mean±standard deviation, or median (serum C-reactive protein). Comparisons by chi-square, Student's t-test, and Mann–Whitney test.
Baseline Risk Profile for Peritonitis-Related and All-Cause Mortalities. Multivariate Analysis. Cox's Model.
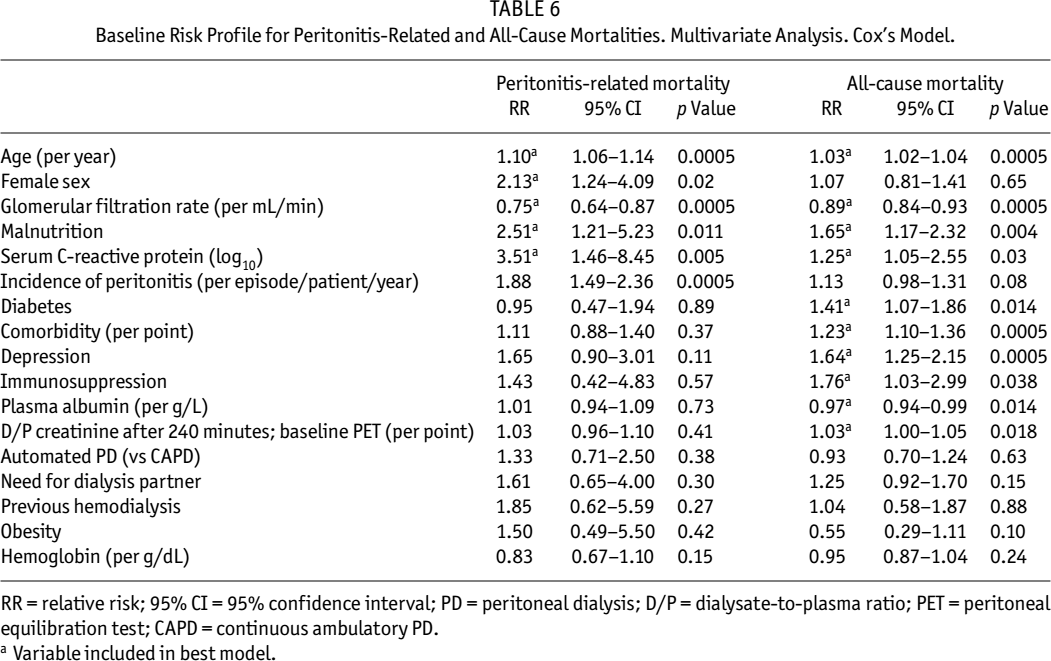
RR = relative risk; 95% CI = 95% confidence interval; PD = peritoneal dialysis; D/P = dialysate-to-plasma ratio; PET = peritoneal equilibration test; CAPD = continuous ambulatory PD.
Variable included in best model.
Risk Profile of Mortality after a Single Episode of Peritonitis
Univariate analysis of the risk profile for mortality after a single episode of infectious peritonitis indicated that this outcome was associated with older age (mean 73.3 years for lethal vs 61.7 for nonlethal infection, p < 0.001), female sex (63.4% of lethal infections vs 45.8% of nonlethal infections, p = 0.02), and overall comorbidity (mean 1.6 points if lethal infection, compared with 0.9 if nonlethal infection, p = 0.02) and malnutrition at the time of the episode (31.7% of lethal infections vs 12.2% of nonlethal infections, p = 0.001). As expected, lethal peritonitis was accompanied by features of clinical aggressiveness (hospital admission, peritoneal catheter removal, laparotomy performed; all p < 0.01 vs nonlethal peritonitis). Finally, there was a minor trend to higher peritoneal leukocyte counts in lethal peritonitis (median 1865 cells/mm3, compared with 1280 in nonlethal peritonitis; p = 0.10, Mann–Whitney). Table 7 presents the results of multivariate analysis of risk factors of mortality after a single episode of peritonitis (all) or severe peritonitis.
Mortality After a Single Episode of Peritonitis (All) or Severe Peritonitis. Multivariate Analysis. Logistic Regression Analysis.
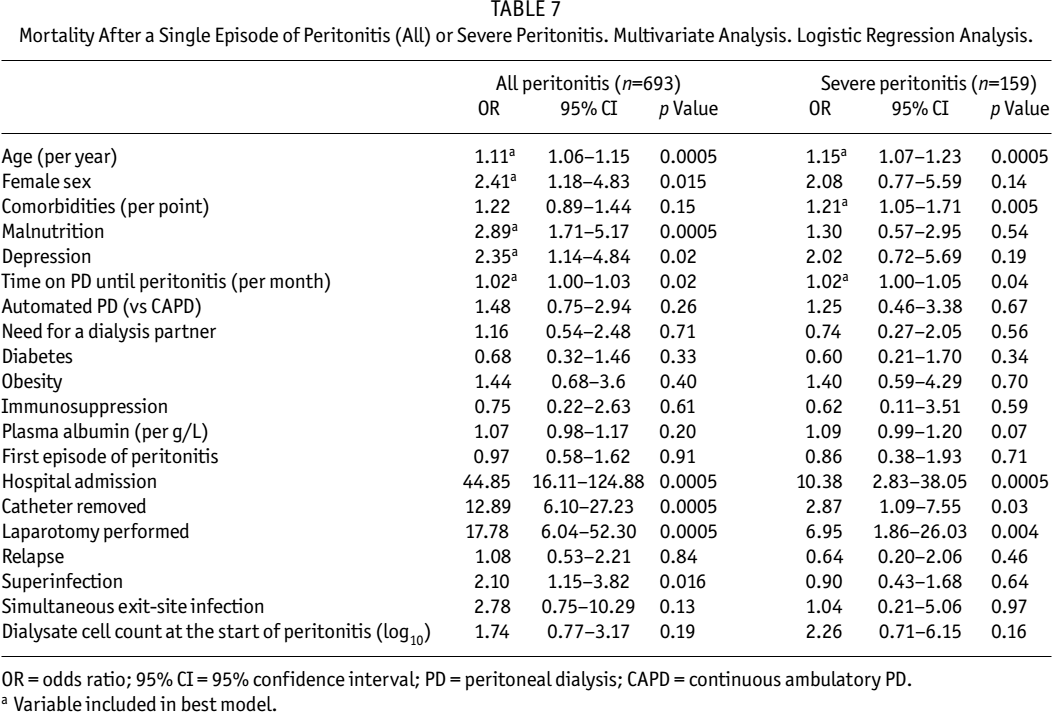
OR = odds ratio; 95% CI = 95% confidence interval; PD = peritoneal dialysis; CAPD = continuous ambulatory PD.
Variable included in best model.
Discussion
Our results show that peritonitis represents a significant cause of mortality in patients undergoing PD therapy. The accumulated peritonitis-related mortality rates observed in our center (15.2% of deaths and 68.5% of infectious deaths) match well with values reported previously (3). On the other hand, peritonitis-related mortality rates did not change markedly during a long study follow-up (Figure 2) and did not improve significantly on results reported in older studies (3,16). There are two possible explanations for this seemingly unexpected finding. First, technical advances in PD therapy have been relatively successful at preventing some of the less aggressive forms of peritonitis (including coagulase-negative staphylococci infections) but, with the possible exception of S. aureus (1), their impact on the incidence of the most severe forms of peritonitis (namely fungal and enteric infections) has been small, if any (2). Second, the clinical condition (age, diabetes, comorbidity) of patients starting PD therapy has declined markedly in past years (18). The combination of relatively higher incidences of more aggressive forms of peritonitis affecting progressively more debilitated patients may underlie the lack of improvement in peritonitis-related mortality rates, as observed in our study.
Our study confirms also the definite role of the etiologic agent in the outcome of PD-related peritonitis. Infections by S. aureus (10,11), Pseudomonas aeruginosa (3,9,14), fungi (3,7,8), mycobacteria (19), and enteric micro-organisms (5,6,20,21), which together formed the severe peritonitis group, are well known for their significant morbidity and mortality rates. On the contrary, single gram-negative bacteria and vancomycin-sensitive Enterococcus spp may be less consistently associated with a complicated course and mortality after peritonitis, as shown by our own results (Table 2); consequently, we excluded these two groups from the subset of severe peritonitis.
It is noteworthy that, in 41.5% of patients with peritonitis-related mortality, the immediate cause of death was a cardiovascular event, representing indirect evidence of the impact of preexisting cardiovascular disease on the outcome of PD-related peritonitis. This association has been suggested by some previous studies (3,16,20) and our results provide further evidence of the high incidence of cardiovascular mortality during the period surrounding an episode of severe peritonitis. Our analysis of the risk profile for peritonitis-related mortality provides new clues to understanding this correlation.
In past years, several studies have clearly demonstrated that residual renal function is a strong correlate of overall survival of PD patients (22-25). Our study is the first to demonstrate that baseline GFR has a specific and consistent inverse correlation with the later incidence of peritonitis (Table 3) and peritonitis-related mortality (Table 6). It is evident that a lower number of bag exchanges in patients with a significant GFR may reduce the chances for contamination and subsequent infection, but this explanation seems clearly insufficient to justify such a strong correlation. On the other hand, low or absent GFR at the start of dialysis is a hallmark of delayed referral (a variable not explored in this study) (26) and secondary selection of PD (after chronic HD), and is associated with inadequacy of dialysis, malnutrition (22), inflammation (27), and volume overload (28), among other complications. It is true that the correlation between GFR and peritonitis outcomes persisted after controlling for the effects of malnutrition (SGA) and s-CRP levels (Tables 3 and 6), but residual renal function may still have predicted the risk of peritonitis by performing as a marker of poor medical and nonmedical conditions of PD patients.
Baseline s-CRP levels were strongly predictive of the later risk of presenting both peritonitis and severe peritonitis (Table 3), as well as of peritonitis-related mortality (Table 6). Previous attempts to establish this correlation have been unsuccessful (29), but peritonitis is generally recognized as a potential source of inflammation in patients undergoing PD therapy (30). Several studies (29,31-34) have explored the correlation between s-CRP and general mortality in PD patients, confirming the well-known association between this marker of inflammation and cardiovascular risk in chronic renal failure (35). Our study provides the first evidence of an association between a baseline inflammatory state and the later incidence of peritonitis and peritonitis-related mortality.
The background of the correlation between a baseline inflammatory state and the following risk of peritonitis and peritonitis-related mortality in PD patients is not clear. We cannot even discard a chance association, as some subsets of patients could present, for independent reasons, increased s-CRP levels and high incidences of peritonitis. Alternatively, inflammatory states are strongly associated with cardiovascular disease, malnutrition, and, in general, clinical deterioration of affected patients (30). Thus, similar to the case of GFR, inflammation may define a subgroup of debilitated patients prone to more frequent infections and complicated clinical courses. A third, more speculative hypothesis may be based on the potential links between inflammatory states and intestinal permeability. First, it is conceivable that a functionally (e.g., due to wall edema in volume overloaded patients) or anatomically (e.g., colonic diverticulosis) disrupted intestinal wall, with recurrent microbial transmigration, may be a source of inflammation in some patients. On the other side, we know, mainly from studies in critical patients (36), that proinflammatory cytokines may induce dysfunction of the gut mucosal barrier. In either of those cases, high s-CRP levels could be, in some patients, a marker for a disabled antimicrobial intestinal barrier, with a potentially increased risk of peritonitis by intestinal micro-organisms during PD therapy. Our results are consistent but do not provide evidence favoring this hypothesis.
Advancing age was strongly associated with the risk of presenting PD-related peritonitis (Table 3). Previous information on the relative incidence of these infections in elderly patients is controversial [reviewed in Ref. (37)] but our results demonstrate that older PD patients experience a definite risk of severe peritonitis (Table 3) and peritonitis-related mortality (Tables 5, 6, 7). On the other hand, our study showed that female patients were more likely to present severe peritonitis but not all-cause peritonitis (Table 3) than were males. As an expected consequence, the risk of peritonitis-related mortality was also higher in women (Tables 6 and 7). The explanation for this previously unreported finding is not clear but the female genitourinary tract may act as a potential reservoir for yeasts and other micro-organisms causing aggressive peritonitis during PD therapy.
Depressive disorders are relatively frequent in patients on dialysis and have been demonstrated to be associated with malnutrition (38), hospitalization (39), general mortality (39,40), and, in the case of PD patients, a high incidence of peritonitis (41). Our study confirmed a consistent association between depressive disorders and general mortality in PD patients and showed clear, previously unreported trends to correlation between baseline depression and a following incidence of severe peritonitis (Table 3) and peritonitis-related mortality (Table 6). Moreover, the risk of death after a single episode of peritonitis was significantly higher in patients with a depressive background (Table 7).
Incidence of peritonitis was a strong independent predictor of peritonitis-related mortality and showed a clear trend to predicting overall mortality (Table 6), which is in agreement with previous studies (3). On the other side, to our knowledge, the direct correlation between time on PD at the time of the event and peritonitis-related mortality (Table 7) has not been reported previously. The incidence of severe peritonitis was particularly high in patients with a background of frequent infections and a longer follow-up on PD (Table 3), an observation that may provide an explanation for that finding.
Some relevant variables did not behave as predictors of peritonitis or peritonitis-related mortality and deserve some comment. Our results do not indicate an increased risk of presenting peritonitis in hypoalbuminemic patients (42), neither do they support a predictive role of plasma albumin levels for peritonitis-related mortality, as suggested by previous studies based on univariate strategies of analysis (4,12,16). The relatively low prevalence of severe hypoalbuminemia among our patients (Table 1) and better performance by other markers of malnutrition and inflammation (SGA, s-CRP) in the regression models may explain this discrepancy. On the other hand, the debate over the relative risk of PD-related peritonitis in patients with diabetes mellitus is still open after many years (43), but our results do not show even a minor trend to such an association. Finally, immunosuppressive drug therapy was independently associated with all-cause mortality (Table 6) but not with the risk of peritonitis or peritonitis-related mortality, and our results do not support recent reports (44) suggesting a high risk of peritonitis-related mortality in patients starting PD with a failing renal allograft, although, in this case, the validity of our conclusions may be limited by an evident lack of statistical potency.
In summary, peritonitis represents a significant cause of mortality in patients undergoing PD therapy. The etiologic agent is an essential predictor of peritonitis-related mortality but advancing age, female gender, poor residual renal function, a baseline inflammatory state (as estimated from s-CRP levels), malnutrition, a depressive background, and a high incidence of peritonitis are other significant predictors of this complication. Time on dialysis at the time of the event is associated with increased mortality after a single episode of peritonitis. Most of these risk factors are common to cardiovascular and peritonitis-related mortality, which may help to explain the high incidence of cardiovascular events as an immediate cause of death in patients with severe peritonitis.