
Abstract
Background
The potential risk for transmission of hepatitis C virus (HCV) by peritoneal dialysis (PD) has been studied previously, with conflicting results.
Methods
To assess whether HCV crosses the peritoneal membrane, the following determinations were performed in 16 patients (7 males, 9 females; mean age 41.8 years; mean time on PD 14 ± 15 months) undergoing PD: serum anti-HCV using second-generation enzyme-linked immunosorbent assay (ELISA), serum and PD fluid HCV RNA by nested polymerase chain reaction, HCV genotyping by restriction fragment length polymorphism, and serum HCV load by branched DNA assay.
Results
Anti-HCV was positive in 10 patients. Serum HCV RNA was positive in 7 anti-HCV-positive patients and negative in all anti-HCV-negative patients. Fluid HCV RNA was detected in 5 (71.4%) patients testing positive for serum HCV RNA and in none testing negative for serum HCV RNA. Serum HCV genotype was 1a in 3 patients and 1b in 4; PD fluid HCV genotype was 1a in 1 patient and 1b in 4. Genotypes in serum and fluid were concordant when both were positive. Serum viral load ranged from nondetectable by the quantitative method to 5.1 MEq genome/mL in patients with fluid infection, and 1.05 MEq and 29 MEq genome/mL in the remaining 2 patients without detectable HCV in PD fluid.
Conclusions
HCV crosses the peritoneal membrane and may be detected in the dialysate of PD patients with proven viremia. Although our study population was small for firm conclusions to be drawn, this passage does not seem to depend upon the serum viral load. Our data support the notion that PD fluid needs careful handling and local disinfection to prevent possible spreading of viruses, in the institutional and the domestic environments.
End-stage renal disease (ESRD) patients constitute a high-risk group for hepatitis C virus (HCV) infection and have high prevalence rates (1). In Argentina, the prevalence of hepatitis C infection in chronic hemodialysis (HD) patients is 27.9% (2), and in volunteer blood donors it is 0.8%. Other viruses, such as hepatitis B and HIV (3-7), can be recovered from peritoneal dialysis (PD) fluid, but published studies concerning the diffusion of HCV through the peritoneal membrane give conflicting results (8-11). The prevalence of this virus in the peritoneal effluent and the factors that can influence its presence have not been defined.
The purpose of the present study was to evaluate the presence of HCV in the peritoneal effluent of viremic patients under chronic PD and to determine if this fluid could be potentially infective.
Material and Methods
The population under study comprised all 16 patients (7 men, 9 women; mean age 41.8 years, range 18 – 61 years; on chronic PD for 14 ± 15 months) dialyzed in our unit during July 1997. No patient was excluded from the study. Three patients were on automated peritoneal dialysis (APD) and 12 were on continuous ambulatory peritoneal dialysis (CAPD) (Y-system double bag). The remaining patient had received a cadaveric renal transplant 24 hours before, stopped dialysis at that point, and was under full immunosuppression. No peritonitis during the previous month and no severe liver disease by clinical and/or histological criteria had been diagnosed in any of the patients.
Peritoneal transport was assessed using the standard peritoneal equilibration test (PET), anti-HCV antibodies in serum were determined using a second-generation enzyme-linked immunosorbent assay (ELISA) (Abbott Laboratories, Wiesbaden, Germany), and HCV RNA in serum and peritoneal fluid was determined by nested polymerase chain reaction (PCR). RNA was extracted (12) and PCR analysis was performed in all 16 patients, using primers for the 5’ non-coding region of the viral genome; nested amplification was carried out as described previously (13). Serum and peritoneal samples were taken simultaneously.
Peritoneal fluid (10 mL) was collected from the overnight bag from patients on CAPD and from the discard bag for APD. Blood samples were obtained simultaneously and centrifuged immediately. All samples were frozen at –20°C and processed within 30 days. Our laboratory personnel were blinded to the names and the previous known serology results.
In viremic patients, the viral genotype was determined in the blood and the dialysate by restriction fragment length polymorphism, applying Simmond's classification. The viral load was determined using Quantiplex HCV RNA branched DNA (Chiron Diagnostics, Emeryville, California, USA) v2.0 [quantification range 0.2 – 12 MEq genome/mL; detection limit 0.2 MEq genome/mL (200 000 Eq genome/mL)].
Results
Ten of the 16 (62.5%; 4 men, 6 women) patients were found to be positive for anti-HCV antibodies (Table 1). These 10 patients had tested positive before beginning chronic PD treatment; all had been on HD in the past (9 before 1991, the year when HCV testing was introduced in our country) and 9 had a functioning renal graft before returning to dialysis. In three of the latter, the graft had been removed before the study. No patient was under immunosuppression. Results of the PET studies in the HCV-positive patients were as follows: 1 low transporter, 1 high average, and the rest low average.
Patients with Serum Hepatitis C Virus (HCV) Antibodies and HCV RNA in Serum and Peritoneal Fluid
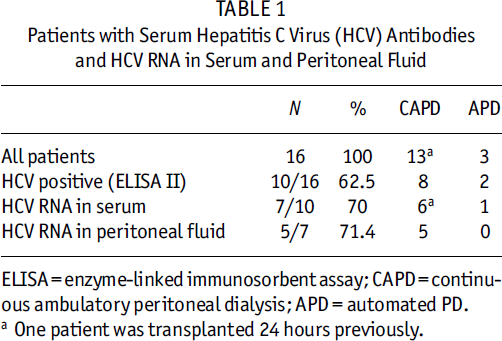
ELISA = enzyme-linked immunosorbent assay; CAPD = continuous ambulatory peritoneal dialysis; APD = automated PD.
One patient was transplanted 24 hours previously.
Of the 6 patients negative for HCV, 2 had never been hemodialyzed and the other 4 had been on HD for less than 1 year.
None of the 6 HCV-negative patients had demonstrable viremia, but viral sequences were found in the blood of 7/10 patients with positive serology for HCV (70%) (1 on APD, 1 recently transplanted, 5 on CAPD); classified according to PET, 1 was high-average and 6 were low-average transporters. In 5 of these 7 patients with viremia, HCV RNA (PCR) was found in the peritoneal fluid (71.4%); these 5 patients were on CAPD (Table 1).
When viremia was negative, HCV RNA determination by PCR was consistently negative in the peritoneal effluent.
Genotyping was performed in blood and in the peritoneal fluid in all cases in which HCV RNA was positive by nested PCR. The genotype found in blood was 1a in 3 cases and 1b in the other 4. Whenever HCV RNA tested positive in both blood and peritoneal fluid, the genotypes were identical (4/4 cases of 1b, 1/3 cases when the genotype was 1a).
The viral load varied from nondetectable to 5.1 MEq genome/mL in patients in whom the virus was recovered from the dialysate, and was 1.05 and 29 MEq genome/mL in the 2 cases in whom HCV RNA was not detected in the PD fluid. Hence, in this small sample, no obvious relationship emerged between viral load and detection of viral RNA (by PCR) in the peritoneal fluid (Table 2).
Results of Viral Studies in Each Patient
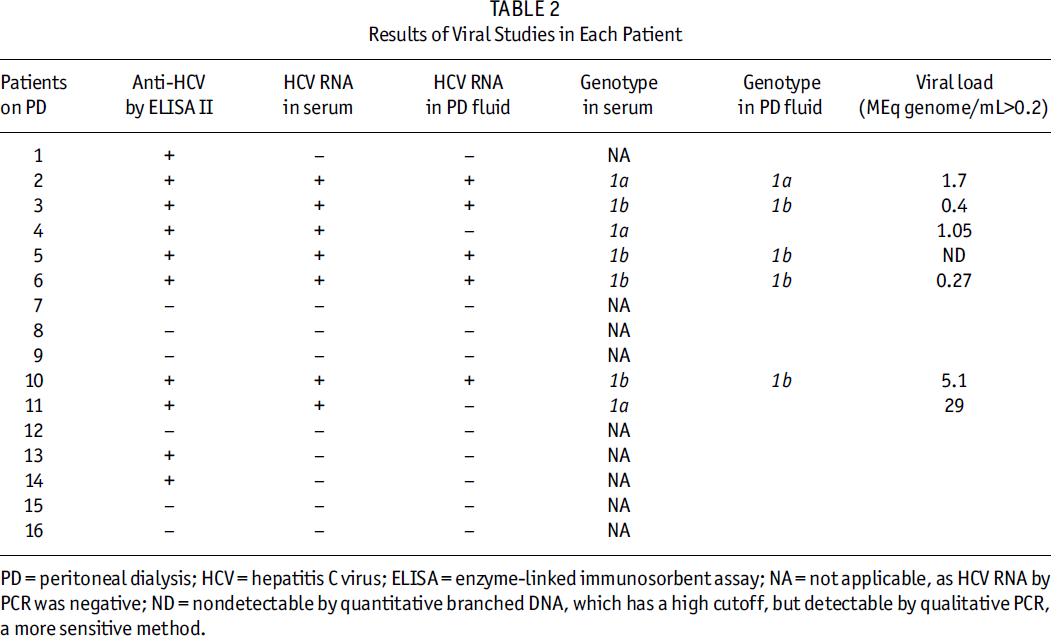
PD = peritoneal dialysis; HCV = hepatitis C virus; ELISA = enzyme-linked immunosorbent assay; NA = not applicable, as HCV RNA by PCR was negative; ND = nondetectable by quantitative branched DNA, which has a high cutoff, but detectable by qualitative PCR, a more sensitive method.
Discussion
Our study showed conclusively that HCV crosses the peritoneal membrane. In 5/7 patients with viremia, all on CAPD, the virus was isolated from peritoneal fluid. The virus was not recovered from PD fluid of 2 viremic patients on APD.
In patients with ESRD, the prevalence of HCV infection is lower in those who began their replacement therapy with PD than in those who started with HD, ranging from 2% to 29.7% (14-17). Our population presented a high prevalence of infection at the start of PD treatment, as could be expected in patients who had been on HD previously. The high proportion of patients in the study with a long previous history of HD or a failing kidney graft is no longer a common situation in Argentina, but when we started the PD program in 1995, it was offered only to patients with multiple access failures and to patients who did not want to return to HD after a failed graft.
Hepatitis C virus is an RNA virus belonging to the Flaviviridae family and measures 55 – 65 nm, with an inner core genomic region of 30 – 35 nm and a lipid envelope. The size of the HCV particles ought not to be, by itself, an obstacle for its passage through the peritoneal membrane. A complete B virus, considering its three components (the 42 nm Dane particle, the 22 nm spheres, the 22 nm filaments, and its length of 250 – 300 nm) is larger than the HCV, and has been detected in PD fluid (6,7). Another virus, HIV, although smaller than HCV, has also been recovered from peritoneal dialysate (3-5).
Few authors have investigated the presence of HCV in peritoneal fluid, but the results have been conflictive and may have depended upon the clinical scenario. While Caramelo et al. (9) did not find passage of the virus in 5 patients whose sera were positive for HCV RNA, Castelnovo et al. (11) found the virus in peritoneal fluid only in patients who suffered from severe liver damage, and other authors (8,10) have recovered the virus from the peritoneal fluid in varying proportions, ranging between 36% and 80% (Table 3).
Reported Studies on Recovery of Hepatitis C Virus (HCV) RNA from Peritoneal Dialysis (PD) Fluid
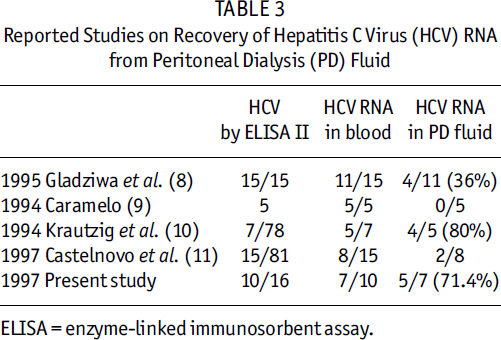
ELISA = enzyme-linked immunosorbent assay.
The total number of reported patients, including the present series, in whom viral RNA was detected by PCR in the blood and in whom the presence of HCV in the PD fluid virus was simultaneously investigated is 36; HCV RNA was detected in the dialysate in 15/36 (41.7%).
Krautzig et al. (10) recovered the virus in the peritoneal fluid in 80% of patients positive for HCV RNA in blood, but this result was obtained after repeated testing in the peritoneal fluid in three different samples, taken on different days, and in only one case were all three samples positive.
These conflicting results might suggest that the viral load or the prevailing genotypes, the frequency of testing, or even the permeability of the peritoneal membrane itself may have an influence on the appearance of the virus in peritoneal effluent. In our small population, however, the first of these factors was not related to viral passage, but further studies are needed to define these issues.
It is known that patients with peritonitis have a high flux of neutrophils, lymphocytes, and monocytes into the peritoneal cavity, and that there is continuous migration of cells, predominantly B and T lymphocytes, even in patients free of infection. In addition, HCV has the ability to replicate in lymphomononuclear cells, a property also shared by HIV in cultures from peritoneal macrophages (18,19).
The viral genotypes found in the blood samples of our population were those found in HD patients in our country, and the same genotypes were identified in the peritoneal fluid: 3/4 1b and 1/3 1a. This confirms that HCV crosses the peritoneal membrane. To our knowledge, this is the first study that investigated viral genotypes simultaneously in the serum and the peritoneal fluid, and that measured blood viral load at the same time. More extensive studies are necessary to define which variables influence the passage of the virus and thus to explain, retrospectively, the conflicting results published until now.
The explanation for the absence of PD fluid positivity in the two viremic patients on APD is unclear, but it could be related to a concentration of the virus below the detection limit of the method, due to greater volumes and less contact time. We did not concentrate the samples to perform determinations and this approach could have enhanced the results, as has been suggested (11).
The recovery of HCV from peritoneal fluid indicates that this fluid has to be subjected to universal precaution measures. Relevant to this point, the study by Krautzig et al. established that peritoneal dialysate remains positive for HCV RNA after a storage time of up to 24 hours at room temperature. These are important issues, not only for the procedures to be followed by the dialysis units but also for how peritoneal fluids should be handled at the patients’ homes, particularly when partners are involved in their care.
Conclusions
Our data confirm that HCV passes across the peritoneal membrane and may be detected in the dialysate of a high percentage of patients with proven viremia. This passage does not seem to depend upon the serum viral load, although the sample under investigation was too small to conclusively define this point. Our data support the notion that PD fluid needs careful handling and local disinfection to prevent possible spreading of viruses, in the institutional and the domestic environments.