
Abstract
Objectives
The aim of this study was to evaluate hepatic subcapsular steatosis (HSS) and its association with clinical parameters in nondiabetic continuous ambulatory peritoneal dialysis (CAPD) patients and in diabetic CAPD patients receiving intraperitoneal (IP) or subcutaneous (SC) insulin.
Design
Cross-sectional study.
Setting
A tertiary-care university hospital.
Patients
28 CAPD patients (17 males and 11 females; mean age 53.5 ± 14 years; mean CAPD duration 22.8 ± 9 months) were included in the study. 14 patients had type II diabetes mellitus and 14 were nondiabetics. In the diabetic group, 8 patients were receiving IP insulin and 6 were receiving SC insulin.
Outcome Measures
HSS was diagnosed on computed tomography without contrast administration. Other data collected were body mass index (BMI), weekly Kt/V, peritoneal equilibration test (PET) results, daily insulin dosage, duration of diabetes mellitus, duration of insulin treatment, dialysate glucose load, and serum findings for alanine aminotransferase, aspartate aminotransferase, albumin, and lipid profiles.
Results
HSS was detected in 5 of the 8 diabetics who were receiving IP insulin. None of the diabetics receiving SC insulin and none of the nondiabetic patients exhibited HSS. Daily insulin dosage [108 (95 – 108.5) vs 54 (36 – 72) U/day, p = 0.02], BMI [31 (30.5 – 36) vs 26.6 (26 – 30) kg/m2, p = 0.02], serum triglyceride level [194 (184 – 505) vs 69 (61 – 82) mg/dL, p = 0.04], and PET creatinine levels [D/P2 creat: 0.67 (0.54 – 0.74) vs 0.50 (0.50 – 0.56), p = 0.05; D/P4 creat: 0.75 (0.64 – 0.86) vs 0.60 (0.59 – 0.62), p = 0.02] were higher in diabetic patients receiving IP insulin who had HSS than in those who did not have HSS. PET glucose levels [D0/D2 glu: 0.40 (0.37 – 0.45) vs 0.50 (0.48 – 0.51), p = 0.03; D0/D4 glu: 0.36 (0.26 – 0.38) vs 0.44 (0.38 – 0.48), p = 0.04] were lower in diabetic patients receiving IP insulin who had HSS than in those who did not have HSS.
Conclusions
Our results suggest that IP insulin plays a more important role in the pathogenesis of HSS than glucose levels in diabetic CAPD patients. They also indicate that HSS is associated with higher daily insulin requirement, obesity, hypertriglyceridemia, and high peritoneal transport rate in diabetic CAPD patients receiving IP insulin.
Generalized intra-abdominal fat accumulation due to increased glucose load has been reported in patients on continuous ambulatory peritoneal dialysis (CAPD). It has been suggested that this fat accumulation increases the already high risk of cardiovascular disease in CAPD patients (1). In contrast to this generalized buildup, focal fat accumulation beneath the capsule of the liver is a rare finding associated with intraperitoneal (IP) insulin administration in diabetics who are on CAPD, and the clinical importance of this finding is unclear (2).
The aim of this study was to evaluate hepatic subcapsular steatosis (HSS) and its association with clinical parameters in nondiabetic CAPD patients and in diabetic CAPD patients receiving IP or subcutaneous (SC) insulin.
Materials and Methods
The study included 28 patients on CAPD (17 males, 11 females; mean age 53.5 ± 14 years; mean CAPD duration 22.8 ± 9 months). The exclusion criteria were malnutrition, hepatitis B or C virus infection, one or more episodes of peritonitis during the study period, history of excessive alcohol consumption, use of lipid-lowering drugs, and requirement for total parenteral nutrition. Informed consent was obtained from each participant and the study was conducted in accordance with the Declaration of Helsinki. Our institution's Clinical Investigation Ethics Committee approved the study protocol.
Fourteen patients had type II diabetes mellitus (DM) and 14 were nondiabetics. To control blood glucose levels, 8 of the diabetics were receiving IP insulin and 6 were receiving SC insulin. The patients on SC therapy received regular insulin three times daily (before each meal) and NPH insulin once in the evening. The patients on IP insulin received regular insulin four times daily, with one dose injected into each dialysis bag before fluid exchange. For each of the 14 diabetic patients, the insulin dose was adjusted in order to keep serum HbA1c below 7%.
Each patient's daily CAPD regimen involved 4 – 5 daily exchanges of 2 – 2.5 L standard dialysis solutions containing 1.36%, 2.27%, or 3.86% dextrose. Total weekly Kt/V was kept at 2.1 ± 0.1.
Hepatic subcapsular steatosis was diagnosed on spiral computed tomography (CT) scans of the liver (Somatom AR Star; Siemens, Erlangen, Germany), without oral or intravenous contrast administration. These scans were done as part of routine CAPD follow-up. The entire liver was examined using 5-mm slice thickness; in each case, the maximum dimensions of HSS were measured.
The serum parameters investigated were alanine aminotransferase, aspartate aminotransferase, albumin, and lipid profile, and these levels were also determined as part of regular CAPD follow-up. The average values for the 3 months prior to the study were recorded. These laboratory parameters were measured using colorimetric assays in a Roche Modular biochemical automatic analyzer (Roche Diagnostics, Indianapolis, Indiana, USA).
For each of the 28 cases, body mass index (BMI) was calculated in kilograms per meter squared and a standard peritoneal equilibration test (PET) was performed using the method described by Twardowski et al. (3).
For each of the diabetic patients, duration of DM, duration of insulin treatment, route of insulin administration (IP or SC), and daily insulin dosage were recorded.
All results are expressed as mean ± SD. Differences between group findings were analyzed using Student's t-test, Mann–Whitney U test, and chi-square test. The Pearson or Spearman correlation coefficient was used to express correlations between variables.
Results
There were no significant differences between the diabetic group (n = 14) and the nondiabetic group (n = 14) with respect to mean age, sex distribution, or mean BMI. Of the laboratory parameters, only mean serum albumin level was lower in the diabetic group than in the nondiabetic group (35 ± 3 vs 43 ± 12 g/L respectively, p = 0.039). There was no significant difference between the groups’ mean PET results.
Table 1 shows the clinical characteristics, laboratory values, and PET findings for the diabetic patients, categorized according to route of insulin administration (IP vs SC). There were no significant differences between the IP subgroup (n = 8) and the SC subgroup (n = 6) with respect to age, duration of DM, or duration of insulin treatment. The IP subgroup had significantly higher mean values than the SC subgroup for daily insulin dosage (84.6 ± 27.9 vs 32.5 ± 27 U/day, p = 0.04), BMI (31.8 ± 3.0 vs 27.9 ± 3.3 kg/m2, p = 0.04), and serum triglyceride level (259.2 ± 161.0 vs 107.0 ± 56.0 mg/dL, p = 0.03), but had lower mean Kt/V than the SC subgroup (2.08 ± 0.13 vs 2.2 ± 0.12, p = 0.05). The ratio of dialysate creatinine level to plasma creatinine level at 2 hours (D/P2 creat) was higher in the IP subgroup than in the SC subgroup (0.59 ± 0.11 vs 0.46 ± 0.12, p = 0.05); this difference was even more significant at 4 hours (D/P4 creat 0.69 ± 0.10 vs 0.53 ± 0.10, p = 0.01). The ratio of initial dialysate glucose level to dialysate glucose level at 2 hours (D0/D2 glu) was lower in the IP subgroup than in the SC subgroup (0.45 ± 0.10 vs 0.54 ± 0.10, p = 0.05); this difference was also more significant at 4 hours (D0/D4 glu 0.36 ± 0.10 vs 0.46 ± 0.11, p = 0.01).
Comparison of Clinical Characteristics, Laboratory Values, and Peritoneal Equilibration Test Results in Diabetic Patients Divided According to Route of Insulin Administration [Intraperitoneal (IP) or Subcutaneous (SC)]
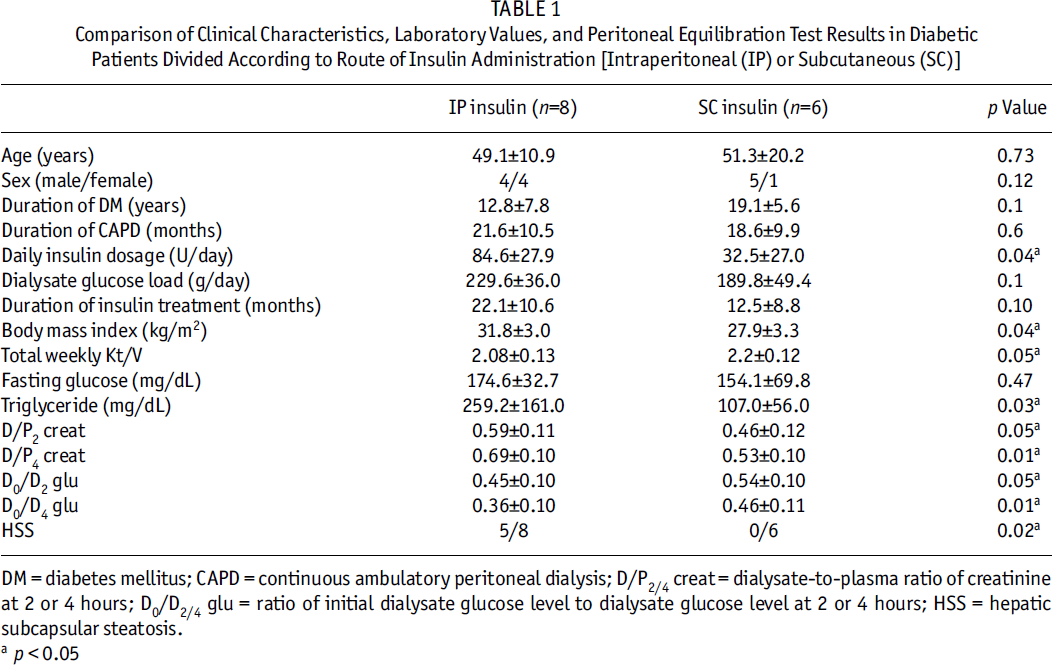
DM = diabetes mellitus; CAPD = continuous ambulatory peritoneal dialysis; D/P2/4 creat = dialysate-to-plasma ratio of creatinine at 2 or 4 hours; D0/D2/4 glu = ratio of initial dialysate glucose level to dialysate glucose level at 2 or 4 hours; HSS = hepatic subcapsular steatosis.
p < 0.05
Hepatic subcapsular steatosis was detected in 5 (62%) of the 8 diabetics who were receiving IP insulin. The maximum thickness of the fatty rim in the 5 HSS cases ranged from 7 to 12 mm (mean 9.8 ± 1.9 mm). None of the diabetics receiving SC insulin and none of the nondiabetic patients exhibited HSS.
Hepatic subcapsular steatosis was positively correlated with BMI (r = 381, p = 0.045), daily insulin dosage (r = 622, p = 0.001), serum triglyceride level (r = 543, p = 0.004), and PET creatinine findings (D/P2 creat: r = 722, p = 0.04; D/P4 creat: r = 741, p = 0.02), whereas it was negatively correlated with PET glucose findings (D0/D2 glu: r = –612, p = 0.02; D0/D4 glu: r = –669, p = 0.009) in diabetics receiving IP insulin. Daily insulin dosage [108 (95 – 108.5) vs 54 (36 –72) U/day,p= 0.02], BMI [31 (30.5 – 36) vs 26.6 (26 – 30) kg/m2,p = 0.02], serum triglyceride level [194 (184 – 505) vs 69 (61 – 82) mg/dL,p = 0.04], and PET creatinine findings [D/P2 creat: 0.67 (0.54 – 0.74) vs 0.50 (0.50 – 0.56),p = 0.05; D/P4 creat: 0.75 (0.64 – 0.86) vs 0.60 (0.59 – 0.62), p = 0.02] were higher in diabetic patients receiving IP insulin who had HSS than in those who did not have HSS. PET glucose findings [D0/D2 glu: 0.40 (0.37 – 0.45) vs 0.50 (0.48 – 0.51),p = 0.03; D0/D4 glu: 0.36 (0.26 – 0.38) vs 0.44 (0.38 – 0.48),p = 0.04] were lower in diabetic patients receiving IP insulin who had HSS than in those who did not have HSS (Table 2).
Clinical Characteristics of Diabetic Patients Receiving Intraperitoneal Insulin Who Have or Do Not Have Hepatic Subcapsular Steatosis [HSS(+) & HSS(–)]
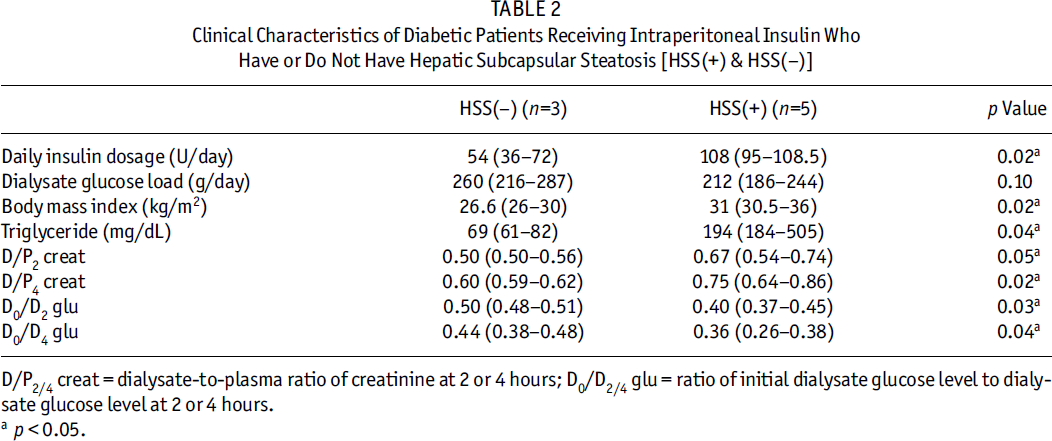
D/P2/4 creat = dialysate-to-plasma ratio of creatinine at 2 or 4 hours; D0/D2/4 glu = ratio of initial dialysate glucose level to dialysate glucose level at 2 or 4 hours.
p < 0.05.
Discussion
Intraperitoneal administration of insulin is preferred over the SC route in diabetic patients on CAPD (4). It has been suggested that IP insulin induces better metabolic control than SC insulin because the IP route is associated with greater insulin sensitivity in the peripheral circulation and lower levels of endogenous glucose production by the liver (5). However, IP insulin administration in diabetics on CAPD has potential drawbacks, the main ones being increased risk of peritonitis, deterioration of serum cholesterol profile, and HSS (6).
Hepatic subcapsular steatosis is a rare form of fat accumulation in the liver that was first described by Wanless et al. in 11 of 12 autopsied diabetic CAPD patients who had been treated with IP insulin (2). In our study of nondiabetic CAPD patients and diabetic CAPD patients receiving IP or SC insulin, we observed HSS only in the diabetic patients who were receiving their insulin via the IP route. High concentrations of glucose and insulin in the peritoneal cavity have been suggested as causal factors in the pathogenesis of HSS (7). We found no differences in dialysate glucose load between diabetic CAPD patients receiving IP insulin who had HSS and those who did not have HSS, but mean daily insulin dosage in the diabetics with HSS and receiving IP insulin was roughly twice as high as that in the diabetics without HSS and receiving IP insulin. Katz and co-workers reported that high glucose load alone is probably not sufficient to induce hepatosteatosis because of the low level of hepatic glucokinase in humans (8). Our findings suggest that IP insulin dosage plays a more important role in the pathogenesis of HSS than dialysate glucose load. The higher daily insulin dosage in our IP insulin subgroup versus the SC subgroup may be the basis for the association between HSS and IP insulin administration.
Our analysis also revealed higher peritoneal transport rates in the diabetic CAPD patients treated with IP insulin than in those treated with SC insulin. Previous work has shown that high peritoneal transport rate is more prevalent in diabetic CAPD patients than in nondiabetic CAPD patients, and that high peritoneal permeability is associated with increased mortality and morbidity in patients on CAPD (9). The mechanism responsible for increased peritoneal transport rate in diabetic patients is poorly understood. One study that compared diabetic patients on CAPD who were receiving IP insulin with those receiving SC insulin revealed no significant differences with respect to ultrafiltration, solute clearance rates, or glucose absorption from the dialysate (10). However, insulin is known to be a mitogenic substrate, and long-term IP insulin use can lead to peritoneal fibrosis (11). Fibrotic changes might at least partially explain the high peritoneal transport rates we observed in our diabetic patients treated with IP insulin.
The clinical manifestations of HSS are not yet clear. Our findings identify daily insulin dosage, BMI, triglyceride levels, and peritoneal transport rates were higher in diabetic CAPD patients receiving IP insulin who had HSS than in those who did not have HSS. Nevalainen et al. also observed that the amount of HSS increases when peritoneal transfer rate is high in diabetic CAPD patients treated with IP insulin (12). Higher glucose and insulin absorption due to greater peritoneal permeability might explain why obesity and hypertriglyceridemia were associated with HSS in the diabetic patients in our study who were receiving IP insulin and had high peritoneal transport rates.
It has also been suggested that fatty liver can be considered the hepatic consequence of insulin resistance/metabolic syndrome (13). We suggest that IP insulin administration in diabetic CAPD patients with high peritoneal transport rate leads to HSS, which is associated with clinical conditions similar to those seen in insulin resistance/metabolic syndrome. Avoidance of IP insulin administration in diabetics on CAPD who have high peritoneal transport rates may prevent the development of HSS and its associated metabolic abnormalities.
Ultrasonography can also be used to diagnose fatty liver. Sonographic changes tend to parallel biochemical and clinical dysfunction. However, the sonographic pattern of fatty infiltration (especially focal fatty infiltration) can change from hyperechogenic to hypoechogenic foci, and this can make diagnosis of HSS difficult. In our study, we used non-contrast CT to assess for fat infiltration in the liver because research has shown that CT attenuation in the hepatic parenchyma is strongly correlated with the amount of triglyceride in liver biopsy specimens obtained in efforts to diagnose fatty liver (14). Non-contrast CT is considered the reference standard imaging modality for diagnosing fatty infiltration of the liver (15).
The main limitation in our study was the small size of the patient population. Investigations of larger groups will be needed to determine exactly how HSS is related to metabolic abnormalities in diabetic patients on CAPD.
In conclusion, our results suggest that IP insulin plays a more important role in the pathogenesis of HSS in the setting of CAPD than glucose levels in diabetic CAPD patients. They also indicate that HSS is associated with higher daily insulin requirement, obesity, hypertriglyceridemia, and high peritoneal transport rate in diabetic CAPD patients receiving IP insulin. Attention should be focused on screening for the development of HSS in diabetic patients on CAPD who are receiving insulin via the IP route.