
Abstract
Over the past 30 years, the focus of peritoneal dialysis research has changed from the technical issues related to the establishment of clinical peritoneal dialysis to complex problems of peritoneal membrane biology. Here, we present how these research topics developed, discuss their significance for clinical science, and outline future challenges for peritoneal dialysis research.
Keywords
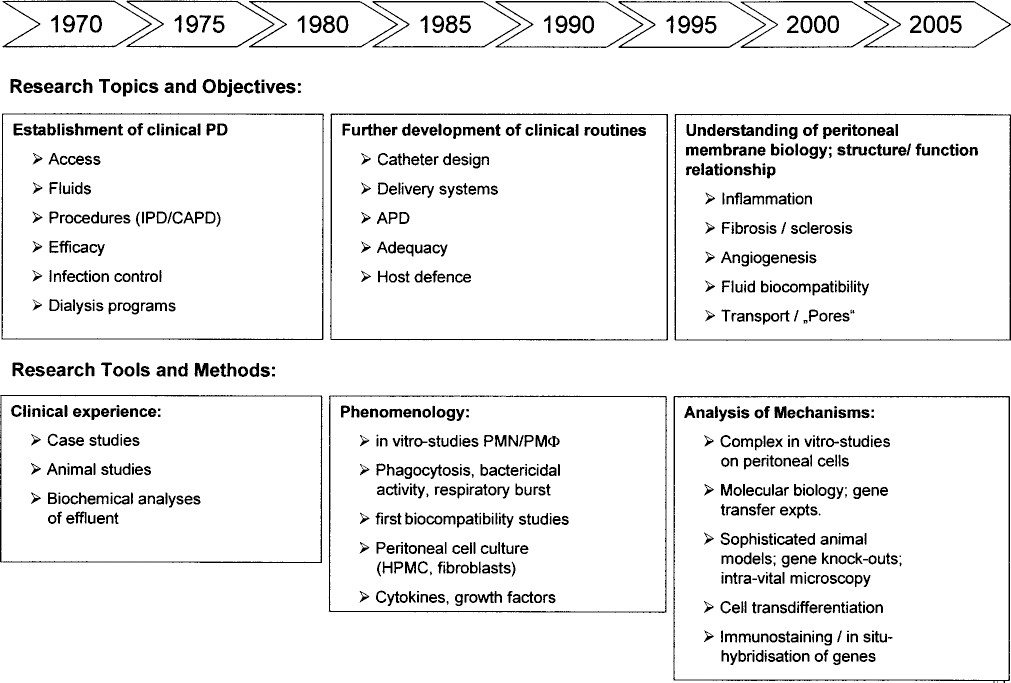
Development of peritoneal dialysis research over time.
From the mid-1980s to the early 1990s, further development of clinical routines in PD was achieved, with CAPD as the routine treatment and automated PD techniques being developed and refined. Catheters, connectors, and delivery systems underwent further sophistication, and clinical research was focused on both adequacy and host defense. Also during that period, the first research articles on PD fluid biocompatibility were published, most using peripheral blood leukocytes as a model system to assess their viability and function following exposure to unused dialysis solutions (1). In parallel, basic research on host defense began in earnest, at that time mostly investigating the phenotypes and functions of peritoneal macrophages, monocytes, and neutrophils, such as their capacity for phagocytosis, respiratory burst activation, and bacterial killing. Much attention was directed at humoral immunity but, in addition to soluble factors such as opsonins, immunoglobulins, and complement factors, initial data on cytokine and growth factor concentrations in PD patients were also generated. Information on peritoneal microanatomy and histology was obtained using peritoneal biopsies or following autopsies; however, there was no systematic prospective evaluation of morphological changes that occur over the course of PD.
A major breakthrough to a better understanding of the complex interactions between leukocytes and resident cells of the peritoneal membrane was finally made possible by the establishment and development of peritoneal cell culture (2,3). Since then, complex in vitro studies with peritoneal mesothelial cells and fibroblasts have enormously increased our knowledge of the complexity of peritoneal cell biology and the cytokine/growth factor networks that regulate peritoneal host defense (4). They have also created a new platform for more complex and relevant biocompatibility studies (5). The latter have induced substantial momentum toward the development of novel dialysis solutions, which first underwent extensive preclinical screening (6).
In the past decade, the increasing availability of specific immunoassays and molecular biology techniques has finally enabled a transition from pure phenomenology to the era of analyzing the underlying mechanisms of the observed phenomena. What we need to learn and understand is the sequence of events leading to both morphological and functional changes in the peritoneum during long-term PD, changes that ultimately result in the loss of its function as a dialyzing membrane. The corresponding area that is currently a hot spot in basic PD research is analysis of the interactions and interrelationships between inflammation, angiogenesis, and fibrosis. Most of this work is still based on cell culture experiments; however, an increasing number of research groups are meanwhile combining in vitro studies with sophisticated animal models to more closely simulate the specific constellation of the dialyzed peritoneum. In parallel, the Peritoneal Biopsy Registry has begun to deliver a clearer picture of the morphological changes occurring during PD, thereby also hinting at potential influencing factors, such as duration of therapy, glucose exposure, and infectious complications (7). The complexity of the problem is further illustrated by the possibility that, during PD, cells of the peritoneal membrane may undergo a transition of their phenotype (8), the significance and mechanisms of which require further clarification. Overall, we need to realize, however, that we are only at the very beginning of a better understanding of structure–function relationships that might eventually create a basis for potential therapeutic interventions.
The research area that has most directly created an impact on treatment practice is solution development and biocompatibility. It has to be said, however, that it has taken more than 20 years from the first report on solution bioincompatibility (1) until the large-scale introduction of improved solutions into clinical routine, which is presently ongoing in Europe and parts of Asia and is only about to start in North America. It was a long time from first identifying the relative importance of obvious pitfalls in the composition of conventional PD fluids (acidic pH, hyperosmolality, high glucose content) that lead to acute disturbances of peritoneal cell functions, to the emerging concept of chronic bioincompatibility that is most likely relevant to actual patient outcomes. Again, it has taken many years from the first report on the in vitro toxicity of glucose degradation products (GDPs) (9) to more complex studies in peritoneal cells (10), and finally to clinical trials with modern, GDP-depleted fluids that indicate improved biocompatibility, albeit mostly using surrogate markers such as ex vivo cell function and effluent cancer antigen 125 concentrations, or subjective parameters such as reduction in inflow pain (11-16). From these clinical studies with novel solutions it has become increasingly apparent that we will have to redefine our concept of what the “normal” values of, for example, mediator effluent concentrations from the dialyzed peritoneum, really are, because our prior experience is based solely on data derived from treatment with solutions that are clearly unphysiological. Moreover, the fact that we are looking at the dialyzed peritoneum of a uremic patient is almost certainly having an impact of its own since the data from the Biopsy Registry indicate that changes already occur in the nondialyzed uremic peritoneum and in the patient undergoing hemodialysis (7).
In summary, there are many lessons we have learned from basic research, but even more things we still need to know:
We have a clearer concept of peritoneal cell biology, with its complex interactions and feedback loops involved in the control of peritoneal host defense and inflammation, but we still need to learn more about the relationship between inflammation, angiogenesis, and fibrosis as a basis for potential therapeutic interventions.
A systematic evaluation of peritoneal microstructure in the course of PD is already under way (e.g., biopsy registry); however, we still do not have an integrated concept of structure–function relationships and the impact of PD.
A broad database on PD fluid biocompatibility is already available and new dialysis solutions are presently being introduced into clinical routine; however, we still need to establish their true value by assessing clinical end points in prospective clinical studies.