
Abstract
The number of end-stage renal disease (ESRD) patients with diabetes mellitus has increased dramatically during the past few years and, in many countries, diabetes has become the most important cause of ESRD in patients admitted to dialysis. Furthermore, compared to nondiabetic patients, diabetic patients continue to suffer from more frequent and severe comorbidity and complications, including cardiovascular disease, poor fluid balance, worse quality of life, as well as high morbidity and mortality after initiation of dialysis. These systemic problems in diabetic patients should influence the dialysis prescription. In addition, the structure and transport properties of the peritoneal membrane may deteriorate as a consequence of diabetes. Thus, both the systemic and the peritoneal consequences of diabetes influence the dialysis prescription in diabetic patients. In this brief review, we discuss the care of diabetic ESRD patients on peritoneal dialysis — which, compared with hemodialysis, has both advantages and disadvantages in this group of patients — focusing on the special needs for intense and integrated care involving individualized dialysis prescription as well as care of diabetic complications and comorbidity in this diseased patient group.
The main topic of this brief review is integrated dialysis prescription and care to improve the outcomes for this group of patients.
Adequacy of Dialysis
After the ADEMEX study, small solute clearances are no longer the only factor defining dialysis adequacy in peritoneal dialysis (PD) patients. Other aspects, such as fluid and balance, calcium and phosphate control, management of comorbidity, etc., need much more attention (Table 1). With respect to the impact of small solute clearances on outcome in diabetic patients, analysis of the diabetic subgroup of the ADEMEX study showed results identical to the whole study, with no improvement in patient survival with increased peritoneal Kt/V urea and creatinine clearance (2). Similar to other patient groups, residual renal function seems to be equally important for outcome in diabetic PD patients and preservation of residual renal function is an obvious goal also in diabetics on PD.
Integrated Care for Diabetic Peritoneal Dialysis (PD) Patients
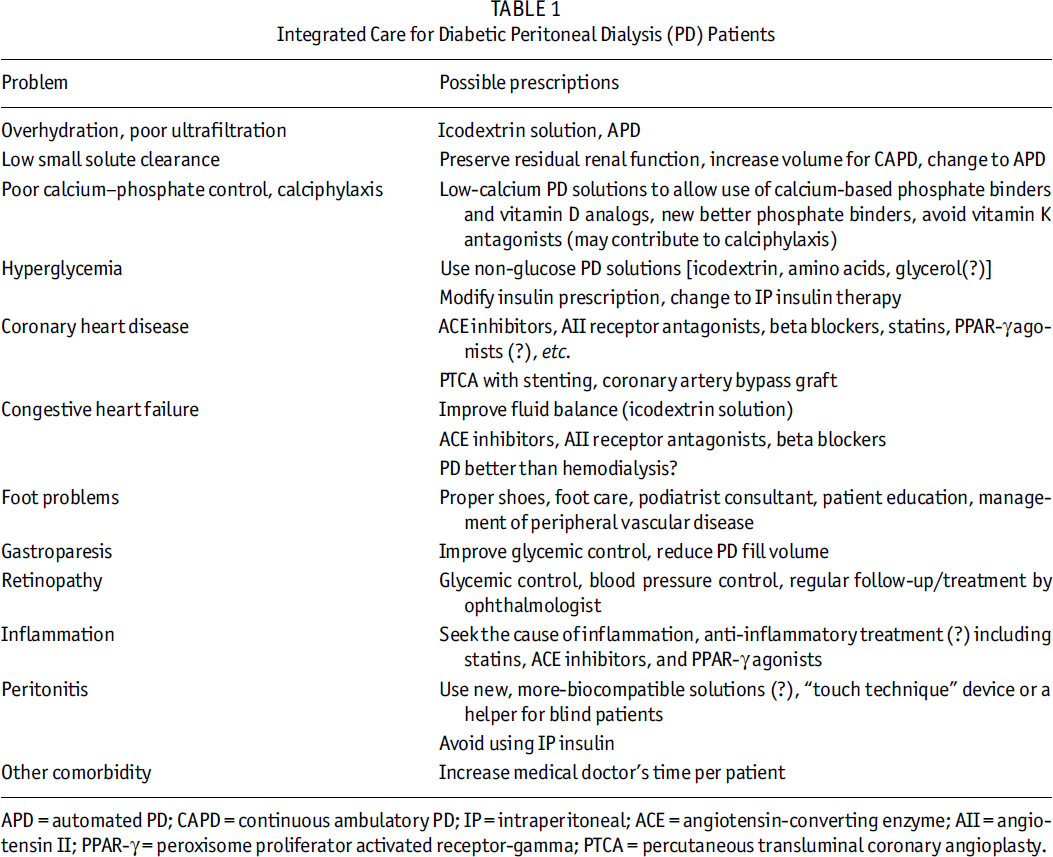
APD = automated PD; CAPD = continuous ambulatory PD; IP = intraperitoneal; ACE = angiotensin-converting enzyme; AII = angiotensin II; PPAR-γ = peroxisome proliferator activated receptor-gamma; PTCA = percutaneous transluminal coronary angioplasty.
Compared with nondiabetic PD patients, experimental and clinical studies suggest that diabetic PD patients are more likely to develop progressive increase in peritoneal transport of small solutes, loss of ultrafiltration, and peritoneal fibrosis. The load of glucose and glucose degradation products in PD fluids are believed to accelerate excess accumulation of advanced glycation end-products (AGEs) in the peritoneum during treatment with continuous ambulatory peritoneal dialysis (CAPD), and it is possible that high levels of AGEs induced by diabetes per se may further contribute to the changes in peritoneal membrane structure and function in diabetic patients on PD. However, results of clinical studies differ with respect to whether diabetics have increased peritoneal transport rates, and some studies show no differences in initial peritoneal transport characteristics between diabetic and nondiabetic patients, suggesting that diabetes does not always cause alterations in peritoneal membrane function.
The patient's peritoneal small solute transport characteristics will influence the optimal dialysis prescription with respect to ultrafiltration and small solute clearances and, furthermore, a high peritoneal transport rate has been identified as an important risk factor for both PD technique failure and mortality. Although the reasons for this are not established, several different mechanisms may contribute, in particular the association between a high peritoneal transport rate and comorbidity (including diabetes), and the more rapid glucose absorption resulting in impaired fluid and sodium removal, contributing to chronic fluid overload, which is associated with left ventricular hypertrophy and left ventricular dysfunction in PD patients.
Choice of Dialysis Solutions
As icodextrin is a solution containing a spectrum of high molecular weight polysaccharides that are slowly absorbed across the peritoneal membrane, it has been suggested that certain patient groups such as diabetics may benefit from the use of such a non-glucose solution. Chronic use of icodextrin in the long nighttime dwell can reduce serum insulin levels and increase insulin sensitivity in CAPD patients. In a prospective open-label study (3) of 17 PD patients (12 diabetics) who were on the verge of being transferred to hemodialysis (HD) because of symptomatic fluid retention, daily use of icodextrin significantly improved peritoneal ultrafiltration and extended PD technique survival in PD patients. The diabetic patients also experienced improved glycemic control. In addition, in a 12-week, three daily exchanges, diabetic, PD rat model, AGE formation in peritoneum was lower with the use of icodextrin-based solution compared to glucose-based solutions (4). Thus, the use of icodextrin may be helpful in slowing the deterioration of the peritoneal membrane, as well as in keeping better glycemic control and ultrafiltration volume in diabetic PD patients. In addition, compared with the conventional PD solutions, new more biocompatible, low glucose degradation product, and/or bicarbonate-buffered pH-neutral PD solutions have been reported to have less-negative effects on peritoneal membrane structure and function in animal models, improved dialysate levels of effluent markers of peritoneal membrane status in clinical studies, and have also been reported to improve peritoneal host defense.
Glycemic Control
Glycemic control in diabetic ESRD patients is as important as in the early stage of diabetes, and perfect glycemic and metabolic control is an obvious goal of therapy in uremic diabetics to reduce morbidity and mortality. During CAPD therapy with conventional glucose-based PD solutions, glucose absorption from the dialysate is about 90 – 140 g/day; thus, an extra amount of insulin for each bag exchange is required to maintain adequate glycemic control. As one of the advantages of PD for diabetic ESRD patients, intraperitoneal insulin therapy with painless administration offers better glycemic control and insulin sensitivity than subcutaneous insulin (5). However, intraperitoneally administered insulin may result in an increased risk of peritonitis due to contamination and may also have some negative metabolic side effects, including increased low density lipoprotein cholesterol and reduced high density lipoprotein (5), and has been reported to be associated with hepatic subcapsular steatosis in a few cases (6), which have limited its use. Recently, Marshall et al. (7) reported the results of continuous glucose monitoring in eight insulin-treated diabetic CAPD patients with different dialysis regimes in three phases: phase 1, with four exchanges of modern, biocompatible, glucose-based PD solution (three bags of Physioneal 1.36% and one of 3.86%); phase 2, with conventional, bioincompatible, glucose-based PD solutions (Dianeal) of similar concentration; and phase 3, with two exchanges of 1.36%, biocompatible, glucose-based PD solution, one of amino acid solution (Nutrineal), and one of icodextrin solution (Extraneal). (Dianeal, Nutrineal, and Extraneal manufactured by Baxter Healthcare, Castlebar, Ireland.) The last combination resulted in a much better glycemic control.
Comorbidity
Cardiovascular disease (CVD) is the main clinical problem in diabetic dialysis patients. Among dialysis patients with a history of myocardial infarction, one third of patients were diabetics and more than half of them died of heart disease within 2 years (8). As the cardiovascular conditions of diabetic patients are already severely impaired before they start dialysis, it seems that the clinical care during the predialysis period is even more important among diabetic patients, even though our present clinical tools may be insufficient to reverse the increased risk of CVD among diabetic ESRD patients. In this context, it is of interest that, among patients with type 2 diabetes on CAPD therapy, serum ACE activity was associated with an increased risk for macroangiopathy and was an independent predictor for mortality (9). Inhibition of ACE may thus have a beneficial effect on the outcome of these patients. In addition, peroxisome proliferator activated receptor-gamma (PPAR-γ) agonists (such as rosiglitazone or pioglitazone) have beneficial effects on insulin resistance and the lipid profile, and furthermore may have anti-inflammatory effects. Therefore, their role in treating the severe CVD complications in diabetic PD patients should be evaluated in further clinical trials. Compared with HD, there are several potential benefits of PD with respect to preventing CVD events through better volume regulation, reduced blood pressure, fewer electrolyte disturbances, and reduced cardiac workload. However, recent reports using the USRDS data showed conflicting results. Stack et al. (10) found that diabetic PD patients with congestive heart failure (CHF) had bad outcome compared with HD, suggesting that PD may not be the optimal choice for new ESRD patients, whereas Trespalacios et al. (11) reported