
Abstract
Background
This study was undertaken to investigate the effect of long-term blood pressure (BP) reduction, achieved with salt restriction and strict volume control, on frequency and regression of left ventricular hypertrophy (LVH) in long-term peritoneal dialysis (PD) patients.
Methods
56 patients who had been treated for more than 2 years under our care were enrolled. After echocardiographic (Echo) evaluation, 46 patients were included in the follow-up study. In our unit, we aim to keep patients’ BP below 130/85 mmHg and cardiothoracic index below 0.50. To reach these targets, moderate salt restriction is advised, and if necessary, hypertonic PD solutions are used. Echo was performed at the beginning of the study (after a mean period of 36 months on PD) and at the end of the prospective follow-up period (24 months later).
Results
At the time of the first Echo, LVH was detected in only 8 (21%) patients. Residual urine volume was significantly decreased compared to data taken when they first started PD (658 ± 795 vs 236 ± 307 mL/day). Mean left ventricular mass index (LVMI) was 107 ± 26.5 g/m2. LVMI was significantly decreased at the end of the follow-up in patients who had LVH at baseline. No LVH developed in patients who had normal LVMI at baseline.
Conclusion
Our results indicate that control of hypertension is possible when extracellular fluid volume is kept under control using hypertonic PD solutions in case of recruitment in addition to salt restriction in long-term PD patients. Sustained normovolemia is associated with low incidence and regression of LVH.
We previously showed that effective blood pressure (BP) control with antihypertensive drugs alone is not possible without appropriate volume control in hypertensive PD patients (3). Recently, it was claimed that control of BP in these patients becomes more difficult as residual renal function (RRF) declines (4). These authors therefore suggested that efforts should be made to preserve renal function in long-term PD patients. However, in our experience, strict volume control affects RRF negatively.
The aim of the present study was to investigate whether long-term BP reduction (BP < 130/85 mmHg) and preservation of cardiac function can be achieved by volume control with salt restriction and without drugs, despite decreased renal function.
Material and Method
Among the 103 PD patients under our care in 1999, we selected for further evaluation those patients who had been treated for more than 2 years (n = 56). After echocardiographic study (baseline Echo), 10 patients were excluded because of serious valvular cardiac disease (n = 2), previous myocardial infarction with low ejection fraction (n = 4), amyloidosis (n = 3), and constructive pericarditis (n = 1). The remaining 46 patients were included in the follow-up study after informed consent was obtained. Cardiovascular disease was present in 13% of the patients. The cause of end-stage renal disease was diabetes in 5, chronic glomerulonephritis in 6, hypertension in 3, reflux nephropathy in 2, and unknown etiology in the remaining patients.
At the time of the baseline Echo, BP, blood chemistry, peritoneal membrane transport characteristics (peritoneal equilibration test), weekly Kt/V urea and total creatinine clearance, residual urine volume, and dialytic fluid removal were recorded. Blood pressure was measured with a manual sphygmomanometer. Measurements were taken in the seated position after 5 minutes’ rest, by an experienced nurse. Normal BP was defined as systolic BP under 130 mmHg and diastolic BP under 85 mmHg.
Routine visits were made every 2 months, during which B P, body weight, residual urine volume, daily ultrafiltration volume, serum albumin, and hematocrit were measured. Every 6 months, Kt/V urea and peritoneal equilibration tests were performed and cardiothoracic index on chest x-ray was measured.
Our Volume Policy
In our dialysis unit, we aim to keep patients’ BP below 130/85 mmHg and cardiothoracic index below 0.50. To reach these targets, moderate salt restriction (NaCl intake 4 – 5 g/day) is advised. If necessary, hypertonic PD solutions are used. The glucose concentration of the hypertonic solution (2.27% or 3.86% glucose) is prescribed at the discretion of the treating physician. If in doubt, we use a “captopril test,” as described previously (5). In hypervolemic patients with urine output of more than 500 mL per day, furosemide is added.
Echocardiography (Echo)
Echocardiography was performed by the same echocardiographer using a Hewlett-Packard (Andover, Massachusetts, USA) ultrasonoscope with a 2.5 MHz transducer. M-mode, two-dimensional Doppler recordings were obtained simultaneously with electrocardiography according to the recommendation of the American Society of Echocardiography. Left ventricular muscle mass (LVM) was calculated using the equation described by Devereux and Reichek (6): LVM = 1.04 x [(IVS + LVDd + PWT)3 – (LVDd)3] – 13.6 (g), where IVS is interventricular septum thickness, LVDd is left ventricular end diastolic diameter, and PWT is posterior wall thickness. Left ventricular hypertrophy was defined as LVM (indexed to a standard body surface area) greater than 131 g/m2 in males and 100 g/m2 in females. Echocardiography was performed at the beginning of the study (after a mean period of 36 months on dialysis) and at the end of the prospective follow-up period (24 months later).
Statistical Analysis
Results are given as mean ± SD. Comparison of means and percentages was estimated by the unpaired two-tailed Student's t-test or Mann–Whitney U test, as appropriate. Calculations were made using SPSS 9.0 statistical software (SPSS Inc., Chicago, Illinois, USA) for Windows operating system (Microsoft Corp, Redmond, Washington, USA). Only variables significant at a p value less than 0.05 were kept in the model.
Results
Of the included patients, 38 completed the prospective part of this study [4 were on automated PD treatment and the rest on conventional continuous ambulatory PD (CAPD)]. During the mean 24 months (24 ± 3 months) of follow-up, 2 patients died (1 by acute myocardial infarction, the other by sudden death) and 6 patients were converted to hemodialysis because of recurrent bacterial peritonitis (n = 1), fungal peritonitis (n = 2), ultrafiltration failure (n = 1), and inadequate dialysis (n = 2).
There were 22 female and 16 male patients. Mean age at the start of PD was 47 (23 – 71) years. The main outcome data are presented in Table 1. In the first column, we give the mean values at the start of dialysis treatment, in the second column values obtained 36 (22 – 43) months before the prospective follow-up study, and in the third column values obtained after 24 months of follow-up.
Clinical and Laboratory Data of the Study Patients (n = 38)
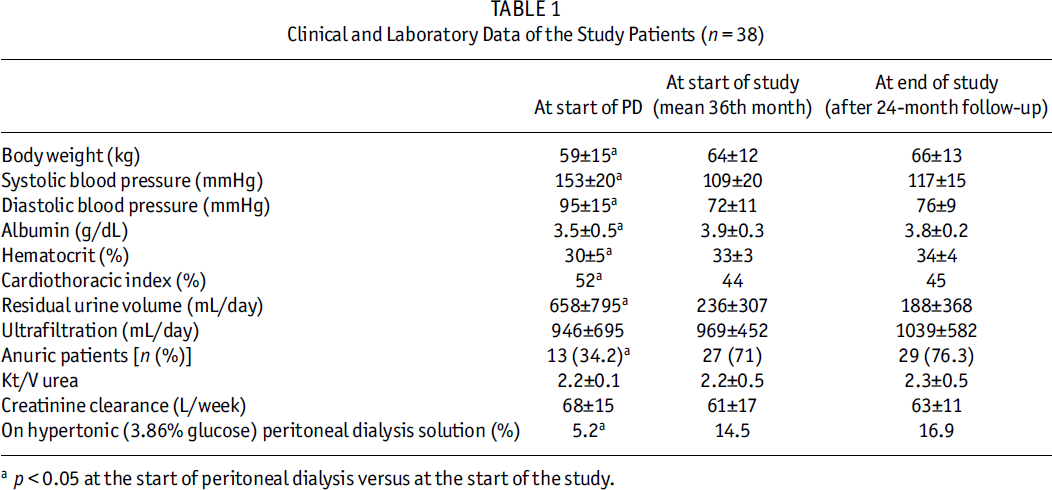
p < 0.05 at the start of peritoneal dialysis versus at the start of the study.
Blood Pressure
At the end of the study, all patients had normal BP (≤130/85 mmHg) even though 33 (87%) had been hypertensive at the start of their PD treatment. With the treatment described above, however, they achieved normal BP without the use of antihypertensive drugs since the present study was started.
Residual Urine Volume
Patients’ residual urine volume decreased slightly (p NS) during the follow-up study, although it had decreased strikingly during the first period after the start of PD.
Other Parameters
There were no changes in ultrafiltration rate, Kt/V urea, total creatinine clearance, serum albumin, or hematocrit levels during the study. Body weight increased by 1.9 kg, probably reflecting improved nutritional state.
Echocardiography (Table 2)
Echocardiographic (Echo) Data of the Study Patients (n = 38)
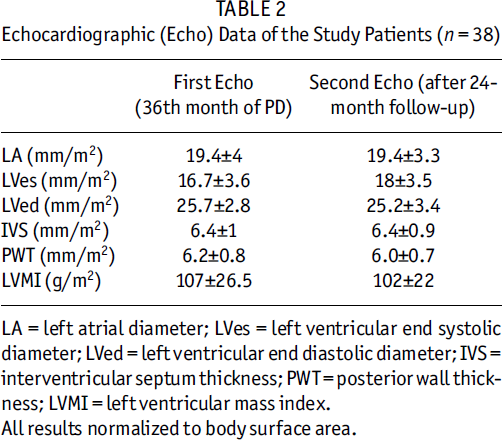
LA = left atrial diameter; LVes = left ventricular end systolic diameter; LVed = left ventricular end diastolic diameter; IVS = interventricular septum thickness; PWT = posterior wall thickness; LVMI = left ventricular mass index.
All results normalized to body surface area.
The Echo values at baseline were taken after a mean period of 36 months on PD treatment; most were within normal limits. Left ventricular mass index was 101 ± 29 g/m2 in females and 113 ± 21 g/m2 in males. Those values did not change significantly during the 24 months of follow-up. Ventricular dilatation was not present in any of the patients; LVH was detected in 8 (21%) patients. Yet, as illustrated in Figure 1, LVM index decreased at the second Echo in the 8 patients with the highest baseline LVM index: from 142 ± 14.5 g/m2 to 122 ± 6.5 g/m2 (p < 0.05).
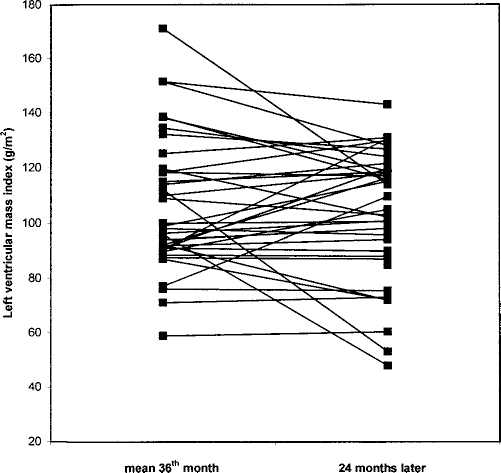
Comparison of the echocardiographic (Echo) data of long-term peritoneal dialysis (PD) patients: baseline Echo was performed by mean 36th month of PD; the second Echo was performed 24 months later.
Discussion
Our study confirms a previous report (3) that shows that excellent BP control can be achieved by strict volume control, without the use of antihypertensive drugs. The present report provides evidence that this is possible not only in short-term but also in long-term PD.
We put a strict volume strategy into practice in all dialysis patients under our care; therefore, our patient population is different from others. During the baseline Echo studies, no major abnormalities and only a few cases of LVH were recorded. The cause of the low percentage of patients with LVH is most probably due to the fact that good volume and BP control had been maintained for a considerable period before the start of this prospective study. Because of the presence of high cardiothoracic index and BP values, it is reasonable to expect that the percentage of patients with LVH would have been much higher at the beginning of PD, despite the fact that Echo data was not available at that time.
It has recently been suggested that BP control is linked to RRF and, therefore, efforts should be made to preserve renal function (4). In another study (7), decreased RRF was strongly correlated with increased mortality.
Our observation that it is possible to preserve BP control and good cardiac function without LVH over prolonged periods, despite a striking decrease in residual urine volume and renal function, is, therefore, of particular relevance. In a similar study in hemodialysis patients from our hospital (8) it was also shown that decrease in RRF did not interfere with reaching normal BP and reducing LVH.
Several authors have reported that CAPD patients are often volume expanded and have higher BPs associated with worse cardiac function (2,9,10). One author noticed that, in the beginning of CAPD treatment, BP control is often better than in hemodialysis patients (11), but that this advantage is lost with prolonged PD treatment (4). Another study (1) showed that mortality was not related to Kt/V or total creatinine clearance, but was positively related with BP level and negatively related with fluid removal. The latter finding is difficult to explain because, in a steady state, intake must equal output. A larger fluid and salt removal means a higher intake, which may be associated with, but not necessarily prove, volume expansion. In our study there was no correlation between ultrafiltration volume and volume state.
The failure to control BP with time is probably related to gradual loss of RRF, which evidently makes volume control more difficult. Years ago, Lameire (12) suggested that volume expansion helps preserve RRF. As we have shown that volume expansion makes good BP control virtually impossible, the treating physician would have the choice between accepting volume expansion and hypertension or treating it at the cost of decreased RRF. However, loss of RRF would necessitate intensifying PD. This dilemma may be one of the reasons that insidious volume expansion often goes on unnoticed.
Our results strongly support Lameire's hypothesis: hypertension, LVH, and increased mortality are caused by insufficient volume control. Loss of RRF may cause unnoticed volume expansion and may thus be blamed for the resulting hypertension and cardiac problems, which are in reality secondary and preventable consequences.