
Abstract

Optimization of Peritoneal Dialysis Program how we do that in Our Center
Objectives: Peritoneal transport kinetic study (with intraperitoneal dialysate volume marker) is a routine method of optimization of peritoneal dialysis (PD) program used in our center. Here were 41 patients examined since 1997 The usefulness of this method is presented on the example of patient with ultrafiltration (UF) failure. Methods. The patient was 45 years old; D/Pcreat=1.01 (according to PET. (1) Kinetic study of peritoneal transport of water, sodium, and urea during the 4-hour dwell (Dianeal, Baxter) with 125HHSA as an intraperitoneal dialysate volume marker. (2) Calculation of rater transport from the dilution of 125I-HSA and then calculation of velocity of sodium removal and velocity of urea transport. (3) Analysis of the course of water and sodium transport and choosing the optimal PD modality and schedule to achieve adequate water and sodium removal. (4) Analysis of the velocity of urea transport and calculation of the predicted adequacy (Kt/V urea; with computer program on the basis of Microsoft Excel} of tire proposed PD schedules. (5) Final selection of the optimal PD schedule. Results: In this patient the course of curves of water and Na peritoneal transport are similar. The curves rise up to 60th minute of dwell then reach the plateau and from 120th minute of dwell they start to fall. In this patient the time of dwell which allows for optimal UF and Na removal is no longer than 2 hours. After this time the intraperitoneal dialyzable volume starts to decrease and Na is lack-absorbed. Selected optima PD modality and schedule in this patient: CCPD (4x100’ mighty dwells+daily dwell) or CAPD (3x2.0h 1.36% glucose+1x4.0h 3.86% glucose+nightly dwell). Predicted Kt/V of proposed PD schedules respectively: 1.93+Kt/V of daily dwell and 1.94+Kt/V of nightly dwell. Conclusion: Extended assessment of peritoneal transport (with intraperitoneal dialysate volume market) allows the prediction of the optimal PD schedule (according to UF and solute transport) for individual patient. This kind of kinetic study increases the capabilities of individualization of PD program and therefore might be proposed as an important element of integrated dialysis care.
Baczynski D.1, Antosiewicz S.1, Debowska M.2, Waniewski J.2, Wantowicz Z.1, Military Institute of Medicine.1 Polish Academy of Sciences,2 Warsaw, Poland.
Dialytic Phosphate Removal: A Hew Measure of Peritoneal Dialysis Adequacy in APD Patients?
Objective: Although hyperphosphatemia is one of the few established risk factors for cardiovascular mortality in dialyzed patients, the relationship between peritoneal dialysis (PD) prescription and dialytic phosphate removal is largely unexplored. Methods: We analyzed 56, 24-hr clearance and PET studies performed in 35 children aged 0.1-17 yrs on automated PD (APD) with 3-13 nighttime exchanges, 998±110 mL/m2 fill volume and 6.07±1.96 L/m2/day total dialysate turnover. 28 children had a daytime-dwell, and 7 were anuric. Results: Mean total weekly Kt/V urea was 3.02±1.03. Dialytic phosphate clearance averaged 3.9±1.6 (range 1.8-9.4), urine phosphate clearance 2.4±2.5 (0-10) mL/min/1.73 m2. Serum phosphate ranged from 0.92 to 2.66 mmol/L The comparison of subjects with phosphate levels above (n=25) and below the upper normal limit for age (n=31) revealed significantly lower dialytic phosphate clearances in the hyperphosphatemic compared to the normophosphatemic patients (3.3±1.2 vs 4.3±1.8, p<0.05), whereas urinary phosphate removal did not differ and daily phosphate binder intake was even higher in the hyperphosphatemic patients. Dialytic phosphate clearance was correlated with 2-hr and 4-hr D/P phosphate (both r=0.52, p<.0001), but not D/P creatinine or D/D0 glucose measured in the PET. The 24-hr dialytic phosphate clearance was correlated with total dialysate turnover (r=0.64, p<0.0001) and the number of exchanges (r=0.59, p<0.001), but not with the fill volume per dwell. A significantly higher dialytic phosphate clearance was associated with >6 nighttime exchanges and a total dialysate turnover of >6 L/m2/day. Conclusions: Dialytic phosphate clearance is an important determinant of serum phosphate control. It can be predicted from the equilibration rate of phosphate but not of creatinine or glucose in the PET, and is a function of the prescribed number of PD cycles and total dialysate turnover. We postulate that in patients on APD, dialytic phosphate removal may be a more relevant marker of PD adequacy than creatinine or urea clearances.
Borzych D.2, Nau B.1, Schmitt C.P.2, Zurowska A.1, Schaefer F.1, Dept of Pediatrics,1 University of Heidelberg, Heidelberg, Germany; Department of Pediatric Nephrology,2 Medical University of Gdansk, Gdansk, Poland.
Combination of Peritoneal Dialysis (PD) and Hemodialysis (HD) Improves Solute Clearance and Quality of Life for Underdialyzed PD Patients
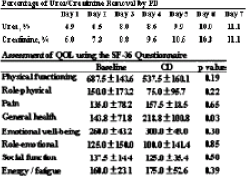
Tansfer to HD because of inadequate dialysis with PD remains a common problem. In an attempt to achieve adequate solute removal and to minimize psychological impact in the transitional period we performed combined PC and HD (CD) in 4 under-dialyzed anuric PD patients (pts; 2 M and 2 F, mean age 58±13, mean duration on PD 3.6±1.4 years). CD consists of a weekly 4- to 5-hour HD session and 2 to 3, 2-L CAPD exchanges per day. For the pts dialyzed with 2 CAPD ex-changes per day, icodextrin-based PD solution was used for the long day dwell to maintain the ultrafiltration. Dialysis dose and quality of life (QOL) were assessed before and 3 months after CD. Weekly Kt/V and creatinine clearance (CrCl) were estimated from recovery of urea and creatinine (creat) in the PD and HD spent dialyzable with time-averaged concentration of urea and creat calculated from pre-, 30-min-post-, and next pre-HD blood samples, QOL was evaluated using the SF-36 questionnaire. In all cases, CD therapy was well tolerated and a reduction in uremic symptomatology was noted. Our data show that mean weekly Kt/V and CrCl were increased from 1.79±0.28 to 2.65±0.61 (p=0.01), and from 52.9±7.9 to 71.3±9.5 L/wk/1.73 m2 (p=0.02), respectively, 37.7%±9.1% of the total urea removal and 32.7%±10.1% of total creat removal were by HD. With reference to day of HD (day 1), % of daily solute removal by PD are presented in the Table. The result of QOL using the SF-36 questionnaire is also shown. Our findings suggest that adequate solute removal can be achieved by CD. Moreover, a significant improvement in general health domain of the SF-36 was observed. In view of the re alive small PD solute removal, a PD-free day on day of HD can be considered. In conclusion, our data suggest that combined PD and HD can be an effective treatment for underdialyzed PD pts.
Cheng Y.L., Yung J.C.U., Chau S.K., Tsui Y.T., Tsang K.Y., Chan W.K., Wong F.S.Y., Yu A.W.Y., Department of Medicine, Alice Ho, Miu Ling, Nethersole Hospital, Hong Kong, China.
Retrospective Study of a Single Center's Dialysis Adequacy Data and Its Association with Mortality
Objectives: To review the adequacy data of a single dialysis center and its association with death.
Methods: Data from all chronic peritoneal dialysis (PD) patients were retrieved from the PD Adequest® 2.0 program. Averaged values were calculated for each patient. Patients who changed to hemodialysis or transplanted were excluded.
Results: From June 2001 to December 2005. 480 patients were eligible. M:F=250:230; mean age 60.5±12.6 years; mean Kt/V 2±0.65, median 1.9; mean creatinine clearance (CrCI) 63.86±25.02 L/wk/1.73 m2, median 56.8 L/wk/1.73 m2; mean glomerular filtration rate (GFR) 1.83± 2.49 mL/min, median 0.53 mL/min; serum albumin 32.93±1.9 g/L, median 33 g/L; body surface area (BSA) averaged 1.6±0.19 m2. Daily ultrafiltration (UF) ranged from -750 to 3200 mL, mean UF was 970.49±605.52 mL PET status was available in 236 patients: H 26.7%, HA 44.9%, LA 8.1%, and L 20.3%. Davies scores were distributed as follows: no comorbidity 134 (27.9%), intermediate 257 (53.5%), and severe 89 (18.5%), 154 patients died (32.1%). On univariate and multivariate analyses, only age (p<0.001) and Davies score (p<0.001) were significantly associated with death, Sex, PET, CrCI, KW, GFR, albumin, BSA, and UF were not associated with death.
Conclusions: In this retrospective study of Chinese chronic PD patients, age and Davies score were significant associations with death. Dialysis adequacy was not predictor of death.
Chu K.H., Tang H.L., Cheuk A., Lee W., Yim K.F., Fung K.S., Chan H.W.H., Tong K.L., Princess Margaret Hospital, Hong Kong, China.
Restricting Dietary Fluid and Salt Intake Does Not Hasten the Decline in Residual Renal Function (RRF) in Peritoneal Dialysis (PD) Patients
Background: Restriction on fluid and salt intake facilitates maintaining good volume status in PD patients (pts). However, the impact of this approach on RRF remains unclear. In this study, we explored the impact of restriction in fluid and salt intake on RRF in pts receiving PD. Subjects and Methods: We analyzed the decline rates of glomerular filtration rate (GFR) prospectively in incident PD pts with initial GFR >2 mL/min/1.73 m2. All pts were asked to restrict dietary salt and fluid intake throughout the whole study period with intensive pt education an d rigorous inspection. GFR was measured as the mean of urea and creatinine clearance. The measurements were repeated 6,12,18, and 24 months after the initiation of dialysis. Results: A total of 59 incident PD pts (34 M, 25 F; mean age 61.4±12.6 years) were enrolled in this study. The cause of renal failure was DM in 22 cases. By the end of the 2-year follow-up, 5 pts (8.5%) became anuric; 26 pts had GFR declining more than 50% of initial value. Median decline rate of GFR was 0.12 mL/min/1.73 m2/month. Median decline rate of daily urine volume was 22 mL/month. DM pts had faster decline in GFR than that of non-DM pts. Conclusions: Our study suggests that limiting dietary fluid and salt intake did not accelerate decline of RRF compared to data reported from the Western world although diabetic pts had faster decline rate of RRF than that of non-DM pts in our PD pts.
Gan H.B.1, Tian X.K.1, Wang T.2, Wang T.1, Division of Nephrology,1 Peking University First Hospital; Division of Nephrology,2 Peking University Third Hospital, Beijing, China.
Glucose Degradation Products in Peritoneal Dialysis Fluids Predict Decline of Residual Renal Function
Residual renal function (RRF) strongly affects mortality, morbidity, blood pressure, and fluid control in peritoneal dialysis (PD) patients. Consider-able amounts of toxic glucose degradation products (GDPs; reactive carbonyl compounds) are formed during heat sterilization of conventional PD fluids. It was recently shown that (1) during dwell GDPs are transported from the peritoneal cavity into the circulation, (2) they may exert negative effects through direct tissue damage or via formation of advanced glycation end products, and (3) the most bioreactive GDP, 3.4-dideoxyglucosone-3-ene (3,4-DGE), promotes renal cell apoptosis. The aim of this prospective, controlled, parallel, multicenter study was to investigate the effect of GDPs on RRF in PD patients, randomly assigned to 18 months treatment with Gambrosol®trio(3.4-DGE<1 mol/L) or conventional fluids (3,4-DGE 13-20 μmol/L). RRF was measured every 4-6 weeks as the mean of renal urea and creatinine clearance. For various reasons not related to the study, data from 69 of 80 randomized patients were eligible. 43 patients on Gambrosol® trio and 26 on conventional fluids contributed data on RRF according to their time in the study. Groups were not statistically different in angiotensin receptor blocker (ARB) medication (16% vs 31%), start RRF (6.7±3.1 vs 6.2±2.4 mL/min/1.73 m2), age (52±12 vs 54±15 years), diabetes (20.9% vs 19.2%), gender (26 vs 14 males), and time on PD(9±13 vs 5±10 months), but in ACE inhibition medication (70% vs 42%).The repeated measures model (heterogeneous compound symmetry) adjusted for age, diabetes, gender ARBs, ACE inhibitors, time on therapy, and potential interactions, provides significant evidence that monthly RRF decline was lower with Gambroso® trio compared to conventional fluids (1.5% vs 4.3% p=0.0437).The present prospective clinical study shows that PD fluid with minimized GDP level has a protective effect on RRF in PD patients.
Haag-Weber M.1, Haag U., Nabut J.2, Wieslander A.2, Deppisch R.,2 for the DIUREST Study Group., Klinikum St. Elisabeth,1 Straubing; Gambro Corporate Research,2 Hechingen, Germany.
Evaluation of Equations for Predicting Residual Renal Function in Patients on Peritoneal Dialysis
Objectives: Retention of residual renal function (RRF) is one of the benefits of peritoneal dialysis (PD) compared with hemodialysis, and plays an important role in achievement of optimal dialysis efficacy and prevention of dialysis complications in PD patients. A method of convenient and accurate estimation of RRF as a substitute for measured creatinine clearance (Ccr) is needed. Recently, the general condition of patients on dialysis is managed in treatment of the final stage of chronic renal disease. In the guidelines of the Kidney Disease Outcomes Quality Initiative [K/DOQI) the formulas developed from the Modification of Diet in Renal Disease Study (MDRD) are recommenced for estimating Ccr. The objective of the present study is to compare the evils of measured Ccr and those of Ccr estimated by the Cockcroft-Gault or MDRD formula in PD patients.
Methods: The correlation between measured Ccr derived from 24-hour urinary collection and predicted Ccr calculated using the Cockcroft-Gault and MDRD equations was evaluated in 61 patients on PD (49 males and 12 females).
Results: The equation of linear regression was as y=-0.237±0.446x (F0.456,p<0.0001) based on the Cockcroft-Gault formula, and y=1.51+0.226x (I=0.263,p<0.01) by the MDRD formula (y. measured Ccr. x. estimated Ccr). The measured Ccr or estimated Ccr based on the Cockcroft-Gault formula and duration of PF showed a significant correlation but no correlation was found for Ccr estimated by the MDRD formula, Ccr estimated by the Cockcroft-Gault formula significantly correlated with 24-hour urinary volume.
Conclusion: It appears that estimated Ccr, especially that estimated by the Cockcroft-Gault formula, is useful for estimating RRF in patients on PD.
Hamada C., Hayashi K., Inuma J., Sekiguchi Y., Shimaoka T., Inaba M., Koyanagi I., Horikoshi S., Tomino Y., Juntendo University, Tokyo, Japan.
Plasma Cystatin C Reflects Residual Glomerular Filtration Rate in Dialysis Patients
Background: Residual renal function influences morbidity, mortality, and quality of life of chronic dialysis patients. Residual glomerular filtration rate (rGFR) is therefore an important parameter in the follow-up of these patients. Because rGFR is measured as the mean of creatinine and urea clearance, a complete 24-hour urine collection is essential, but often very difficult to manage for these patients.
Methods: We investigated if plasma cystatin C (cysC) could give a good estimate of rGFR in dialysis patients and compared it to the measured rGFR, and to the Modification of Diet in Renal Disease (MDRD) estimate of rGFR. A total of 465 patients were in included, cysC levels of 215 hemodialysis (HD) and 95 peritoneal dialysis (PD) patients were used to derive a formula for rGFR. This formula was tested in the validation group of 107 HD and 48 PD patients.
Results: The cysC formula rGFR=-0.70+22* (1/cysC) was derived in the modeling group. The mean estimated rGFR obtained with this formula in the validation group was not significantly different from the mean measured rGFR: difference 0.19 mL/min/1.73 m2,95% confidence interval (CI) -2.37 to 2.75 mL/min/1.73 m2. The MDRD formula gave a larger difference from the mean measured rGFR (3.13 mL/min/1.73 m2) and a much wider 95% CI (-1.29 to 7.55 mL/min/1.73 m2). With the cysC formula 42.6% of the estimates were within 30% of the measured rGFR and 65.8% were with in 50%. With the MDRD formula only 14.2% were within 30% and 23.9% within 50% of the measured rGFR. A separate model for HD and PD patients did not improve the estimation of rGFR.
Conclusions: The cysC formula showed better accuracy and precision than the MDRD formula. Therefore the cysC formula and not the MDRD formula should be used to calculate rGFR in dialysis patients when no 24-hour urine sample is available.
Hoek F.J.1, Korevaar J.C.2, Dekker F.W.3, Boeschoten E.W.4, Krediet R.T.5, Depts of Clin Chem1 & Clin Epidemiol & Biostats,2 Academic Med Cntr, Amsterdam (AMC), Dept of Clin Epidemiol,3 Leiden Univ med Center, Leiden: Hans Mak Inst.4 Naarden: Dept of Nephrol,5AMC. The Netherlands.
Cardiovascular Advantage in Peritoneal Dialysis (PD) Patients Compared with Hemodialysis (HD) Patients
Purpose: Left ventricular hypertrophy (LVH) is the most important predictor of mortality in dialysis patients (pts). The purposes of the present study were to analyze the cardiovascular advantage in PD pts associated with residual glomerular filtration rate (rGFR), and to compare it with that in HD pts. Patients and Methods. The relationship between LV mass index (LVMI) using echocardiography and rGFR was analyzed in 27 PD and 24 HD nendiabetic pts in Juntendo Univ Hosp. Measurement of these 2 parameters was performed at 0, 6, 12, 24, and 36 month after the start of dialysis. Results: Although LVMI in PD pts was. 151.1±50.1 g/m2 at the start of dialysis, it was significantly decreased to 118.6.±31.9 g/m2 after 6 months of dialysis (p<0.01),121.4±24.8 g/m2 after 12 months (p<0.01), and 113.2±30.7 g/m2 after 24 months (p<0.01).The rGFR in PD pts was 3.4+2.6 mL/min at the start of dialysis and was not significantly decreased after 36 months. On the other hand, LVMI in HD pts was 154.8±39.1 g/m2 at the start of dialysis and was not deceased after 6, 12, 24, and 36 months. The rGFR in HD pts was 3.7±2.2 mL/min at the start of dialysis, but was significantly decreased to 1.4±1.2 mL/min after 6 months (p<0.01). The urinary protein eve at the start of dialysis was 6.1±3.5 g/g Cr in PD pts who showed anuria and was 2.8±2.1 g/g Cr (p<.0.01) in PD pts who did not show anuria after 36 months. There was a significant correlation between- the level of rGFR and that urinary protein excretion in PD pts. Conclusion: It appears that PD may improve LVH, since rGFR was maintained in PD pts compared with HD pts.

Io H., Ro Y., Inaba M., Koyanagi I., Sekiguchi Y., Simaoka T., Inuma J., Hayashi K., Hamada C., Horikoshi S., Tomino Y., Division of Nephrol, Dept of Internal Medicine, Juntendo University School of Medicine, Tokyo, Japan
Clinical Benefits of a Low Glucose Degradation Products Solution in Patients Starting Peritoneal Dialysis: Preliminary Report
Objectives: In vitro studies of peritoneal dialysis (PD) solutions demonstrated that a lactate-buffered fluid with their pH-neutral and low glucose degradation products (LF) has better biocompatibility than a conventional acidic lacteal-buffered fluid (CF). However, few clinical trials showed the benefits of the former on clinical parameters. We performed a prospective, randomized study with patents staging PD, to compare LF with CF. Methods: 47 patients who commenced PD in 4 major centers in Korea were randomized to either 6 months of treatment with LF (n=18) or CF (n=29). 4 patients on LF and 6 patients on CF discontinued treatment [death (1 vs 2), switch to hemodialysis (1 vs 2), transfer to another hospital (2 vs 2), respectively]. Peritoneal function tests and adequacy measurements were undertaken at each study center on 2 occasions during the study: after 4-week run-in period and after 6 months of treatment with each fluid. Results: No differences between the 2 groups in the patient survival and technique survival role were observed. In patients using LF there were no significant changes in renal creatinine clearance, urine volume, and peritoneal ultrafiltration over the treatment period. Conversely, in patients on CF renal creatinine clearance and urine volume were significantly decreased, out peritoneal ultrafiltration was significantly increased over the 6-month treatment period: 29.3 (17.8-52.7) vs 12.6 (2.06-39.5) L/1.73 m2/ week, 600 (325-800) vs 420 (90-300) mL/day, and 950 (125-1280) vs 1250 (950-2000) mL/day, respectively Total fluid removal [combined urine and ultrafiltration) was not changed in patients on each fluid. In LF-treated patients, body weight was significantly increased over the treatment period: 63.0 (49.9-70.0) vs 65.0 (53.2-73.0) kg. No differences within groups and between groups were observe for dialysate/plasma creatinine ratio and Kt/V urea. Conclusions: Over the 6-month treatment period, LF better preserved residual renal function and urine volume than CF. No differences in peritoneal solute Iran sport rate were observed between LF and CF.
Kim S.1, Kim S.G.2, Ch J.E.2, Chung W.3, Oh K.H.1, Kim Y.S.1, Ahn C.1, Han J.S.1, Dept of Intern Med.1 Seoul National Univ. College of Med. Seoul; Dept of Intern Med & Kidney Res. Inst of Hallym Univ.2 Anyang; Dept of Intern Med,3 Gachon Univ, Incheon, South Korea.
Clinical Outcome in Long-Term Peritoneal Dialysis Patients: A Chinese Single Center Experience
Objectives: To analyze the clinical outcome in long-term peritoneal dialysis (PD) patients in China.
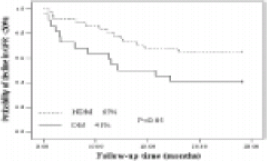
Methods: 58 PD patients who survived on PD more than 3 years were observed. According to their different clinical outcome, the patients were divided into 4 groups: continued PD group (C), transplant group (T), hemodialysis group (H), and death group (D). The recently nutritional index and the recently dialysis adequacy index, fluid removal, and residual renal function were evaluated. The recently index is defined as the recently index within half year of the observed time or the observed events occurred.
Results: The recently total Kt/V in D group was significantly lower than that compared with other 3 groups: D 1.50±0.26 vs C 1.88±0.41. T 2.01±0.43, H 1.83±0.47, respectively; p=0.05,p=0.01,p=0.06 respectively. The recently total Kt/V and total CCr in death group was significantly lower compared with that values of 1 year before death: p=0.05 and p=0.01 respectively. In comparison with D group and H group, the residual renal Kt/V or residual renal CCr in C group was significantly higher: p=0.05. Multivariate Cox regression analysis show that the total Kt/V was an independent predictor of survival (p=0.007), whereas albumin had not significance in predicting these long-term PD patients survival.
Conclusions: Dialysis inadequacy is the important cause of death for long-term PD patients, residual renal function makes an impact on outcome of long-term PD patients, albumin may weaken its predictor of survival in patients more than 3 years PD duration.
Lin X., Qian J., Lin A., Yao Q., Renal Division, Renji Hospital, Medical College of Shanghai Jiao Tong University Shanghai, China.
A Prospective Randomized Open-Label Study of Frusemide in the Preservation of Residual Renal Function in Patients Started on CAPD
Background: Patients on CAPD are dependent on residual renal function (RRF) for solute and water clearances, and this declines with time on dialysis. Loop diuretics have been postulated to slow this decline, but the existing data on this remain controversial. We performed a prospective randomized open-label study where patients new to dialysis were given frusemide or no frusemide at the time of training and followed prospectively for 1 year. Methods: Starting from February 2004, patients newly stared on CARD with base ire glomerular filtration rate (GFR) >2 mL/min/1.73 m2 were recruited to be randomized to receive either frusemide (500 mg once daily/or no frusemide at the time of training. Patients with underlying medical conditions that mandate diuretic therapy, those with poor short-term likelihood of survival, or with planned elective renal transplantation were excluded. Diabetic and nondiabetic patients were stratified at randomization. They were followed for 1 year during which dialytic indices and residual renal function (RRF) were measured at 3-monthly intervals. Frusemide would be stopped when patients became anuric. Results: Of the 37 patients recruited to date, 32 (male:female ratio 14:18, mean age 59.4±15.7) were eligible for analysis. 17 patients received frusemide and 15 were controls. The mean rates of decline of RRF of the 2 groups, established for each patient by line are regression of all available data points, were 1.63 vs 1.76 mL/min/1.73 m2/yr (p=NS). Dividing among the diabetics (1.69 vs 1.82 mL/min/1.73 m2/yr,p=NS) and the nondiabetics (1.61 vs 1.68 mL/min/ 1.73 m2/yr,p=NS) did not yield different results. During the study period, 4 patients became anuric (urine volume <100 mL/day. 2 in each group). Conclusion: Frusemide, when used at a dose of 500 mg once daily, was not able to preserve the RRF better than controls in patients undergoing CAPD.
Mak S.K., Lo M.W., Tong G.M.W., Lo K.Y., Wong P.N., Wong A.K.M., Department of Medicine and Geriatrics, Kwong Wah Hospital. Hong Kong, China.
Impact of Residual Diuresis on Survival in Peritoneal Dialysis
Patient survival in peritoneal dialysis (PD) has been discussed in previous reports: hypoalbuminemia and diabetes (DM) are associated with decreased survival. The influences of other risk factors upon mortality remain less clear.
Objective: To evaluate impact of residual diuresis in the survival of patients in PD.
Methods: We analyzed all patients in PD program since September 1996 to July 2005. Survival curves were analyzed with the Kaplan-Meier method; comparison of survival curves were performed using log-rank test. Multivariate regression analysis was performed to determine the factors associated in the risk of death.
Results: 214 patients were evaluated. 57% males, age 56.4±19.5 years, 22.9% had DM. 24.4% coronary heart disease (CHD), and 94.7% hypertension. PD modalities were CAPD 9.4%, CCPD 32.4%, and NIPD 58.2%. Average weekly Kt/V was 2.4±0.77, serum albumin 3.6±0.4 g/dL, and RRF at admission PD program was 1075±688 mL/24 hours. The probability of survival was significantly better in groups with residual diuresis >750 mL/24 hours (95.2% vs 92.7% in 1 year 91.7% vs 75.4% in 2 years, and 83.5% vs 59.2% in 3 years p=0.02). The survival rate was less in patients with DM. CHD, and hypoalbuminemia. When comparing the group with residual diuresis major and minor to 750 mL/24 hours there was no difference in age, percentage of DM, hypoalbuminemia, and Kt/V. In the multivariate analysis, RRF <750 mL/24 hours was an in dependent mortality risk factor; (DR=3.04, Cl 95% 1.23-7.53. p<0.016), hypoalbuminemia (OR=6.39. Cl 95% 2.69-5.20,p<0.001), and CHD (OR=2.72, CI 96% 1.08-6.90,p<0.034). Main mortality causes were cardiovascular 41.2%, infections unrelated to the technique 25.5%, stroke 5.9%, and peritonitis 3.9%.
Conclusions: The survival rate in the PD population is better in the group with clinically significant residual diuresis. Diabetes, CHD, and hypoalbuminemia are associated with an increased risk of death.
Ortiz A.M., Machuca E., Aravena C., Canto K., Pontificia Universidad Catolica De Chile, Santiago, Chile.
Peritoneal Equilibration Test (PET]: Correlation between Peritoneal Membrane Status and Peritoneal Dialysis Parameters
Objectives: To evaluate the effects of peritoneal membrane status on clinical and biological markers, patient (pt) and peritoneal dialysis (PD) technique survival. Patients: 79 PD pts (36 M, 43 F; mean±SD age 37.5±13.9 years) on PD during an average of 641.2±705.4 days, 66 (83.5%) are dialyzed by automated PD and 13 (16.5%) by CAPD. 61 pts are (83.5%) hypertensives (HT), 19 have hydric overloading (16.5%), and 11 are diabetics (13.9%). Results: The peritoneal membrane status is: L in 6 pts (7.6%); LA in 27 pts (34.17%); HA in 26 pts (32.91%), and H in 13 pts (24.05%). The adequacy parameters of our patients are: Kt/V≥2 (64.6%), total weekly creatinine clearance (WCC)>60 L/1.73 m2 (51.9%), n PCR>0.9 (69%), and albumin >30 g/L (74.7%). We found no statistical correlation between peritoneal membrane status and clinical parameters (age, ultrafiltration, hydric overloading. HT, mode of PD), except for the following parameters:
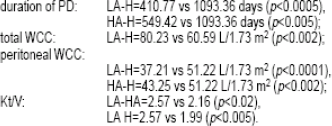
No statistical correlation was found between peritoneal membrane status and patient or technique survivals at 6 and 12 months. Conclusion: The PET is important for PD patients because it helps to evaluate peritoneal membrane status. The adequacy parameters of our patients are similar to the DOQI guidelines. Our study shows significant correlation only between membrane status, duration of PD, total WCC, peritoneal WCC, and Kt/V.
Ounissi M.1, Ben Hamida F.1, Cherif M.1, Ben Abdallah I.1, Helal I.1, Abderrahim E.1, Cherif N.2, Ben Abdallah T.1, Lakhoua R.2, Kheder A.1, Dept of Nephrol,1 Charles. Nicolle Hosp; Dept of Pediatric Dis,2 Charles Nicolle Hosp, Tunis, Tunisia.
Effect of Adequacy of Dialysis on Survival in CAPD Patients in India
The optimum level of adequacy of dialysis for CARD patients has not been studied in India. Thereto re we undertook this study to determine the impart of adequacy of dialysis on survival of CARD patients. 108 patients of CAPD (age 49.8±15 years, male 74) were included in this study. The mean total Kt/V (peritoneal+renal) and total creatinine clearance (CrCI) were calculated by PD Adequest® software. The primary end point of the study was the death of the patient. On Kaplan-Meier survival analysis, the median survival was higher in patients with Kt/V>1.7 (75 months) compared to patients with Kt/V≤1.7 (55 months) but not statistically significant (log rank 0.22, p=0.65). The 12, 24, and, 36 months cumulative survival in patients with Kt/V>1.7 was 100%, 91.3%, and 76% respectively, and in patients with Kt/V≤1.7 it was 97.2%, 85.7%, and 75.9%, respectively. On analyzing the survival based on weekly total CrCI, median survival was 55 months with CrCI≤50 L/week compared to 75 months with CrCl>50 L/ week but not statistically significant (log rank 2.6. p=0.10). The 12.24, and 36 months cumulative survival was lower in patients with CrCI<50 L/week (95%, 76%, and 61%, respectively) compared to patients with CrCI>50 L/ week (100%, 92.6%, and 76.8%, respectively). Median survival was 56 months with urine output>200 mL/day while it was 40 months in patients with urine output of ≤200 mL/day (log rank 7.6, p=0.0050). On Cox regression analysis, while weekly CrCI (odds ratio 2.9.95% CI 0.96-9.2, p=0.05) and urine output (odds ratio 3.36.95% Cl 1.4-7.9, p=0.006) have significant impact on survival of patients, but Kt/V has no significant impact on survival (odds ratio 0.59, 95% CI 0.96-1.78, p=0.35).
We conclude that the optimum level of adequacy of dialysis in peritoneal dialysis is total Kt/V >1.7 and total CrCI >50 L/week. The residual urine of greater than 203 mL has a significant impact on survival of CAPD patients.
Prasad N., Gupta A., Sinha A., Sharma R.K., Gulati S., Kumar A., Kumar R., Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India, Lucknow, India.
The Adequacy of Peritoneal Dialysis in a Single Chinese Center
Objective: To assess the adequacy of peritoneal dialysis (PD) in Chinese patients and its correlated factors.
Methods: A total of 120 patients on continuous ambulatory PD (CAPD) for more than 6 months in Shanghai Rui Jin Hospital between July 2001 and June 2005 were enrolled into this study. The adequacy of PD was quantified by Kt/V and creatinine clearance (CrCI) and calculated by PD Adequest® 2.0 for Windows® software in 62 patients. The biochemical parameters including serum albumin, calcium, phosphate, iPTH, CRP, and Hct were correlated with Kt/V. They were assigned to 2 groups according to weekly Kt/V: group A, Kt/V>2.0, and group B, Kt/V<2.0. Morbidity and mortality were compared with the 2 groups.
Results: All 62 CAPD patients were followed up for 1.60±1.12 years There were 30 men and 32 women, and their mean age was 70.53±11.03 years. Mean Kt/V was 2.35±0.85 and CrCI was 77.29±46.75. Peritoneal equilibration test (PET) showed 23% were high turnover. 26% were high-average. 31% were low-average, and 18% were low turnover. There were positive correlations between Kt/V and Hct, Alb, CO2CP. There were negative correlations between Kt/V and Ca, P, iPTH, CRP. For the 2 groups, the incidence of secondary hyperparathyroidism was significantly different (32% vs 52%. p<0.05) but there was no significant difference with other parameters such as Hct Alb. Ca, P, CO2CP, and mortality.
Conclusions: The study showed the adequacy of PD was increased by correcting anemia, malnutrition, and metabolic acidosis. Calcium phosphate disturbance and inflammation contributed to low Kt/V.
Qian Y., Xu Y.-W., Wu P., Xie J.-Y., Zhu P., Wang J., Chen N., Renal Division, Rui Jin Hospital Affiliated to Jiao Tong University, Shanghai, China.
A Novel Approach to Peritoneal Dialysis Adequacy: Two-year Follow-Up
Background: Loss of residual renal function (RRF) was found to be associated with decreased dietary protein intake (DPI) and increased patient dropout in peritoneal dialysis (PD) patients. In the present study, we investigated a novel approach to PD adequacy and its impact on patient outcome.
Methods: A prospective, longitudinal cohort study was performed in incident PD patients that started PD between January and December 2003 and the patients were followed until December 2005. Patients’ target DPI was set at 0.8-1.0 g/kg/day and total fluid removal was set at 1 L/day (by restricting dietary salt and fluid intake) throughout the whole study period, which was achieved by intensive patient education and individualized PD prescription to maintain nitrogen balance.
Results: A total of 81 incident PD patients (male 43 and female 38) were enrolled in this study. Mean age was 59.6±13.6 years. By the end of 2-year follow-up. 49 patients were still on PD, 16 died. 3 transferred to hemodialysis, and 13 transplanted. Cardiovascular event was the primary cause of death, accounting for 37.5% (6 cases) followed by advanced cancer, 25% (4). During the follow-up period, mean DPI remained within the optimal range recommended by this study (p=0.210). Total Kt/V urea and daily total fluid removal remained unchanged (p=0.124, p=0.892) despite a significant decline in RRF.2-year patient survival and technique survival were 77% and 95%, respectively.
Conclusions: Our study suggested that the approach to limit but maintain patients’ dietary protein, salt, and fluid intake may facilitate adequate dialysis and contribute to good clinical outcome in our PD patients.
Tian X.K.1, Zhe X.W.2, Chen W.2, Wang T.1, Wang T.2, Division of Nephrology,1 First Hospital, Peking University; Division of Nephrology,2 Third Hospital, Peking University, Beijing, China.
Dialysis Adequacy in Anuric Chinese Peritoneal Dialysis Patients
Background: Although weekly Kt/V of 2.0 and daily dietary protein intake (DPI] of 1.2-1.3 g/kg/day were commonly recommended for peritoneal dialysis (PD) patients, our previous study suggested that a lower protein diet did not lead to malnutrition in PD patients. In this study, we explored how limiting DPI would affect dialysis adequacy in anuric PD patents.
Methods: A cross-sectional study including only anuric PD patients from the PD center of Peking University was performed. Patients’ demographic feature was collected. Urea kinetic model was used to assess solute clearance. Patients’ nutritional status was assessed by DPI, biochemistry handgrip strength (HGS), and Subjective Global Assessment (SGA). Volume status was measured by bioelectrical impedance analysis (BIA).
Results: A total of 70 anuric PD patients were included in this study Mean age was 64.3±12.4 years and time on PD was 36.7±30.7 months The prescribed dialysis dose, Kt/V DPI, serum albumin, Karnofsky Index were 7528±1368 mL, 1.72±0.35, 0.84±0.28 g/kg/day, 36.1±4.9 g/L, and 71.9±17.1, respectively. The prevalence of malnutrition was 24.3%. Systolic blood pressure and diastolic blood pressure were 125±23 mmHg and 75.5±14.7 mmHg, respectively.
Conclusions: Our study suggested that anuric PD patients could achieve adequate dialysis even under lower solute clearance. Limiting DP contributed largely to the adequate dialysis in our anuric PD patients.
Tian X.K.1, Chen W.3, Zhe X.W.2, Wang T.1, Wang T.2, Division of Nephrology,1 First Hospital, Peking University; Division of Nephrology,2 Third Hospital, Peking University, Beijing, China.
A Combination Therapy of Peritoneal Dialysis and Hemodialysis without Ultrafiltration from the Initiation of Renal Replacement Therapy
Objectives: Peritoneal dialysis and hemodialysis combination therapy (PD+HD) is an alternative method to supplement the weak points of PD. This therapy has been considered to decline the loads of PD concerning ultrafiltration (UF) volume and solute removal, and is usually applied in PD patients (pts) with UF failure. We performed PD+HD from the initiation period of PD in uremic pts that still preserve residual renal function (RRF) whose daily urine volume was >700 mL. Methods: 4 pts continuously received this combination therapy more than 1 year (1 male and 3 female, 1 DM and 3 chronic glomerulonephritis pts, average age 56 years, average therapy period 20 months). This therapeutic protocol consists of 5 days of PD (1.5%, 1.5 L glucose dialysate x4 bags) plus 1 HD session (3 hours) without UF per week. Weekly creatinine clearance (Ccr) rates in RRF, PD, and HD, D/P ratio estimated by PET were measured in every 6 months. Results: Urinary and UF volumes of PD were maintained in every case, and the UF in HD session was not necessary because the body weights of pts were not changed. A typical pt, who is a 54-year-old female diabetic pt received this therapy for 37 months, showed weekly Ccr of RRF, PD, and HD after the 37 months therapeutic period were 76, 31, and 11, respectively, and Ccr of RRF never declined. D/P ratios at the start and last points were 0.48 and 0.59, respectively. Ccr of RRF and PD in other cases maintained with stability as ‘well as the described case, and D/P ratios were not changed significantly. Conclusion: To initiate this combination therapy from the start of renal replacement therapy caused several beneficial effects. First. PD and HD session without LF may maintain RRF in a long-term. Next, 1 HD session per week bring 2 days peritoneal resting, leading to the maintenance of a long-term peritoneal function. Moreover, pts would have a good opportunity to re-educate fundamental PD procedures, diet, and daily life once a week, which may connect to the early detection of complications. Thus, to initiate this combination from the start of PD should he considered as a useful method.
Ueda A.1,2, Arano Y.1, Inoue M.1,2, Hirayama A.2, Yoh K.2, Yamagata K.2, Nagase S.2, Kidney and Dialysis Center,1 Namegata District Gen Hosp; Dept of Intern Med,2 Institute of Clin Med, Univ of Tsukuba, Ibaraki, Japan.
Adequacy of Automated Peritoneal Dialysis (APD) with and without Manual Daytime Exchange: A Randomized Controlled Trial
Objective: APD is usually performed using a low dialysate flow. Until now it remains unclear whether the addition of manual daytime exchanges or the increase of nightly dialysate flow is the best strategy for optimizing treatment in case of inadequate clearances. Methods: In this open label, randomized controlled crossover trial 18 patients with high-average (HA) or low-average (LA) peritoneal transport rates sequentially underwent 2 different continuous cyclic peritoneal dialysis (CCPD) regimens for 7 days each with an intermittent washout period of 7 days. “Manual exchange’ treatment was a CCPD with low nightly dialysate flow and 1 manual daytime exchange (1 daytime dwell with icodextrin, another daytime dwell with glucose). “High flow” treatment was defined by CCPD with high dialysate flow but without manual daytime exchange (only 1 daytime dwell with icodextrin). Results: Creatinine clearances were significantly increased during “high flow’ treatment compared to “manual exchange” treatment (8.56±1.22 vs 7.87±1.04 L/treatment respectively, p=0.011). Similarly, urea nitrogen clearances were significantly enhanced during “high flow” treatment (12.83±1.98 vs 11.68±1.06 L/treatment, p=0.014). Glucose absorption was higher with the “high flow’ regimen compared to the ‘manual exchange” treatment. Phosphate clearances, β2-microglobulin clearances, ultrafiltration efficacy, and peritoneal protein loss did not differ between the 2 treatment modalities. Subgroup analysis dependent on peritoneal transport types showed that this effect on clearances was most marked in HA transporters but smaller and not significant in LA transporters. Conclusion: Small solute clearances can be significantly improved and β2-microglobulin clearances maintained in CCPD patients by increasing the nightly dialysate flow instead of adding a manual daytime exchange. The clinical impact of increased clearances as well as lifestyle advantages (by sparing manual exchanges} have to be weighed against increased costs of “high flow” treatment when a change in APD prescription is required
Vychytil A.1, Demetrakis D.1, Habicht A.1, Schillinger M.2, Hoerl W.H.1, Division of Nephrology and Dialysis1 and Division of Angiology,2 Medical University Vienna, Vienna, Austria.
CAPD Patients Are Essentially Overhydrated State: Evidence from before and after Kidney Transplantation
Objectives: It seems that many continuous ambulatory peritoneal dialysis (CAPD) patients are overhydrated status, however, the patients with residual renal function (RRF) considered to be maintained as euhydration status. Kidney transplantation might be the most ideal treatment to correct hydrate status in patients with end-stage renal disease. In order to clarify whether hydration slate is maintained appropriately try CAPD, we evaluated it before and after kidney transplantation.
Methods: Living kidney transplantation was performed in 10 CAPD patients with RRF (urine volume>300 mL/day) and 15 anuric hemodialysis (HD) patients. Changes in body weight (BW), systolic blood pressure (SABP), cardiothoracic ratio (CTR), and human atrial natriuretic peptide (hANP) were analyzed before and i month after kidney transplantation for evaluating hydration status.
Results: Before kidney transplantation, there was no significant difference in BW, SABP, CTR, and hANP between CAPD and HD. After kidney transplantation, serum creatinine levels markedly decreased to 1.1 mg/dL in CAPD patients and 1.2 mg/dL in HD patients, respectively. In CAPD patients, all of those parameters significantly decreased. Average % change was -9.1% in BW, -7% in SABP -6% in CTR (45% to 41%), -65.5% in hANP (74.7 to 25.6 pg/mL), respectively. On the other hand, although SABP decreased by 10%, CTR (45% to 45%) and hANP (50.6 to 48.7 pg/mL) did not change after transplantation in FD patients. In addition, BW decreased in only 40% of the patients.
Conclusions: Our data suggest that even CAPD patients with RRF, who might be in appropriate hydration status clinically, were more overhydrated than anuric HD patients.
Yamamoto H., Tanno Y., Kawamura Y., Mitome J., Yamamoto l., Yaginuma T., Hayakawa H., Ikeda M., Hanaoka K., Yokoyama K., Kawaguchi Y., Hosoya T., Div of Nephrol & Hypertens, Dept of Intern Med, Jikei Univ School of Med, Tokyo, Japan.
Residual Renal Function Predicts the Occurrence of Autonomic Neuropathy in Nondiabetic CAPD Patients
Objectives: To evaluate the prevalence of autonomic neuropathy in nondiabetic CAPD patients and to investigate its risk factors.
Methodology: We performed a cross-sectional study on 114 nondiabetic CAPD patients. All patients underwent a standard battery of autonomic function tests including the sympathetic skin response, blood pressure and heart rate response to orthostasis, as well as the R-R interval variation test.
Results: Patients were categorized into 2 groups according to the results of the autonomic function tests. The baseline clinical data, nutritional and dialysis adequacy indices were compared. Definite autonomic neuropathy was noted in 53% of cases. Patients with autonomic neuropathy were significantly older (60.81±12.53 vs 55.80±12.43 years, p=0.041) and both measures of residual renal function as well as dialysis dose were significantly lower in the autonomic neuropathy group. All other variables measured were not significantly different Multivariate analysis using logistic regression identified the weekly renal Kt/V as the sole predictor of the presence/absence of autonomic neuropathy. A 1-unit reduction in residual renal function is predictive of a 10-times increase in the chance of having autonomic neuropathy (odds ratio=0.100, CI=0.030-0.335, p<0.001).
Conclusion: Autonomic neuropathy is common in nondiabetic CAPD patients. Res dual renal function, as calculated by the weekly renal Kt/V remains the most powerful predictor of autonomic neuropathy, underlining the importance of preservation of residual renal function in patients on CAPD. Prospective study is warranted to investigate the reversibility of autonomic dysfunction after an increment in dialysis dose.
Yung J.C.U., Cheng Y.L., Tsui Y.T., Tsang K.Y., Wong S.K., Yu A.W.Y., Department of Medicine, Alice Ho Miu Ling Nethersole Hospital, Tai Po, Hong Kong.
Determination of Hydration State in Dialysis Patients Using Bioimpedance Analysis
Bioimpedance analysis (BIA) is a useful technique, with a noninvasive, inexpensive, and simple way, to measure body fluid volume. The aim of this study was to evaluate the use of segmental normalized resistivity (ρN), an indicator of hydration, by comparing peritoneal dialysis (PD; n=11, age 45.1±1.3) and hemodialysis patients (HD; n=19, age 54.6±16) to healthy subjects (HS; n=22, age 35.9±7). Arm, leg, and whole body extracellular resistance (Re) was measured using a multiple-frequency bioimpedance device (Xitron™ 4000B) after dialysate drainage in PD, at the start and end of the HD, and in HS. Resistivity was calculated by p=A*Re/L (Ω·cm), where A is the cross-sectional area. Re is the extracellular resistance, and L is the length of the segment measured. To reduce the effect of body composition differences, resistivity was normalized by body mass index (ρN=ρ/BMI, 10−2 Ω·m3/kg). Significant differences in the ρN were found between PD and HS in the arm (8.6±1.7 vs 10.7±2.2, p<0.01) and in the leg (11.9±2.9 vs 15.5±3.6, p<0.01), as well as the HD and HS (9.3±1.5, p<0.05) in the arm but not in the leg lp=NS). PD and HD differed in the leg (p<0.01) but not in the arm (p=NS). The results suggest that PD patients are more hydrated than HD patients and that neither group has reached a state of normal hydration. The leg may differ from the arm because of the effect of gravity in accumulating period. Continuous measurement of ρN has been used in HD (Int J Artif Organs 2004; 27:104-9) and could be applied to continuous flow PD (Am J Kidney Dis 2003:42:167-72) and intermittent PD in which progressive reduction in body fluid volume occurs
Zhu F., Carter M., Kotanko P., Levin N.W., Renal Research Institute, New York, NY, U.S.A.