
Abstract

Bone Mineral Density, Arterial Calcifications, and Arterial Stiffness in Peritoneal Dialysis Patients
Background: The usefulness of bone mass measurements to estimate the risk of fracture is not well established in patients on peritoneal dialysis (PD). Objective: Evaluate the correlation of vascular calcifications, arterial stiffness, and calcium-phosphorus metabolism factors with bone mineral density (BMD) in PD Methods: 70 PD patients (37 male, 24% diabetic), mean age 53±14 years, mean follow-up 30±25 months. Aortic stiffness was measured by carotid-femoral pulse wave velocity (PWV). We used a vascular calcification score (vsc) based on plain radiographic film of pelvis and hands. BMD was studied by dual energy x-ray absorptiometry of lumbar spine (L) and femoral neck (F). Biochemical parameters: time averaged for the 6 months preceding BMD evaluation. Results: Absence of vascular calcifications in 39%. F showed lower values of BMD (L 0.965 mg/cm2, F 0.717 mg/cm2, p<0.001) and T score (L1.02, F 1.39. p=0.02). Osteopenia and osteoporosis range, as defined by WHO criteria, were present at L in 41% and 17%, and at F in 41% and 21%. Comparing tertiles of patients based on F-BMD: 0.313 to 0.673, 0.680 to 0.776, and 0.788 to 1.053 mg/cm2, BMD was significantly lower in patients with vascular calcification (p=0.004) and high prevalence of cardiovascular disease (p<0.001). Patients with lower BMD were older (p=0.02), had increased vascular stiffness (8.7±11.9, 7.8±1.4, and 7.3±1.3 m/s, p=0.01), lower albumin (p=0.02) and ejection fraction (33.6±9.3, 37.6±7.6, 41.5±8.7, p=0.02). Higher vsc was associated with lower F-BMD and lower T score. PWV was inversely correlated with F-BMD (r=0.174, p<0.001) and F-T score (R=0.064, p=0.03). The BMD is independently and inversely associated with PWV (B=-0.415: 95% Cl: -0.053-0.0016, p<0.001). Conclusions: In these PD patients, arterial calcifications and arterial stiffness are inversely associated with BMD evaluated at femoral neck, site of mixed bone, cortical and trabecular.
Adragao T.1, Branco P.2, Birne R.1, Silva S.2, Rosa N.2, Nascimento C.1, Goncalves M.1, Bruges M.1, Almeida E.2, Prata M.M.2, Pais M.J.1, Nephrol Dept.1 Hosp Santa Cruz. Carnaxide; Nephrol & Transplantation Dept,2 Hosp Santa Maria, Lisbon, Portugal.
Outcome of Peritoneal Dialysis Patients with Ischemic Heart Disease Submitted to Percutaneous Coronary Intervention
Background: Cardiovascular disease is prevalent among patients on continuous ambulatory peritoneal dialysis (CAPD) and many of them require percutaneous coronary intervention (PCI) We analyzed the outcome of CAPD patients submitted to PCI in our center.
Design: We retrospectively analyzed all records of ESRF patients who underwent PCI after commencement of CAPD from 1 January 2001 to 31 December 2005. Baseline demographic data were recorded and cardiovascular outcome in terms of death and recurrent myocardial infarction (AMI) were measured.
Results: 11 patients (males:females=3:8) were included. Manage of patients at time of PCI was 60±14 years PCIs were performed at a mean of 14.0±13.6 months after commencement of CAPD. Six patients had coexisting DM and 5 patients had hyperlipidemia. Mean hemoglobin level was 8.9±1.0 g/dL, mean phosphorous level was 1.65±0.43 mmol/L, and mean cholesterol level was 5.30±0.83 mmol/L. All procedures were done successfully. Two patients received bare metal stents, 7 had non-drug- eluted stents, and 2 had drug-eluted stents There was no peri-procedure mortality. Five patients (45.4%) had recurrent AMI at 1 year. During the follow-up 3 (27.2%) patients (2 male, 1 female) died post-PCI due to recurrent AMI Survival at 1 month was 100%, 3 months 79.8% and 6 months 68.4% Mean survival was 2.37±0.47 years There was no significant difference in mortality with respect to patient's gender, type of coronary stent used, and comorbidities (diabetes and hyperlipidemia).
Conclusion: Ischemic heart disease still carried a significant mortality and mortality in CAPD patients despite PCI Diffuse vasculopathy and multiple risk factors including inflammation, anemia, hyperphosphatemia, and vascular calcifications may contribute to poor survival benefit in ESRF patients with ischemic cardiomyopathy despite percutaneous coronary intervention.
Chan H.W., Chan Y.H., Liu Y.L., Cheung C.Y., Chak W.L., Wong H.S., Choi K.S., Chau K.F., Li C.S., Renal Unit Department of Medicine. Queen Elizabeth Hospital, Hong Kong.
Association between Hypoalbuminemia and Pulse Pressure in Patients on Continuous Ambulatory Peritoneal Dialysis (CAPD)
Background: Hypoalbuminemia was shown as a risk factor for cardiovascular events and mortality in dialysis patients but the underlying mechanism remained inconclusive. Meanwhile, elevated pulse pressure (PP) was proved to be a surrogate of arterial stiffness. We hypothesized that a possible link between hypoalbuminemia and cardiovascular disease might be arterial stiffness Thus, there should be a negative association between hypoalbuminemia and PP. This cross-sectional study was conducted in CAPD patients to validate this hypothesis Methods: Clinical stable CAPD patients (n=196, 85 M/111F) in a single center were included. The average age was 60±14 years and mean dialysis vintage was 19±17 months. Serum albumin, C-reactive protein (CRP), and brachial blood pressure were measured. Results: Patients were divided into 2 groups according to the serum albumin concentration: hypoalbuminemia group (<35 g/L) and normal albumin group. The 2 groups were matched in age, sex, and diabetes. PP in hypoalbuminemia group was significantly higher than that in normal albumin group (67±17 vs 55±17 mmHg, p<0.01). No difference was observed in serum lipid and antihypertensive medication between the 2 groups Serum albumin was negatively associated with systolic blood pressure (r=-0.211, p<0.01) and PP (r=-0.281, p<0.001), respectively Multiple regression analysis showed that PP was determined by age (odds ratio=0.451, p<0.05), body mass index (odds ratio=1.703, p<0.05), and serum albumin (odds ratio-2492, p<0.01). Lipids and inflammatory marker were not independent determinants of PP. Conclusion: Hypoalbuminemia was closely associated with increased pulse pressure in PD patients. Serum albumin in addition to age and body mass index, was an independent risk factor for elevated pulse pressure in CAPD patients, suggesting that increased arterial stiffness might be the link between hypoalbuminemia and cardiovascular events and mortality in dialysis patients.
Cheng L.T.1, Tang L.J.3, Wang T.2, Division of Nephrol,1 Peking Univ First Hospital; Division of Nephrology,2 Peking University Third Hospital, Beijing: Division of Nephrology,3 Qilu Hospital of Shandong University, Jinan, China
Seasonal Variation of Blood Pressure in Patients on Continuous Ambulatory Peritoneal Dialysis (CAPD)
Background: Seasonal variation of blood pressure (BP) has been observed in hemodialysis and renal transplanted patients However, this phenomenon in CAPO patients-who are characterized by distinct hemodynamics from hemodialysis patients has not been reported before In addition, the contribution of extracellular water (ECW) in seasonal variation of BP is not clear. Methods: All stable CAPD patients (n=122) dialyzed in a single center from 1 January 2003 to 12 December 2004 were studied. Systoli blood pressure (SBP), diastolic blood pressure (DBP), weight, and ECW (by bioimpedance analysis) were measured in every patient Climatic data were obtained from Beijing Weather Bureau, China. These data were pooled together and grouped according to natural month Results: In general, apparent seasonal variation of BP was observed in CAPD patients. BP begun to decrease from spring and reached the lowest level in summer, then increased from autumn and reached its peak in winter. Seasonal variation of BP in male patients was similar with that in female patients, but diabetic patients did not show apparent seasonal vacation of BP compared with nondiabetic patients. SBP and DBP negatively correlated with average atmospheric temperature (r=-0.768, p<0.001 and r=-0.764, p<0.001, respectively). BP also negatively correlated with rainfall and humidity but this correlation disappeared when temperature was controlled in partial correlation Weight and ECW fluctuated throughout the year but showed no seasonal variation. Conclusion: There was apparent seasonal variation in blood pressure in CAPD patients on the whole Diabetic patients did not show apparent seasonal variation in blood pressure as nondiabetic patients did. The seasonal variation of BP was more influenced by temperature than rainfall and humidity, and the change in extracellular water was not seasonal, suggesting other mechanisms such as total peripheral resistance might play a more important role in this phenomenon.
Cheng L.T.1, Jiang H.Y.3, Tang L.J.4, Wang T.2, Div of Nephrol,1 Peking Univ 1st Hosp; Div of Nephrol2 Peking Univ 3rd Hosp, Beijing; Div of Nephrol,3 2nd Affiliated Hosp of Kunming Med Coll, Kunming; Div of Nephrol,4 Qilu Hosp of Shandong Univ. Jinan, China.
Peritoneal Albumin Clearance is Related to Cardiovascular Disease and Independently Predicts Poor Outcome in Peritoneal Dialysis Patients
Dialysis patients have a markedly increased mortality due to cardiovascular disease (CVD), and it has recently been reported that increased peritoneal albumin transport is related to mortality in peritoneal dialysis (PD) patients We measured peritoneal albumin clearance (PalbCI) from a 24-hour dialysate collection in 148 incident PD patients closely after start of PD. Markers of inflammation (IL-6, hs-CRP, p-albumin) had been measured in the same patients before start of dialysis (usually in the morning just before catheter insertion). Presence of atherosclerosis defined as carotid plaques (ultrasound) was determined in a subgroup (n=59) of the patients.
PalbCI was significantly higher in patients with a history of CVD (0.114±0.053 vs 0.084±0.036, p<0.0001), and in patents with carotid plaques (0.122±0.054 vs 0.082±0.035. p=0.01), whereas there was no difference between diabetics and nondiabetics. PalbCI correlated to IL-6 (rho=0.22, p=0.01) but there was no relation between PalbCI and hs-CRP. There was a significant inverse relation between PalbCI and P-albumin before start of PD (r=-0.27. p<0.001), 55 patients died during the followup period of 52±37 months In a Cox multivariate analysis PalbCI predicted mortality (p=0.015) independently of CVD (p=0.03), diabetes (p=0.004), age (p<0.001), and log IL-6 (p=0.06).
We conclude that PalbCI is closely related to atherosclerosis and predicts mortality independently of clinical CVD in PD patients. The relation between PalbCI and plasma albumin levels before start of PD suggests that PalbCI is related to increase in vascular permeability, possibly reflecting a more general vascular disease at start of PD Peritoneal albumin clearance is likely to be a marker of endothelial function in PD patents.
Heimbürger O., Hilderman M., Axelsson J., Stenvinkel P., Tong M., Pecoits-Filho R., Lindholm B., Karolinska, Stockholm, Sweden
No Association of Peritoneal Albumin Excretion with Preexisting Cardiovascular Disease and Systemic Inflammation in New Peritoneal Dialysis (PD) Patients
Background: Microalbuminuria is a well-known risk factor and a predictor of cardiovascular disease (CVD) in patients (pts) with chronic kidney diseases. Recently, researchers found that peritoneal albumin excretion was related to the CV events and all-cause mortality in PD pts. Objectives: We evaluate the association of peritoneal albumin excretion and IL-6 level with preexisting CVD and diabetic status in the new PD pts Patients and Methods: In this multicenter cross-sectional study, we enrolled 85 pts who started PD Preexisting CVD was defined as angina, history of myocardial infarction, cerebrovascular disease, or peripheral arterial disease. Modified peritoneal equilibration test (PET) was performed within 2 months after the initiation of PD At that time peritoneal albumin and protein excretion, serum and dialysate IL-6, C-receive protein (CRP) level were measured. Results The age (mean±D) was 49.5±14 years and male-to-female ratio was 1.3. The estimated GFR (by MDRD equation) at the start of PD was 7.9±3.79 mL/min/1.73 m2. DM and CVD were present in 40% and 28% of pts, respectively. The peritoneal albumin concentration and dialysate-to- plasma (DIP) albumin ratio were correlated with the DIP creatinine ratio at 4 hours (r=0552, p<0.001), and were higher in the high-average/high transporter group than in the low-average/low transporter groups (630±202 vs 410±162 mg/L & 0.19±0.008 vs 0.12±0.005, respectively; p<0.001). The peritoneal albumin concentration was closely correlated with the dialysate IL-6 level (r=0.424, p<0.001), but not with the serum IL-6 and CRP levels. There were no differences in peritoneal albumin excretion with respect to the diabetic status or preexisting CVD Conclusion: Peritoneal albumin concentration was associated with peritoneal small solute transport and dialysate IL-6 level, but not with preexisting CVD and markers for systemic inflammation in the new PD pts. Prospective study will fallow in order to verify the role of peritoneal albumin excretion as a predictor of CV events.
Increased Carotid Intima-Media Thickness is Related to Peritoneal Membrane Permeability of Creatinine
Objective: Little information is available as to the prevalence of atherosclerotic systemic disorders in patients treated with peritoneal dialysis (PD) Particularly, it remains unknown how peritoneal membrane permeability of solutes is related to atherosclerosis We, therefore, wanted to reveal a relationship between dialysate-to-plasma ratio of creatinine (D/P Cr) at 2 hour of the dwell in peritoneal equilibration test and carotid intima-media thickness (IMT) as a surrogate marker of atherosclerosis.
Methods: Inclusion criteria were patients undergoing PD in our hospital for more than 12 months. Both carotid arteries were examined using 7.5 MHz linear array transducer and we recorded maximum IMT as we I as the presence or absence of plaque. Then, we defined thickened IMT if maximum IMT was greater than or equal to 1 mm The prevalence of thickened IMT was calculated and was related with D/P Cr or other blood chemical data.
Results: There were 23 patients (mean age 62.9 years; male 14, female 9) who had been treated with PD (mean PD duration 33.4 months) Thickened IMT was found in 10 of 23 patients, and also 10 patients had plaque. Patients with thickened IMT showed significantly increased D/P Cr ratio compared with those without thickened IMT (0.47±0.11 vs 0.36±0.10. p<0.05). Patients with thickened IMT had tendency to have higher plasma levels of fibrinogen, or to have diabetes mellitus. Regarding the presence or absence of plaque, there was a significant association with age (67.7±8.5 vs 69.2±9.8 years, p<0.05). Pulse blood pressure, serum levels of triglyceride Lp(a), total homocysteine (tHcy), and human atrial natriuretic polypeptide (hANP) were also higher in patents with plaque than those without plaque, although they did not reach statistical significance.
Conclusion: Patients with more advanced carotid arteriosclerosis have increased D/P ratio of creatinine in peritoneal membrane.
Ikee R., Oka M., Mano T., Moriya H., Ohtake T., Kobayashi S., Shonan Kamakura General Hospital, Kamakura, Japan.
Effect of Peritoneal Dialysis Solution Type on Serum Lipid Levels in End-Stage Renal Disease
Aim: Dyslipidemia accompanies end-stage renal disease and contributes to the high incidence of cardiovascular disease in patients on chronic peritoneal dialysis (CAPD) treatment However, there is not any data about the effect of peritoneal dialysis solution (PDS) type on serum lipid levels This study was designed to investigate the effect of PDS type on serum lipid levels.
Materials and Methods: 67 subjects were enrolled to the study. All were outpatients and free of acute illness. PDS types are including glucose ammo acids, and icodextrin. We divided patients into 3 groups: group A, 18 patients patient's taking only glucose; solutions; group B, 18 patients patient's taking glucose and amino acid solutions; and group C, 31 patients patient's taking glucose and icodextrin Serum levels of lipid profile including total cholesterol (TC), low-density lipoprotein (LDL-C), high-density lipoprotein (HDL-C), triglyceride (TG), lipoprotein(a) [Lp(a|], and Lp(b) were determined in all groups. Patients who used statin within 6 months were not included to the study.
Results No significant difference in TC, LDL-C. HDL-C, TG, Lp(a), and Lp(b) serum levels were found between group A, B, and C.

Conclusion: These results suggest that type of peritoneal solutions has no negative or positive effect on serum lipid levels.
Kanbay M., Kaya A., Aydogan T., Altay M., Koca C., Akcay A., Duranay M., Ramazan Yigitoglu Fatih University School of Medicine, Ankara, Turkey.
A Significant Difference in Leukocyte-Platelet Aggregates and Serum Levels of Osteopontin between Patients with CAPD and HD
Recently, the idea that micro-inflammation plays a key rote in atherosclerosis has received much attention. The formation of platelet-leukocyte aggregates (LA) may play an important role by facilitating platelet-endothelial interaction, thus leading to atherosclerosis. In this regard we have recently reported that blood rheology in hemodialysis (HD) patients by using micro-channel array flow analyzer (MC-FAN) that makes it possible to directly observe the flow of blood cell elements through the micro-channel is well related with high sensitive CRP as well as carotid intima-media thickness (Hemodial Int 2005; 9:268). Using this method, we wanted to compare the effect of 2 modalities, HD 8 CAPD, on a number of LA or serum levels of osteopontin (OPN) because OPN is known to play a role as an intermediary of macrophage infiltration or accumulation after endothelial dysfunction.
Using MC-FAN, we measured a number of LA during 50 μL flow of whole blood through micro-channels and serum levels of OPN in 18 patients (age 62±11. PD duration 39±30 months) with CAPD, or 118 patients (age 65±11, HD duration 67±61 months) with HD. In healthy individuals, the number of LA was 23.4±9.8, whereas in HD patients it was 48.2±16.4 (p<0.001). In patients with CAPD, the number of LA was 28.1±7.8, significantly lower than that in patents with HD. Flow cytometry demonstrated that in monocytes 16.9% of total monocytes were aggregated with platelets, in neutrophil 8.5%, and in lymphocytes 3.3%, respectively. Serum levels of OPN were significantly lower in PD patients than in HD patents (0.606±0.093 vs 0.845±0.365 μg/mL, p<0.05).
In conclusion, we showed that patients with CAPD are in better condition than those with HD in terms of proinflammation.
Kobayashi S., Oka M., Ishii T., Maesato K., Ikee R., Mano T., Monya H., Ohtake T., Shonan Kamakura General Hospital, Department of Nephrology, Kamakura, Japan.
Relationship between Heart Rate Variability and Left Ventricular Systolic Dysfunction of CAPD Patients
Cardiovascular (CV) autonomic dysfunction has teen proposed as an important mechanism that may explain at least part of this excess CV mortality We investigated how the autonomic nervous activity is associated with the presence of left ventricular (LV) dysfunction of CAPD patients (pts), Methods; 22 CAPD pts underwent an echocardiographic evaluation [LV ejection faction (EF; %)] and a 5-minute ECG record in supine and orthostatic position for time- and frequency domain heart rate variability (HRV) calculation standard deviation of normal-to-normal R-R intervals (SDNM, ms), square root of the median of SD (rMSSD), measurement of the % of differences between adjacent NN intervals more than 50 ms (pNN50; %) and high frequency (HF) component, and the ratio of low frequency component (LF) to HF (LF/HF). Results: 9 pts (41.5±0.7 years old. MMF=6/3; dialysis duration 40.3±6.7 months) had EF LV= 38.8±10.2% (group 1: G-1). The rest of the pts (44.5±6.7 yeare old; M/F=8/5; dialysis duration 38.3±9.7 months) had EF LV=85.1±5.9% (group 2; G-2). The results of HRV are shown in the Table.
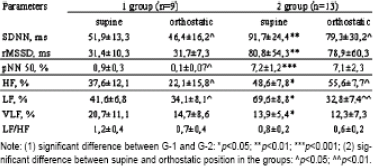
Note: (1) significant difference between G-1 and G-2:
p<0.05;
p<0.01;
p<0.001; (2) significant difference between supine and orthostatic position in the groups:
p<0.05;
p<0.01.
G-1 pts had significant low SDNN (51.9±13.3 ms vs 91.7±24.4 ms, p<0.01) pNN50 (0.9%±0.3% 69.3%±3.8%, p<0.05) in supine position than the G-2 pts, respectively During orthostatic test the parameters of HRV deeply depressed compare with the supine position in G-1 At the same tune HRV parameters in G-2 stayed unchangeable. We retested positive corrections between EF LV and HF component of HRV or CAPD pts with LV dysfunction (r=0.08; p<0.001).
Conclusions: These results suggest that CAPD pts with LV dysfunction have deeper parasympathetic and sympathetic dysfunction compare with the pts with preserved LV function.
Komissarov K.S., Pilotovich V.S., The National Center of Nephrology, Dialysis and Transplantation, Minsk, Belarus.
Role of Plasma Thrombin-Automatable Fibrinolysis Inhibitor Levels in Continuous Ambulatory Peritoneally Dialyzed (CAPD) Patients
Objectives: Recently, a new potent inhibitor of fibrinolysis, the thrombin-automatable fibrinolysis inhibitor (TAFI), has been isolated from human plasma The possibility that TAFI also participates in the mechanism of hypofibrinolysis has not been appraised in peritoneal dialysis (PD) patients. In the present study, we investigated the plasma levels of TAFI and its relation to urinary albumin excretion in patients maintained on CAPD with normo- and microalbuminuria.
Methods: 47 CAPD patients (29 with normoalbuminuria, 18 with microalbuminuria) and 45 age-matched normal subjects were enrolled in this study.
Results: The plasma level of thrombin-antithrombin complex was significantly increased (23.2±2.4 vs 7.9±1.3 nmol/L p<0.05) whereas the D-dimer/thrombin-antithrombin complex ratio was significantly decreased (14.6±1.2 vs 25.4±2.7, p<0.05), showing the occurrence of hypercoagulability and hypofibrinolysis in CAPD patients. The plasma level of TAFI in PD patients was significantly elevated, compared with normal subjects (136.1%±10.3% vs 97.4%±4.5%, p<0.05). The plasma level of TAFI in CAPD patients with microalbuminuria was significantly higher than the level in PD patients with normoalbuminuria (183.2%±23.4% vs 117.9%±11.9%. p<0.05) or normal subjects (188.6%±23.4% vs 98.7±14.3%, p<0.01). Univariate analysis showed that the plasma TAFI levels are significantly and proportionally correlated with urinary albumin excretion rate (r=0.53, p<0.05) and with plasma soluble thrombomodulin level a marker of endothelial cell damage, in all CAPD patients (r=0.47, p<0.05).
Conclusions: These data suggest that increased plasma level of TAFI may be involved in the mechanism of vascular endothelial damage in CAPD patients. Additional study is needed to explore possible mechanistic links between TAFI, inflammation, soluble adhesion molecules, and residual renal function in CAPD patients.
Korzh I.V., Fedotova I.F., Kharkov Medical University, Kharkov, Ukraine.
Number and Migratory Activity of Circulating Endothelial Progenitor Cells in Peritoneal Dialysis Patients
Objectives: Increased risk of cardiovascular disease in peritoneal dialysis (PD) patients has been explained by accelerated atherosclerosis and impaired angiogenesis, in which endothelial progenitor cells (EPCs) may play key roles. We hypothesized that altered EPC biology may contribute to the pathophysiology of cardiovascular complications.
Methods EPCs were determined in PD patients (n=53) and in a normal control group (n=52) by fluorescence-activated cell-sorting (FACS) analysis. Cells that were positive by flow cytometry for CD34/KDR/AC133 within the lymphocyte population were characterized as EPCs
Results: PD patients showed markedly decreased numbers of EPCs (43.7%) and colonies (74.5%) when compared with the controls (p<0.001). These findings were corroborated by 29.8% decrease in EPC migratory function in response to vascular endothelial growth factor (VEGF) (p=0.039) and 47.6% decrease in EPC incorporation into human umbilical vein endothelial cells (HUVEC) (p<0.001). In addition, Framingham's risk factor score of both PD patients (r=-0.472, p=0.01) and normal group (r=-0.376, (p=0.012) significantly correlated with the numbers of EPCs Indeed, the number of circulating EPCs was significantly lower in PD patients than in normal group under the same burden of risk factors (p<0.001).
Conclusions: EPC biology, which is critical for neovascularization and the maintenance of vascular function, is altered in PD patients. Our data strongly suggest that dysfunction of circulating EPCs has a role in the progression of cardiovascular disease in these patients.
Korzh O.M., Krasnokutskiy S.V., Kotchuev G.I., Kharkov Medical Academy of Postgraduate Education, Kharkov, Ukraine.
Significance of Endothelial Cell-Derived Microparticles in Patients Undergoing Continuous Ambulatory Peritoneal Dialysis (CAPD)
Objectives: Endothelial cells, platelets, and oxidized low density lipoprotein (LDL) could play very important roles in the development of vascular injury in peritoneal dialysis (PD). The aim of this study was to investigate the role of plasma endothelial cell-derived microparticles (EDMP) in patients undergoing CAPD.
Methods: We studied 52 CAPD patients and 49 age- and sex-matched healthy controls by measuring their levels of plasma EDMP, platelet- derived microparticles (PDMP), platelet-P-selectin (plt-PS), soluble CD40 ligand (sCD40L), and ant-oxidized LDL antibody.
Results The concentrations of EDMP. PDMP, plt-PS, and sCD40L in CAPD patients were significantly higher than those in normal subjects Levels of anti-oxidized LDL antibody were also higher in CAPD patients than in control subjects In addition anti-oxidized LDL antibody levels correlated with EDMP. PDMP plt-PS, and sCD40L levels in CAPD patients Oxidized LDL increased expression of plt-PS and promoted shedding of PDMP. On the other hand, activated platelets and PDMP promoted endothelial cells and THP-1 (monocytic cell line) interaction, and membrane vesiculation occurred in the presence of oxidized LDL.
Conclusions: These findings suggest that activated platelets and oxidized LDL induce EDMP generation, and that elevated EDMPs may be a sign of vascular injury in CAPD patients. It may lead to fibrin deposition in the vascular wall thrombus formation, and development and progression of atherosclerosis with its complications.
Korzh O.M., Pavlova O.O., Krasnokutskiy S.V., Kharkov Medical Academy of Postgraduate Education, Kharkov, Ukraine.
A Prospective Study on the Predictive Value of Conventional and Emerging Risk Factors on Cardiovascular Mortality in a Cohort of Peritoneal Dialysis (PD) Patients without Preexisting Cardiovascular Disease (CVD)
Background: Patients (pts) with end-stage renal disease (ESRD) face a particularly high risk of CVD. The increased risk is partly due to a higher prevalence of established risk factors such as hypertension, diabetes mellitus (DM), smoking, and anemia. Increase in C-reactive protein (CRP), hyperhomo- cysteinemia, nutritional status and disordered lipid metabolism represent factors are recently recognized as CV risk factors of emerging importance. Objectives and Design: This is a prospective observational study to determine the predictive value of traditional and emerging risk factors on CV mortality in a cohort of PD pts without preexisting CVD. Study Population: A prospective follow-up of 186 pts with ESRD without preexisting CVDs receiving PD between year 2001 and 2004 were carried out Initial measurement of serum CRP homocysteine (Hcy) level, nutritional data [body mass index (BMI), serum albumin, and lipid profile], demographic data and preexisting diseases (history of DM, hypertension, and smoking) were obtained at the start of the cohort study. CV and all-cause mortality were determined during the 4-year follow-up period. Results: By Cox regression multivariate analysis, every 1-mg/L increase in CRP was independently predictive of a 3% increase in CV (95% Cl 1.00-1.05, p<0.05) and 1% increase in overall mortality (95% Cl 1.01-1.02, p<0.001). Every 1-year increase in age was independently associated with 7% increase in CV (95% Cl 1.03-1.12, p=0.001) and 5% increase in overall mortality (95% Cl 1.03-1.07, p<0.0001). History of DM was also an independent risk factor predictive of CV as well as overall mortality. In contrast plasma concentration of Hcy level, BMI, and plasma cholesterol and triglyceride levels were not associated with the different causes of mortality. Conclusion In this study, we conclude that history of DM and plasma CRP level were independently associated with CV and overall mortality in a group of PD pts without preexisting CVDs, while hyperhomocysteinemia, dyslipidemia, and BMI did not predict CV or overall mortality on multivariate analysis.
Liu Y.L., Chan Y.H., Wong K.M., Wong H.S., Chan H.W., Cheung C.Y., Chak W.L., Choi K.S., Chau K.F., Li C.S., Queen Elizabeth Hospital, Hong Kong, China.
Intima Media Thickness Correlations with Serum Lipids and Some Hemostatic Parameters in CAPD and Hemodialysis Patients
Background: Cardiovascular disease (CVD) is a leading cause of death in patients (pts) on renal replacement therapy Increased concentration of fibrinogen, dyslipidemia, and impaired fibrinolysis are regarded as important risk factors for CVD. Intima media thickness (IMT) of the common carotid artery is related to coronary and cerebrovascular arterial disease. Thrombin automatable fibrinolysis inhibitor (TAFI) is recently discovered inhibitor of the fibrinolytic system. The a m of the study was to evaluate whether IMT is related to some hemostatic factors [prothrombin fragments 1+2 -F1+2, throm- bin-antithrombin complexes (TAT)], plasmin-antiplasmin complexes (RAP), fibrinogen, euglobulin clot lysis time (ECLT), TAFI, thrombomodulin, in peritoneal (PD) and hemodialysis (HD) population. Methods: The study was performed on 80 chronically dialyzed pts (27 on PD & 53 on HD) Hemostatic parameters were measured with commercially available kits Results: PD pts had significantly higher concentration of cholesterol. LDL triglycerides, and C-reactive protein and lower of total protein and albumin than HD group Fibrinogen. TAFI concentration and activity, F1+2 were elevated significantly in PD pts compared to HD. Thrombomodulin was lower prothrombin time (PT) and activated partial thromboplastin time (APTT) were significantly prolonged in HD pts over PD Significant positive correlations were found between fibrinogen or triglycerides and TAFI activity only in PD pts. In univariate analysis IMT correlated significantly with age. (r=0.7, p<0.001), cholesterol (r=0.6, p<0.01). CRP (r=0.4, p<0.05), fibrinogen (r=0.5, p<0.05), hemoglobin (r=0.5, p<0.01), PT (r=0.56, p<0.01), APTT (r=0.59, p<0.01), and iron (r=-0.53, p<0.05) in PD pts. IMT correlated with age (r=0.6, p<0.05), PT (r=0.52, p<0.05), and iron (r=-0.54, p<0.05) in HD pts. Conclusions Triglycerides and fibrinogen correlated with TAFI activity only in subjects on PD This phenomenon may predispose PD pts to the suppression of fibrinolysis Correlations between IMT and Hb may implicate the role of these rheological factors in progression and acceleration of arterial remodeling in PD population
Malyszko J., Malyszko J.S., Brzosko S., Pawlak K., Mysliwiec M., Medical University, Department of Nephrology, Bialystok, Poland.
Hyperuricemia: A Predictive Risk Factor for Cerebro-Cardiovascular Disease among Hemodialysis Patients but Not among Peritoneal Dialysis Patients
Background: Recent basic and clinical studies have shown that hyperuricemia is associated with cerebro-cardiovascular disease (CCVD). Although hyperuricemia is common among dialysis patients, little is known about the relationship between hyperuricemia and CCVD among dialysis patients.
Aim: We conducted a case control study to evaluate the association between hyperuricemia and CCVD among dialysis patients.
Methods: The 28 hemodialysis (HD) and 9 peritoneal dialysis (PD) patients who developed CCVD after 1 year of starting dialysis were selected as cases. The 48 HD and 17 PD patients are randomly selected and matched for age, gender, and medical history of CCVD We evaluated the serum uric acid, albumin, and CRP at the onset, 1 month. 6 months, and 1 year before the CCVD event, and analyzed the time-dependent risk, using logistic regression analysis.
Results: There was no significant difference in dialysis periods, diabetes between cases and controls. In HD patients, serum uric acid at 1 year before the CCVD event was significantly higher than in control (case 8.3±1.3, control 7.5±1.4 mg/dL, p=0.02). However, we could not find significant difference among PD patients (case 7.0±1.3, control 7.4±1.2 mg/dL, NS). The average of CRP is higher and the average of albumin is lower at all points studied in both groups (CRP: HD case 0.3, HD control 0.1, PD case 0.6, PD control 0.3 mg/dL; albumin: HD case 3.8, HD control 3.9, PD case 3.6, PD control 3.8 g/dL) 1 year before the event Logistic regression analysis showed that the adjustment odds ratio for uric acid was 1.45 (95% Cl 1.0-2.1) in HD patients.
Conclusion: The present study suggests hyperuricemia may be a predictive risk factor of CCVD in HD patients, but not in PD patients.
Mashimo Y., Komatsu Y., St. Luke's International Hospital, Tokyo, Japan
Correlation of Cardiac Dysfunction with BNP and Adequacy of Dialysis in South Indian CAPD Patients
Background: There is a paucity of data on correlating plasma BNP with left ventricular (LV) diastolic dysfunction (DD) in CAPD patients (pts). This prospective study aims to correlate plasma BNP in prevalent CAPD pts with LV-DD, dialysis adequacy, and calcium and phosphorus levels Aim: To identify what determines DD in CAPD patents and if there is a correlation with the seventy of DD and BNP values Methods and Materials: Study group consisted of 22 pts (males 15, females 7) on CAPD for a minimum period of 2 months with no history of preexisting cardiac and lung disease. They should also have had no peritonitis in the past 2 months. Mean age was 56.09±11.72 years. ESRD was due to hypertensive or diabetic nephropathy in 18, ADPKD in 2, and CGN in 2. They had baseline ECG and Echo. Hemoglobin, hematocrit blood urea nitrogen, serum creatinine, electrolytes, Ca and P estimation. Adequacy of dialysis was done weekly (Kt/V). Serum BNP done (Micro Particle Enzyme Immunoassay). M mode, 2-dimensional and Doppler Echo study done by a single experienced observer and the following parameters determined: maximal early diastolic flow velocity (E. max), maxima late atrial few velocity (A. max), E/A ratio, left atrial dimensions (LAD), LV end diastolic diameter (LViDD), isovolumetric relaxation time (IVRT), section fraction (EF), LV mass (LVM), LV mass index (LVMI), and regional wall motion abnormalities (RWMA: Results: Mean duration of PD was 20.64±0.2114 months, serum Ca 925911.124 mg/dL, P 4.327±1.407 mg/dL, E max 0.8150±0.3124 msec, A. max 0.8018±0.2873 m/sec, LAD 38.009±7.134 mm, LVDD 51.364±14.122 mm, IVRT 98.41±45.89 m/sec, LVM 187.41±53.98 g, LVMI 115.550±31.878 g/m2, EF 67.50%±10.3%. BNP 624.0768±883.6108 pg/mL. There were negative correlations between adequacy and LAD (p=0.029), LviDD (p=0.034), and serum BNP (p=0.035). Serum BNP3 also correlated positively with E. max (p=0.001), LAD (p=0.001), LViDD (p=0.023), LVM (p=0.068). There was a negative correlation between BNP and A. max (p=0.005). There was also a significant correlation between s. Ca and E.max (positive: (p=0.038) and A max (negative) (p=0.010). Conclusion: Correlations between adequacy: LAD, LV DD, and serum BNP points toward the predominant effect of fluid overload on DD. It also indicates the possible use of serum BNP as a surrogate marker of fluid remora in CAPD pts with preexisting heart disease. Significant correlations between the different parameters of DD and serum BNP makes serum BNP a reliable marker of DD in CAPD pts Serial evaluation can predict card ac morbidly and mortality in CAPD pts The significant correlated between serum Ca and E.max (pos) and A.max (neg) indicates a possible effect of electrolytes on DD
Matthew V.2, Surendranath A.1, Abraham G.1, Sri Ramachandra Medical College & Research Institute,1 Madras Medical Mission Hospital2 Chennai, India.
The Hemodynamic Effects Observed during Peritoneal Dialysis Fluid Drainage and Instillation Do Not Adversely Affect Regional Left Ventricular Function or Troponin T Levels
CAPD patents have greatly increased rates of cardiovascular morbidity and mortality We have previously demonstrated that hemodialysis can induce regional left ventricular (LV) wall motion abnormalities, probably reflecting subclinical myocardial ischemia. We therefore performed a study to examine whether new LV regional wall motion abnormalities (as a surrogate marker of subclinical myocardial ischemia) develop in response to the marked hemodynamic changes that have been described in association with CAPD. 10 patents were studied, none with atherosclerosis and only 2 had LVH. 2-D echocardiography was performed before and after draining then instilling 2.5 L of dialysate. Images were analyzed to assess ejection fraction (EF) and regional systolic function in each of 10 LV regions (SF). Throughout this period, blood pressure (BP) and a full range of hemodynamic variables were measured using noninvasive pulse wave analysis. cTnT levels were measured before and 150 min after the study period. During drain periods BP fell, and rose during instillation. These changes were due to peripheral resistance falling upon fluid drainage and rising on instillation. There was an extremely low frequency of LV regions that displayed reduced wall motion following the drain-fill period (<5%). Mean SF increased in 4 of the 10 LV regions, as did overall mean SF (p<0.001). Mean EF and SF in the other 6 regions remained unchanged cTnT levels were low with a mean of 0.02±0.01 g/L (in keeping with patent demographics) and did not rise following the drain/fill period.
In a cohort of CAPD patients with little atherosclerosis or structural heart disease the hemodynamic effects observed during the drainage of fluid into and out of the abdominal cavity did not produce any signs indicative of subclinical myocardial ischemia It remains to be seen whether LV regional wall motion abnormalities occur in response to these hemodynamic changes in higher risk patients.
Selby N.M., Fialova J., McIntyre C.W., Derby City Hospital, Derby, United Kingdom.
Peritoneal Dialysis is Associated with Less Progressive Vascular Calcification than Hemodialysis
Vascular calcification (VC) plays an important role in the pathophysiology of cardiovascular disease in CKD The natural history of arterial calcification remains largely undefined. The objective of this study was to prospectively investigate the determinants and cardiovascular functional consequences of VC. 134 subjects [28 peritoneal dialysis (PD),60 hemodialysis (HD), and 46 CKD-4] were studied. Patients were studied at baseline and 12 months later. VC was assessed using multi-slice spiral CT scanning of a 5 cm standardized segment of superficial femoral artery (SFA). Calcification scoring was undertaken using the Agatston score. Pulse wave analysis and pulse wave velocity (PWV) were utilized to assess arterial compliance Further digital arterial pulse wave analysis (Finometer®) was used to generate additional data on systemic hemodynamics. All medications were recorded and biochemical parameters were time-averaged over 12 months. 117 patients remained to be studied at 12 months (8 patients were lost to FU and 10 died). 9/10 patients who died had VC. Progressive calcification was seen in 71/113 subjects calcification score increased from a median of 45 (95%Cl 209-397) to 62 (95%CI 209-527) at 1 year (p<0.0001). The HD group demonstrated significantly greater degree of progression than the PD or CKD-4 groups (p=0.002). 20/46 CKD-4 patients initiated dialysis HD appears to be associated with a greater Increase in arterial calcification on commencing dialysis than PD. Change in VC significantly correlated with decreased vascular compliance (ΔPWV) (r=0.55, p<0.001). Mean time-averaged serum phosphate, corrected calcium and calcium × phosphate product were 1.6±0.36 mmol/L, 2.44±0.14 mmol/L and 3.7±0.12 mmol2/L respectively.
In conclusion, CKD-4 and -5 patients with preexisting VC exhibit significantly increased calcification despite excellent mineral control.
Signst K.M., Priestman W., Bungay P., McIntyre C.W., Derby City General Hospital, Derby, United Kingdom.
An Association between Aortic Pulse Wave Velocity, Inflammation, and Calcification Regulatory Proteins in Patients Treated with Peritoneal Dialysis
Background: Arterial stiffness in end-stage renal disease (ESRD) appears to be complicated and multifactorial process. Inflammation and increased vascular wall calcification mediated by proteins involved in the controlling of bone metabolism may account for this process The aim of this study was to evaluate an association between aortic stiffness, assessed using pulse-wave velocity (AoPWV) measurement and substances that reflect the degree of inflammation, and those involved in bone metabolism and presumably in vascular calcification in uremic patients. The material of this study comprised of 55 peritoneal dialysis (PD) patients (age 53.2±12.7 years, on PD for 42.7±288 months) Serum hsTNF-α, IL-6, osteocalcin, osteoprotegerin, fetuin, matrix gla protein and phosphatonin FGF23 were assessed using ELISA, whereas hs-CRP with nephelometry. AoPWV was measured with Compilior Colson device with dialysate completely drained out. Results: Mean AoPWV value was 12.4±3.89 m/s. In Table 1 the associations between AoPWV and serum levels of tested biochemical parameters are summarized. No association was found between PWV and hs-CRP, fetuin, matrix gla protein, or FGF23.

Conclusion: Obtained results may suggest that except for inflammation, bone metabolism may also interact with aortic stiffening. Osteocalcin, the marker of osteoblastic activity and bone formation seems to adversely impact on the arterial stiffening, whereas osteoprotegerin, considered by some authors as the marker of low bone turnover, may promote aortic stiffness.
Stompor T.1, Dubiel M.2, Stompor M.2, Krzanowski M.1, Janda K.1, Kusnierz B.3, Zdzienicka A.3, Grocdzicki T.2, Dembinska-Kiec A.3, Naskalski J.3, Sulowicz W.1, PD Unit,1 Chair & Dept of Nephrol; Dept of Intern Med & Geriatrics.2 Dept of Clin Biochem,3 Jagiellonian Univ. Cracow Poland.
An Association between Parameters of Skin Microcirculation and Echocardiographic Indices in Patients Treated with PD
Background: Several preliminary reports suggest that patents (pts) with advanced heart failure display abnormalities in microvasculature, including skin microcirculation. However, the data concerning this issue in pts treated with peritoneal dialysis (PD) are scarce. In this preliminary report we aimed to study an association between several perimeters of skim microcode and echocardiography (echo-CG) findings in pts treated with PD. Material and Methods: The material of this study comprised of 55 PD pts (age 53.2±12.7 years on PD far 42.7±28.8 months). Skin microcircuit bleed flow was assessed using skin laser Doppler flowery (LDF; Periflow Sweden). The following indices were obtained: mean blood flow under basal conditions (MF1); area under curve of flow recorded after a 3-minute occlusion and during the first 5 seconds after cuff deflation (ADC1); peak flow during post-occlusive reactive hyperemia, expressed as an absolute value (PFP) and % increase vs MF1 (PFP%); mean bleed flow at the temperature of 44°C (MF44), and area under curve at 44°C (AUC44). Echc-CG was performed using Hewett Packard Sonos 2000 equipment. Left ventricle internal diameter (LVID; cm), posterior wall thickness (PWT; cm), and ventricular septum thickness (VST; cm) in systole and diastole were measured Ejection fraction (EF%) was calculated using Teicholtz method and LV mass (LVM; g) with Devereux formula. LVM was normalized to body surface area (LVM; g/m2). Results: In Table 1 we show the parameters of microcode in our study group; in Table 2 the correlations between tested skin microcircuit parameters and echc-CG indices are summarized. No correlation was found between echo-CG findings and MF1 PFP, and PFP%, as well as between EF% and none of the tested microcirc parameters Pts with LV hypertrophy were characterized with significantly lower values of PFP, PFP%, MF44 and AUC44 (p<0.05 for all differences, vs pts without hypertrophy). Conclusion: Our results indicate that impaired reactive vasodilation identified after the temperature stimulus may be associated with LV hypertrophy in pts on PD.

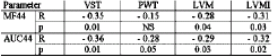
Stompor T.1, Dubiel M.2, Stompor M.2, Sorysz D.3, Krzanowski M.1, Janda K.1, Dubiel J.3, Grodzicki T.2, Suowicz W.1, PD Unit,1 Chair & Dept of Nephrol; Dept of Intern Med & Geriatrics,2 II Dept of Cardiol,3 Jagiellonian Univ, Cracow, Poland.
An Association between Skin Microcirculation and Inflammation in Patients Treated with Peritoneal Dialysis (PD)
Background: Several preliminary reports suggest that patients (pts) with advanced renal failure develop abnormalities in skin microcirculation. However, the data concerning this issue in pts treated with PD are scarce The chronic “non-specific” inflammation is considered the important factor that promotes the development and progresses of several cardiovascular pathologies in pts with end-stage renal disease The association between systemic inflammation and microcirc has rot been studied in PD pts to date. The aim of the present study was to analyze selected parameters of skin microcline in relation to several measures of inflammation in pts treated with PD Material and Methods. The material of this preliminary report comprised of 55 PD pts (age 53.2±12.7 years, or PD for 42.7±28.3 months). Sen microcirc blood flow was assessed using skin laser Doppler flowmetry (LDF; Periflow Sweden) The blowing indices were obtained: mean blood flow under basal coeditors (MF1); area under curve of flow recorded after a 3-minute occlusion and during the first 5 seconds after cuff deflation (AUC1); peak flow during post-occlusive reactive hyperemia, expressed as an absolute value (PFP) and At increase vs MF1 (PFP%); mean blood flow at the temperature of 44°C (MF44), and area under curve at 44°C (AUC44) Serum hs-TSF, circulating TNF receptor. IL-β, IL-8 levels (all using ELISA), hs-CRP and fibrinogen (nephelometry) we measured as the parameters reflecting an inflammatory process The TNF/TNF-R ratio was also calculated Results: In Table 1 we show the parameters of microcirc in our study group; in Table 2 the correlations between tested skin microcirc parameters cytokines, and acute-phase proteins are summarized Conclusion. Our results suggest that inflammatory cytokines and acute-phase proteins may negatively affect both basal blood flow in the skin microcirc as well as its response to the temperature and/or ischemic stimulus, although the strong positive association between TNF/ TSF-R ratio and post-occlusive flow increase is difficult to interpret

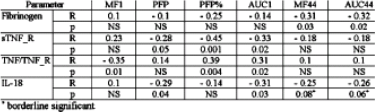
borderline significant.
Stompor T.1, Stompor M.2, Dubiel M.2, Kusnierz B.3, Krzanowski M.1, Janda K.1, Naskalski J.3, Grodzicki T.2, Sulowicz W.1, PD Unit,1 Chair & Dept of Nephrol Dept of Intern Med & Geriatrics,2 Dept of Clin Biochem,2 Jagiellonian Univ, Cracow, Poland.
Lack of Difference in Skin Microcirculation Parameters between Peritoneal Dialysis (PD) Patients and Subjects with Functioning Kidney Graft
Background: Several preliminary reports suggest that patients (pts) with advanced renal failure develop abnormalities in skin microcirculation However, the data concerning this issue in pts treated with PD are scarce. The aim of the present study was to compare the skin microcirc parameters between pts treated with PD and those with functioning kidney graft (RTx). Material and Methods The material of this preliminary report comprised of 55 PD pts (age 53.2±12.7 years, on PD for 42.7±28.8 months) and 16 pts with functioning kidney graft (age 44.0±11.8 years, p<0.01 vs PD; 39.2±4.52 months post-RTx: mean GFR 65.9±23.4 mL/min/1.73 m2). All RTx pts were previously treated with PD. Skin microcirc blood flow was assessed using skin laser Doppler flowmetry (LDF Periflow, Sweden). The following indices were obtained; mean blood flow under basal conditions (MF1); area under curve of flow recorded after a 3-minute occlusion and during the first 5 seconds after cuff deflation (AUC1); peak flow during post-occlusive reactive hyperemia, expressed as an absolute value (PFP) and % increase vs MF1 (PFP%); mean blood flow at the temperature of 44°C (MF44), and area under curve at 44°C (AUC44). Results: In Table 1 the comparison between pts on PD and those with functioning graft is summarized Conclusion: Quite unexpectedly and unlike in the case of several other cardiovascular parameters, we failed to demonstrate any significant difference in skin microcirc between PD and RTx pts, despite significant age difference between the 2 pt groups. This may suggest that the variables that can possibly modify the skin microcirc in PD pts persist after RTx.

Stompor T.1, Dubiel M.2, Stamper M.2, Krzanowski M.2, Janda K.1, Grodzicki T.2, Sulowicz W.1, PD Unit,1 Chair & Dept of Nephrology; Department of Internal Medicine and Geriatrics,2 Jagiellonian University, Cracow, Poland.
What Happens with Coronary Artery Calcification in PD Patients after Long-Term Follow-up: Must They Really Turn into Stone?
Background: Long-tern observations concerning trends in coronary artery calcification in dialysis and transplant patients (pts) are lacking. The aim of this preliminary nary study is analyze the long-term follow-up changes in coronary artery qualification score (CaSc) in pts on peritoneal dialysis (PD). Material and Methods: In the years 2001 and 2002 we performed CaSc using multi-slice spiral computed tomography (MSCT) in 63 ESRD pts treated with PD. In 2005 (after mean period of 38.6±6.2 months, i.e. after >3 years on average) we repeated this assessment in 20 subjects who were still on PD. From refraining 43 pits 6 died. 8 were switched to hemodialysis, 21 were transplanted, and 6 were continuing PD but refused to repeat MSCT or were not suitable to undergo this examination (mostly due to arrhythmia) This report is limited to those PD pts who survived and had repeated long-term follow-up MSCT. Results: in Table 1 we show the baseline and follow-up CaSc as we as the absolute difference between these 2 values (ΔCaSc) for a pts, and we split into 2 categories these who progressed and those in whom CaSc remained stable. Pts who stabilized did not differ at baseline from those who processed in terms of age and dialysis duration Cavies comorbidity score, serum levels of IL-6, TNF, fibrinogen, albumin, lipid profile dialysis adequacy, residual renal function, or D/P creatinine. Pts who progressed were characterized with significantly higher baseline serum CRP (14.6±8.7 vs 3.26±4.2 mg/L, p<0.001), BMI (27.1±3.3 vs 22.7±3.33 kg/m2, p<0.05), and daily ultrafiltration volume (1.56±0.52 vs 1.0±0.5-9 L, p<0.05). Conclusion: This preliminary, small sample size observation providing very long-term follow-up (for >3 years) of CaSc trends indicates that, although most pts on PD are at the risk of “turning into stone.” some of these pts can still be protected against this fate. Since our study was imitated before the importance of fetuin and other regulatory proteins emerged, we were unable to further flight the possible reasons of this striking difference between the 2 groups
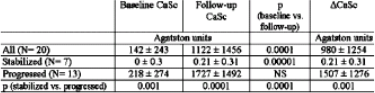
Stompor T.1, Pasowwicz M.2, Janda K.1, Krzanowski M.1, Klimeczek M.2, Konieczynska M.2, Wojcik K.1, Miarka P.1, Tracz W.2, Sulowicz W.1, PD Unit, 1 Chair & Dept of Nephrol; Dept of Cardiac & Vascular Dis.2 Jagiellonian Univ, Cracow, Poland.
Daytime Ambulatory PD for the Treatment of Refractory Congestive Heart Failure in Nonuremic Patients with Diabetic Nephropathy
Background: Volume (V) overload and refractory congestive heart failure (CHF) are common in nonuremic (non-U) patents (pts) with diabetic nephropathy ON) and are responsible for increased mortality. Current medical therapeutic strategies for refractory CHF in nor-U pts with DN are limited. Our objective in the present study was to examine the effect of using daytime ambulatory peritoneal dialysis (CAPD) on clinical outcomes of refractory CHF in non- U pts with DN. Methods: A single eerier, prospective but nonrandomized study in 24 non-U pts with DN win severe CHF refractory to drug therapy, was performed in the PD Center Dept of Nephrology, Xijing Hospital of 4th Military Medical University, between 2002 and 2004. (1) All pts (100.0%) were or state of V overload. (2) all pts (100.0%) were New York Heart Association (NYHA) class IV arid the mean left ventricular ejector fraction of all 24 pts was <40% (33.8%±5.3%). (3) mean urine V of these pts was 334±156 mL/d, arid no response to diuretics; (4) the initial MDRD glomerular filtration rate (GFR) calculated from serum creatinine was 19.25±4.3 mL/min. The mean age of these pts was 63.8±10.2 years. Initially, most pts received continuous ultrafiltration (UF) by continuous venovenous hemofiltration (CVVH) or automated PD (AFD) was started after implantation of a Tenckhoff catheter. When the symptoms of heart failure in pts were alleviated, they were convenes to DAPD regimen of 1-3 exchanges per 24 hr according to their individual reeds Dialysate containing 132 mmol/L Na and 1.5% or 25% glucose concentration (Dianeal; Baxter Healthcare, Guangzhou, China) was used in all the pts Meanwhile the salt and water intake were restricted. During the follow-up period body weights, mean arterial pressure (MAP), urine V, UF-V, cardiothoracic ratio, total (PD and renal) weekly Kt/V urea, residual renal function (GFR), heart function parameters (LVEF) were evaluated periodically. Total follow-up time: B-24 months Results. Clinical improvement was observed in all the pts. (1) Mean UF-V was 719±429 mL/d, and was kept stable during follow-up period. Mean urine V increased from 334±156 to 535±268 mL/d (p<0.05). The V of fluid intake recued from 1486.67±334.79 to 1107.73±400.13 mL/d (p<0.01). Weight decreased from 70.32±10.74 kg to 58.64±8.52 kg (p<0.01), and 79.16% (19) pts keep cry weight stable MAP arid cardiothoracic ratio of pts were sharply decreased compared to those taken before treatment. Use of ant hypertensive agents was also reduced. (2) NYHA class and LVEF: the cardiac function of all pts improved significantly; with a reduction of mean NYHA class of more than 2 graces at 3 months to 1 year follow-up LVEF increased significantly (p<0.06) at 3 months to 1 year follow-up. (3) Compared with the year before DAPD was initiated the number of CHF hospitalizations during follow-up was reduced from 5.2 to 0.4 (p<0.005). (4) At the end of the follow-up, 12 pts remained on DAPD and 10 pts converted to CAPD in order to achieve dialysis adequacy because their residual renal functions (GFR) were reduced. Two pts withdrew dialysis financial reasons. Conclusion This study showed that DAPD is a safe, feasible and effective therapy for non-U pts suffering from V overload and refractory CHF, but it needs further evaluation in carefully designed, prospective, randomized clinical trials. DAPD has the potential for offer ng another important therapeutic option for non-U pts with refractory CHF.
Sun S., Chen W., Jing M.F., Department of Nephrology, Xijing Hospital, Fourth Military Medical University, Xian, China.
Morbidity and Mortality Rates and Causes in CAPD versus Hemodialysis and Predialysis Patients
Renal transplantation represents the election method of renal substitution in ESRD, but is limited by the low number of donors. Objectives. The aim of the study is to establish the morbidity and mortality rates and causes in CAPD vs hemodialysis (HD) and predialysis patients. Material and Methods. 432 patients (236 males, mean age 47.4 years, Cl creatinine <15 mL/min) were random zed in 3 groups CAPD (n=93), HD (n=202), and pre- dialysis (n=137) The mean period of follow-up was 11.6 months (1-119) Results Renal transplantation rate was 8.3%, year (36/432 patients) 35 patients (81%) died death rate being significantly lower in CAPD (2.1% vs 15.3% in predialysis and 5.9% in HD, p<0.05). Death causes in CAPD were sepsis 1.0% and cancer 1%. Morbidity rates were 84.9% in CAPD, 73.8% in HD and 81.0% in predialysis, without statistical significance (p>0.05). The main morbidity causes were arterial hypertension, significantly high in predialysis (80.3% vs 64.5% in CAPD and 61.4% in HD, p<0.05) and infections, more frequent in CAPD or HD due to catheter's presence (33.3% in CAPD and 21.3% in HD vs 7.6%, p<0.05). Other morbidity causes were angina, arrhythmia, and cardiac failure, more frequent in dialyzed patients due to electrolytes disturbances and hemodynamic changes (15% in CAPD and 19.2% in HD vs 5.6% in predialysis. p<0.05) Chronic liver diseases are more frequent in dialyzed patients, due to nosocomial transmission in HD and preferential allocation of HBV and HCV infected patients on CAPD (4.2% in ESRD patients vs 10.9% in HD patients and 20.4% in CAPD patients). Conclusions The mortality rate in CAPD patients is significant lower than in HD or nondialyzed patients. Morbidity rate is high in ESRD patents, over 70%, without significant difference between CAPD and HD. Arterial hypertension and infections are the main morbidity causes in CAPD patients.
Voiculescu M., Ionescu C.A., Ismail G., Dimulescu R., Dimulescu T., Zilisteanu D., Rosu M., Fundeni Clinical Institute, Bucharest, Romania.
Abstract withdrawn
Novel Compounds for Reducing Oxidative and Carbonyl Stress in Peritoneal Dialysis Patients
Oxidative and carbonyl stress have been implicated in the development of atherosclerosis and increased cardiovascular mortality in dialysis patients. In addition, excessive reactive oxidants and carbonyl compounds are thought to accelerate the decline of residual renal function, and alter peritoneal membrane resulting in progressive loss of ultrafiltration for peritoneal dialysis (PD) patients. We hypothesize that PD solution containing compounds with antioxidant and carbonyl-trapping properties may reduce the risk of cardiovascular mortality attenuate the decline of residual renal function, and better preserve peritoneal membrane function. We designed and synthesized several novel analogues of vitamin E, a widely studied antioxidant in both general population and dialysis patents Vitamin E was chemically modified to impart carbonyl-trapping property In addition to their efficient binding of reactive carbonyls, a property lacked in vitamin E, the free radical binding or antioxidant capacity was enhanced by as much as 70% as a result of the chemical structure modification. Carbonyl-trapping and anti-AGE capacities were found to be greater than that of aminoguanidine, a widely investigated anti-AGE compound In a peripheral human blood mononuclear cell assay, those novel compounds were found to inhibit LPS stimulated release of inflammatory cytokines Our investigation demonstrates that vitamin E can be chemically modified to enhance antioxidant activity, and to impart carbonyl binding and anti-inflammatory properties.
Wang R.1, Hai T.2, Jiang C.2, Melnick B.2, Nordhaus M.2, Sanders P.2, Karoor S.1, Skoufos L.1, Lamela J.1, Martis L.1, Baxter Healthcare,1 McGaw Park. Baxter Healthcare,2 Round Lake, IL, U.S.A.
Hypotonia in Patients with Chronic Renal Failure Treated by CAPD
In this report we describe the possible causes of hypotonia in chronic renal failure patents (pts) treated by CAPD Hypotonia is defined as systole blood pressure (SBP) constantly below 100 mmHg. We excluded hypovolemia and antihypertensive medication as causes of hypotonia in our pts. Echocardographic examination, 24-hour BP, and 24-hour ECG (Holter ECG) monitoring was performed in 30 pts treated by CAPO for the last 5 years. 7 (23%) pts were hypotensive and 23 (77%) non-hypotensive We found the fallowing possible causes of hypotonia: heart failure (HF) (4 pts), chronic infection (2 pts), and amikacin administration (1 pt). HF was presumed to cause hypotension if pt had a clinical features of congestive HF, ejection fraction (EF) was <40%, and no evidence of fluid overload was present. Hypotension was due to chronic inflammation if pt had clinical and laboratory evidence of septicemia, i.e. positive blood culture and CRP >50 mg/L with present site of infection. Hypotension was attributed to aminoglycosides treatment when BP significantly decreased after antibiotic administration and returned to previous range after withdrawal of the drug In 4 (13.3%) pts we found systolic/diastolic dysfunction with EF ≤40%, IVRT <90 ms, and E/A<1. Mean SBP was <100 mmHg and diastolic BP (DBP) was <65 mmHg. All 4 pts had clinical signs of HF and 2 of them died. In 2 (6.7%) pts serum level of CRP was >400 mg/L during at least 6 months. One of them had a chronic inflammatory process in AV shunt and the second one had recurring positive blood cultures (Staphylococcus aureus) due to infected ventriculoatrial shunt valve. In these 2 pts mean SBP was <90 mmHg and DBP was <60 mmHg. Both pts died. In 1 pt hypotonia developed after amikacin administration. Aminoglycosides show affinity to the calcium receptor (CaR). Parathyroid glands synthesize the parathyroid hypertension agent (PHF) responsible for hypertension. Aminoglycosides induce hypotonia by activation of CaR with successive decrease in PHF secretion. Halter ECG showed signs of overactivity of sympathetic nervous system in all 7 described pts with hypotonia Autonomic neuropathy could be an additonal cause of hypotonia in these pts. We conclude that hypotonia is common in CAPD pts. Hypotensive pts have higher mortality rate (57%) than non-hypotensive patents (17%).
Wanic-Kossowska M., Kobelski M., Koziol L., Czekalski S., Department of Nephrology, Transplantology and Internal Diseases Poznan University of Medical Sciences, Poznan, Poland.
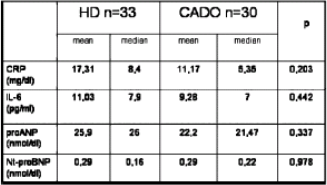
The Distribution of Nontraditional Cardiovascular Risk Factors in Elderly and Diabetic ESRD Patients in Relation to Dialysis Modality (PD versus HD)
Elderly and diabetics are the groups of the highest cardiovascular (CV) complicated risk during maintenance dialysis. The aim of the study was to compare the occurrence of nontraditional CV risk factor in elderly and diabetics treated by peritoneal dialysis (PD) and hemodialysis (HD). The study group encompassed 63 patients, 30 treated by PD and 33 by HD. PD group included 15 patients above 75 years and 15 diabetics with Mecklenburg type of Intravascular calcifications. In HD group were 17 patients above 75 years and 16 diabetics with Mecklenburg type of intravascular calcifications. The clinical characteristics of both group were not different. CRP, IL-6, proANP, Nt-proBNP serum levels were measured as associated with renal failure CV risk factors. The results are shown in Table 1. Considering the CV risk factors connected with intensity of inflammation and with volume status of the patients, PD and HD should be evaluated as equally suitable methods of renal replacement therapy for elderly and diabetics.
Weyde W., Klak R., Madziarska K., Krajewska M., Kusztal M., Kopec W., Porazko T., Golebiewski T., Bartosik H., Penar J., Klinger M., Dept of Nephrology & Transplantation Medicine, Wroclaw Medical Univ, Wroclaw, Poland
Serum Cystatin C is Associated with Cardiovascular Disease in CAPD Patients
Objectives Cardiovascular disease (CVD) is the primary cause of death of peritoneal dialysis (PD) patients. Residual renal function also plays a critical role in survival of PD patients. Recently, cystatin C (Cyst) has been found to be a serum marker of renal function. Our work investigated the relationship between Cyst and the development of CVD in CAPD patients.
Methods: Our study included 52 patients initiating CAPD treatment since 2000. There were 27 males and 25 females whose mean age was 69.49±11.04 years. Their mean PD duration was 19±14.79 months. Serum Cyst levels were measured by ELISA. Clinical data contained patients’ serum creatinine (Scr), residual glomerular filtration rate (rGFR), urine output. Kt/V, Alb, Hb, CRP, lipids, blood pressure, and echocardiography and the history of CVD.
Results Mean Scr of 52 CAPD patients was 743.99±225.52 μmol/L, mean serum Cyst 7.03±1.45 μmol/L, and mean rGFR was 3.01±2.74 mL/in. A strong correlation was observed between serum Cyst and Sa (r=0.302, p<0.01) and rGFR (r=-0.458, p<0.01). Compared with nonanuric CAPD patients, the Cyst levels were higher in anuric patients (7.66±1.47 vs 6.59±1.31 μmol/L, p<0.05). The concentrations of serum Cyst were directly related to cholesterol and CRP, and negatively related to Kt/V. The serum Cyst levels were higher among CAPD patients with CVD than that of other patients (7.28±1.39 vs 5.84±1.12 μmol/L, p<0.01)
Conclusion: Our study suggest that Cyst is correlate with inflammation, dyslipidemia, and the adequacy of PD Serum Cyst may be a new noteworthy predictor of CVD in CAPD patients.
Wu P., Ren H., Yu H., Zhu P., Chen N., Department of Nephrology. Ruijin Hospital, Medical College of Shanghai Jiaotong University, Shanghai, China.
Serum Troponin T in Patients on CAPD
Objective: Elevated concentration of cardiac troponin T (cTnT) has been shown to be a predictive marker of poorer long-term cardiovascular outcomes in stable patients with ESRD. The aim of this investigation was to assess the significance of cTnT in patients on CAPD. Methods: The value of serum cTnT of 64 follow-up CAPD patients (mean age 52±16 years; 36 males and 28 females) with no evidence of acute coronary syndrome were detected by using the third-generation TnT assay on Elecsys 2010 (Roche, Switzerland), 15 persons as the health control. The analytical range of cTnT assay was 0.01-25.0 ng/mL. The levels of C-reactive protein. TNF-α, interleukin-6 (IL-6), cholesterol, triglyceride, albumin, ferritin, serum glucose and electrocardiogram were also measured. Results The level of serum cTnT in CAPD patents (0.08852±0.16168 ng/mL) were significant increased compared with the health control persons <0.01 ng/mL. Among these CAPD patients, 7 had a level between 0.07 and 0.10 ng/ mL, 23 had a level range from 0.03 to 0.07 ng/mL, and 18 had a level of 0.01–0.03 ng/mL. Only 4 were <0.01 ng/mL The level of cTnT had strong correlation with the level of blood glucose (r=0.53784, p<0.01) C-reactive protein (r=0.35550, p<0.01), IL-6 (r=0.10148, p<0.01), residual urine volume (r=-0.27480, p<0.05), and the period of peritoneal dialysis (r=0.34728, p<0.01). The level of cTnT in CAPD patients with ischemic heart disease (IHD) or left ventricular hypertrophy (LVH) was significantly higher than that of patients without IHD or LVH (chi-square 7.61781, p<0.01), 42% of diabetic patents had an increased cTnT which significantly higher than that of nondiabetic patients (chi-square 7.77198, p<001). AII diabetic patients with IHD or LVH had an increased cTnT Conclusions: Our study demonstrated that cTnT in patients on CAPD was elevated which can predict the cardiovascular events The CAPD patients with diabetes mellitus had a high rate of elevated cTnT which suggests these patients may have a higher cardiovascular risk The value of cTnT is also a negative indicator of residual renal function and a positive indicator of inflammation.
Yang X., Zhang Y.E., Guo Q.Y., Un J.X., Jiang Z.P., Mao H.P., Chen W., Zhang X.D., Guan J.M., Hu L.Q., Yu X.Q., Department of Nephrology, The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, China.
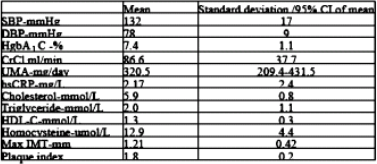
Atherosclerotic Risk Factors and Carotid Intimal-Medial Thickness/Plaque Formation in Diabetic Nephropathy: How are they Related?
Background: Atherosclerotic diseases have been shown to be correlated with carotid intimal-medial thickens (IMT) and plaque formation. Patients :pts; with diabetic nephropathy (DN) are more vulnerable to develop atherosclerotic complications. Management of a relevant atherosclerotic risk factors is therefore important treatment target. Methods 81 asymptomatic DN pts at their mean age of 58.5 years (range 36–74) were recruited. 21% received insulin, 78% oral hypoglycemic drugs, 100% antihypertensive drugs, and 98% ACEI/ARB. Carotid IMT and plaque lesion were measured by high resolution B-mode ultrasound. Atherosclerotic risk factors were assessed and compared with maximal IMT and plaque lesion by univariate and multivariate analyses Results: Demographic characteristics were tabulated On univariate analysis, plaque lesion formation (IMT>1.2 mm) was found to be related with LDL- cholesterol (r=0.24, p=0.04) and diastolic blood pressure (DBP) (r=-023, p=0.04), while maximal IMT was related with HDL-cholesterol (r=-026, p=0.03), systolic BP (SBP) (r=0.28, p=0.02), and microalbuminuria (LIMA) (r=0.31, p=001). On multivariate analysis maximal IMT is related with microalbuminuria (r=0.61, p=0.01) after adjusting for age, body mass index, BPs, glycosylated hemoglobin (HgbA1C), creatinine clearance (OrCl), hsCRP, insulin, C-peptide, lipid profiles, and homocysteine level (R2=0.36, F-value=2.84). Conclusion: BPs, cholesterol, and microallbuminuria are important independent risk factors for subclinical atherosclerosis in DN. They should be monitored and managed aggressively for atherosclerosis prevention.
Yip T.W.C.1, Chook P.2, Li J.K.Y.1, Leung A.Y.S.1, Kwan W.K.1, Szeto C.C.2, Hung V.H.F.3, Chung C.H.3, Chan A.Y.W.3, Tong M.K.L.3, Chan L.L.T.2, Chan M.H.M.2, Woo K.S.2, Yan Chai Hosp.,1 The Chinese Univ of Hong Kong,2 Princess Margaret Hosp,3 China.
Serum Adiponectin Level is Related to Inflammation but Not to Decline of Renal Function in Peritoneal Dialysis Patients
Objectives: Adiponectin (ADPN), exclusively expressed and secreted from adipocytes, is a cytokine with anti-atherogenic and anti-inflammatory properties Plasma ADPN is reduced in obesity and insulin-resistant states Reports show an elevation in the serum ADPN levels in patients with CRF or maintained on dialysis. Evidence show that in patients without obvious renal dysfunction, ADPN may inversely relate to renal function. The purpose of this study was to assess the relation of serum ADPN to residual renal function and clearance of creatinine in peritoneal dialysis patients.
Methods: The residual glomerular filtration rate, Kt/V, and creatinine clearance (Ca) of dialysate and residual renal were estimated in 59 CAPD patients followed up in our center The peritoneal equilibration test was measured in 52 of these patents. We measured the serum levels of ADPN by ELISA.
Results: Serum ADPN levels of PD patients were 2 times higher than those of healthy subjects (13.09±7.54 vs 6.65±4.33 μg/mL, p<0.01). Mean total Ccr and Kt/V values of the CAPD patients were 55.87±15.61 L/week/ 1.73 m2 and 1.83±0.35. The mean residual renal Ca, KtV, and glomerular filtration rate were 14.94±17.03 L/week/1.73 m2, 0.33±0.37, and 1.44±1.60 mL/min, respectively. By linear regression analysis serum ADPN level was not correlated with total Ccr or Kt/V. It was also not correlated with residual renal Ccr, Kt/V, or glomerular filtration rate. The serum ADPN levels were not significantly different between different peritoneal transport type [12.87±7.44 (L/LA) vs 13.68±7.63 μg/mL (H/HA),p=0.702]. The concentrations of serum ADPN were inversely related to BMI (p<0.05), triglycerides (p<0.01), CRP (p<0.05), and IL-6 (p<0.05), and were directly related to HDL (p<0.01) of the patients.
Conclusions: Serum ADPN appears mainly influenced by inflammation, body mass index, and metabolic disturbance in CAPD patients, while not affected by residual renal function or clearance of creatinine.
Yu Z.Z., Ni Z.H., Gu L.Y., Lin A.W., Fang W., Qian J.Q., Dai H.L., Cao L.O., Renal Division, Renji Hospital, Shanghai Jiaotong University, Shanghai, China