
Abstract

Modified Desferrioxamine (DFO) Test for Aluminum Overload in Continuous Ambulatory Peritoneal Dialysis (CAPD)
Aim: Standard similar test is prescribed to assess aluminum overload in hemodialysis and CAPD. Since 2 therapies differ fundamentally as 1 is intermittent and other continuous we propose a modified DFO test for CAPD patients keeping DFO pharmacokinetics in view. Aim of study is to compare results of the modified DFO test against the standard DFO test in patients with aluminum levels>60 μg/L.
Material and Methods: Patients on hemodialysis for ≥ 2 years and presently on CAPD having a baseline aluminum levels>60 μg/L were enrolled These patients had either resistant anemia, neurological disturbances, or bone disease (iPTH 50 μg/L)
Results: Four patients meeting inclusion criterion were enrolled. DFO test was negative by the standard DFO test in all 4 patients. By the modified DFO test 3 patients had positive test and 1 negative. Doubling of aluminum values was observed at 5 or 12 hours post DFO in these 3 patients A44 values in all the 4 patients were not significantly different from AO All 3 patients with positive modified DFO test were treated with DFO and symptoms of aluminum overload Improved.
Conclusion: Standard DFO test is ineffective in diagnosing aluminum overload in CAPD. Proposed modified DFO test tailored to drug kinetics and CAPD dynamics is a superior test to diagnose aluminum overload in CAPD.
Aggarwal V.D., Bahadur M.M., Mali M., Jaslok Hospital and Research Center, Mumbai, India.
FDG PET Scans in Long-Term Peritoneal Dialysis Patients May Detect an Inflammatory Phase of Encapsulating Peritoneal Sclerosis (EPS): Evidence from Dialysate MCP-1 Levels
EPS is a major complication of long-term peritoneal dialysis (PD) and is associated with considerable morbidity and mortality. In many patients (pts), there is thought to be an inflammatory phase preceding the progressive fibrosis that eventually results in peritoneal sclerosis Currently the diagnosis is made late either clinically with bowel obstruction or on CT scan with evidence of bowel wall thickening or peritoneal calcification. An earlier diagnosis at the time of inflammatory phase may enable appropriate treatment and thereby prevent the onset of fibrosis. As part of our prospective PD study, we have used 2 techniques to screen long-term PD pts for peritoneal inflammation: FDG PET scanning, which is commonly used to detect metabolic tumor activity, and dialysate MCP-1 level obtained during a standard peritoneal equilibration test (PET). We have previously shown that dialysate MCP-1 is associated with ongoing peritoneal inflammation and ultrafiltration failure (ASN Abstract 2004). FDG PET scans were done in 15 long-term PD pts with mean duration of PD 6.26±0.53 years: 6 were positive for peritoneal inflammation and 9 were negative. CT scans have been done in the 6 pts with positive scans: 4 had changes suggestive of EPS and 2 were normal Dialysate MCP-1 levels were higher in pts with positive scans (mean 259.4±68.28 vs 137.7±28.18 pg/mL, p=0.087). These results suggest that FDG PET scans may be useful in making an earlier diagnosis of EPS, by detecting an inflammatory phase. Such scans, however, are expensive and are not uniformly available. Larger numbers of pts are needed to determine whether the scan results correlate with levels of MCP-1 or other inflammatory cytokines in the dialysate.
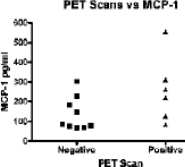
Ahmad S.1, Frank J.W.2, Tam F.W.K.1, Brown E.A.1, West London Renal and Transplant Center,1 Imperial College London: Department of Nuclear Medicine,2 Charing Cross Hospital London, United Kingdom.
Relevance of Mast Cells to Peritoneal Injury Induced by Peritoneal Dialysis
Objectives: Peritoneal sclerosis is the major complication of peritoneal dialysis (PD) Mast cells were shown to be actively involved in renal fibrosis. They can produce factors such as tryptase, chymase, and base fibroblast growth factor that might contribute to neoangiogenesis. This study aimed to establish the possible role of mast cells in peritoneal sclerosis in the setting of PD. Neovascularization, in the peritoneum as a part of the fibrotic process and its relation to fibrosis, was also investigated. Methods: This study comprised 54 nonuremic male Wistar rats divided into 2 groups injected with test solutions intraperitoneally on daily toasts and a control group. Test solutions included peritoneal effluent (from human patients) and dextrose Six rats were sacrificed at monthly intervals Specimens of the peritoneum were harvested The expression of trichrome, collagen III, alpha-smooth muscle actin (α-SMA), vascular endothelial growth factor (VEGF), and mast cells (using mast cell tryptase) were quantified immunohistochemically Results: Morphological changes of the peritoneum included cubic transformation of mesothelial cells with increased fibrous tissue depositor. Mast cells accumulated in the submesothelial layer and in between muscle fibers. A statistically significant increase in their number was detected in the third month in both test groups compared to controls (3.86±0.386 & 3.66±0.38 respectively vs 0.1±0.01, p=0.001). Collagen III, α-SMA, and VEGF also showed a statistically increased level of expression in both test groups in comparison to controls (p=0.001, p=0.01, p=0.001). A significant correlation was observed between the expression of trichrome, VEGF, α-SMA, collagen III, and the number of mast cells in both study groups compared to controls (r=0.809, p=0.008; r=0.794, p=0.01; r=0.829, p=0.006; r=0.804, p=0.009 respectively in group 1, and r=0.904, p=0.001; r=0.909, p=0.001, r=0.934, p=0.001; r=0.896, p=0.001 respectively in group 2). Conclusion: Mast cells accumulated in the peritoneum upon exposure to PD fluid Their actual role in peritoneal fibrosis might be due to the induction of angiogenesis during PD. However, this needs further investigation.
Allam N.A.A.1, Baddour N.M.2, El-eter E.A.2, Naga S.S.2, Naga Y.S.2, Menofeya University,1 Shebeen: Alexandria University,2 Alexandria, Egypt.
Tamoxifen Treatment for Peritoneal Fibrosing Syndromes: Comparison to a Non-Treated Historical Series
Encapsulating peritoneal sclerosis is a serious complication of peritoneal dialysis (PD) with a high mortality rate. Early diagnosis is mandatory in order to avoid its fatal consequences. Tamoxifen is an anti-estrogen drug that has been shown to be useful in the treatment of other fibrosing diseases The purpose of this study is to evaluate the effect of tamoxifen for sclerosing peritonitis (SP) treatment. We included all our patients diagnosed of SP. To compare the outcome of patients treated or not with tamoxifen we established 2 groups: 14 patients treated with tamoxifen (20 mg/12h) (TG) for 15.5±6.8 months, and another 15 patients with SP who received no treatment (CG). There were no significant deference's between both groups for age, accumulated days of inflammation activity, incidence of peritonitis and hemoperitoneum, days of active inflammation during the last episode values of peritoneal transport for small solutes and ultrafiltration capacity at baseline and time on PD (60.6±32 in CG vs 64.1±43 months, in TG). Complications related to SP were less frequent in TG than in controls (p=0.004). One patient treated with tamoxifen and 6 patients from CG developed encapsulating SP (p=0.039) 13 patients form CG and 6 from TG died during the follow-up (p=0.013). Causes of death were related to SP in 6 patients in CG and 1 in TG (p=0.039). All these complications appeared before 6 months of follow-up in the control group. Survival analysis demonstrated that mortality related to SP was significantly higher in patents not treated with tamoxifen (p=0.038). Overall mortality was also significantly higher in control group at the first year (p=0.01).
In conclusion, our experience suggests that the treatment with tamoxifen of patients diagnosed of SP may be beneficial and should be considered. It diminishes the complications related to SP and significantly decreases mortality.
Bajo M.A., Del Peso G., Castro M.J., Sanchez-Villanueva R., Gonzalez E., Romero S., Olivas E., Selgas R., Hospital Universitario La Paz, Madrid, Spain.
Evaluation of Salivary pH, Buffering Capacity, and DMFT Index Values in Peritoneal Dialysis Patients
Objectives: Oral and dental problems of peritoneal dialysis (PD) patients are important in respect to potential infections. Saliva has antibacterial, antiviral, and antifungal activities. Salivary buffering capacity (SBC) is an important parameter for decreasing the risk of decayed teeth by maintaining optimal salivary pH (SpH). The decayed (D), missing (M), and filled (F) teeth index (DMFT) has been developed to determine the oral and dental health status. Our aim was to analyze and compare SpH, SBC, and DMFT index values of CRF patients receiving PD to healthy controls (C).
Method: 76 PD (33 M, 43 F; mean age 44±12 years), 111 C (46 M, 65 F; mean age 45±18 years) were included in the study. SpH was measured immediately after collecting stimulated whole saliva using Merck indicator (Universal indicator, pH 0-14 Merck, Darmstadt, Germany), whereas SBC was measured according to the method of Ericsson; 1 mL of whole saliva was transferred to 3 mL of 0.005N HCl and a stream of air was passed through this mixture for 20 min before the determination of SBC. Student t-test was used for statistical analysis of SpH and SBC. Mann Whitney U test was used to compare DMFT index values.
Results: No statistical differences were found for age and gender distribution in PD and C groups (p>0.05) In the PD group mean SpH (8.35±0.43), SBC (7.40±0.47), and number of filled teeth (4.47±5.90) were significantly higher than the means in C group (7.16±0.76, 5.08±0.73, 1.57±2.58, respectively; p<0.001).
Conclusions: In spite of high SpH and SBC values in PD patients, an increased number of filled teeth and no reduction in DMFT values have been found. Thus, more care should be taken in maintaining optimal oral hygiene in this patient group. PD patients should also regularly go to dental examinations for fluoride applications and necessary restorative treatments to be done.
Bayraktar G.1, Kurtulus I.2, Kazancioglu R.3, Yildiz A.4, Cintan S.2, Bozfakioglu S.4, Besler M.5, Trablus S.5, Depts of Removable Prosthodontics1 & Periodontal,2 Faculty of Dentistry. Istanbul Univ: Dept of Nephrol,3 Haseki Training & Res Hosp: Dept of Nephrol,4 Faculty of Med, Istanbul Univ; Dept of Nephrol,5 Istanbul Tearing & Res Hosp, Istanbul, Turkey.
Xerostomia in Patients Undergoing Peritoneal Dialysis
Objective: Saliva plays an important protective role in defending the oral cavity. In addition to preventing oral tissues from dehydration, it also has functions like mechanical cleaning of food and microbial debris. Decrease in salivary flow rate (SFR) can be the cause of symptoms like xerostomia, atrophic appearance of the mucosa, as well as change in the microbial flora. Hence, SFR is an important salivary parameter affecting the health of oral and surrounding tissues It is the aim of our study to evaluate and compare SFR of chronic renal failure (CRF) patients receiving peritoneal dialysis (PD) to healthy controls
Methods: 75 PD (PD group: 33 male, 42 female; mean age 44±12 years). 50 healthy controls [control (C) group. 24 male, 26 female: mean age 46±15 years] were included in the study. Stimulated whole saliva was collected at 09.30-11.00 am in the PD and C groups For pre-stimulation, standard weight (∼1 g) paraffin wax was chewed for 60 seconds intensively and cumulated saliva was swallowed first Thereafter, while chewing on the same paraffin was continued, saliva was spit into sterile aliquots during the next 5 minutes Stimulated SFR was expressed as mL/min. Statistical analysis was performed using Student t-test.
Results: No statistically significant differences between the age and gender of title PD and C groups were found (p>0.05). The mean SFR in the PD group (1.30±0.83 mL/min) was found statistically less than that of the C group (1.64±0.45 mL/min) (p<0.001).
Conclusion: CRF patients receiving PD have been found to have lower SFR than healthy controls. Thus, it is of great importance to keep these patients under regular dental control, to measure SFR regularly and prescribe saliva substitutes or mouth rinses without alcohol, recommending chewing gums without sugar in cases where it is necessary, in order to be able to maintain optimal oral health and prevent xerostomia in this patient group.
Bayraktar G.1, Kurtulus I.2, Kazancioglu R.3, Yildiz A.4, Cintan S.2, Bozfakioglu S.4, Bester M.5, Trablus S.5, Depts of Removable Prosthodontics1 & Periodontol,2 Faculty of Dentistry, Istanbul Univ; Dept of Nephrol,3 Haseki Training & Res Hosp; Dept of Nephrol,4 Faculty of Med, Istanbul Univ; Dept of Nephrol,5 Istanbul Training & Res Hosp, Istanbul, Turkey.
Guidelines for Withdrawal from Chronic Dialysis
In 2033 the prevalence of patients (pts) on renal replacement therapy was 794 in South Korea, 946 in Germany, 1509 in the U.S.A., 1631 in Taiwan, and 1797 per million inhabitants in Japan. Advanced age and acceptance of polymorbidity at the start of dialysis as well as large socioeconomic, cultural, and religious differences in attitude of the pts to dialysis and transplantation are the man reasons for the wide range of this prevalence Between 1994 and 1995 the withdrawal from dialysis was 0.7% in Japan 1.6% in Germany, and 5.1% in the U.S.A. The Ethical commission of the Berlin Chamber of Physicians has worked out guidelines from withdrawal of dialysis which are in many respect universal. Guidelines: (1) Life-sustaining procedures are intensive care medical treatments (2) Artificial enteral and parenteral nutrition are medical care. (3) The essential basis for the medical decision is the will of the pt (4) The pt has the right to disagree with the treatment even if it is a life-sustaining one. (5) Before the withdrawal, the pt and in case of incompetence or unconsciousness of the pt, the legal surrogate must be informed completely. (6) If there is an obvious discrepancy between the wish not to be treated and the pt's sickness, then the physician should involve a psychiatrist in order to clarify whether the disagreement is a symptom of a psychiatric disease (7) If the pt is near to death, then the prolongation of life through intensifying the treatment would prolong suffering and could hurt individual dignity. The physician should stop the intensive care, such as dialysis. (8) If the pt s mentally incompetent or unconscious the physician has to find out the pt's presumed will. If there is no written advance directive and legal surrogate resp., then the physician has to stop the treatment in case of an infaust prognosis. (9) The physician must follow the written advance directive But if there are signs that the patient has changed his will which is written in his advance directive or the situation has changed so that his written advance directive no longer matches the original written advance directive the physician must follow the actual will of the pt (10) If a person has the power of attorney for health care, that person {surrogate} has the power to decide for the mentally incompetent or unconscious pt due to the written advance directive. If there is no written advance directive, the surrogate and the physician have to explore the pt's presumed will. (11) If the physician wants to star, or to continue the life-sustaining treatment but the surrogate does not want the continuation of the treatment then that person has to get further consent by court The physician continues the treatment until the decision of the court is made. If the court decides in agreement with the physician the surrogate has to accept the physician's decision. (12) The physician decides in agreement with the surrogate to stop the treatment because of the infaust prognosis then there is no need for a consent by the court. The court decides only if there is a conflict situation. (13) If the physician wants to stop the life-sustaining treatment, but the surrogate wants continuation of the treatment then the physician has the right to stop the treatment on pts with infaust prognosis without involvement of the court. (14) The physician has the medical tradition to uphold in not harm ng the patient. Prolonging the dying process proceeding only for scientific reasons or performing for possible monetary compensation are illegal medical procedures. (15) During the process of dying, the respecting pts dignity is of supreme importance. Even if life-sustaining procedures are withdrawn, the physician must assist me pt if there is any suffering such as pair or shortness of breath. The nursing care must be continued until the pt's death.
Becker H.P.1, Matthies R.2, Hennes G.3, Fischer H.C.1, Kuratorium for Dialysis,1 Ethical Commission Berlin,2 Social Court Berlin,3 Berlin, Germany.
Daytime Sleepiness and Quality of Life in Automated Peritoneal Dialysis and Continuous Ambulatory Peritoneal Dialysis (CAPD) Patients
The goals for dialysis therapy are to reduce morbidity, improve survival and quality of life (QOL). Automated peritoneal dialysis (APD) is a preferred dialysis therapy as it offers better flexibility during daytime. However APD procedure continues throughout the night so it may cause sleep disorders and daytime sleepiness. In this study we aimed to compare APD and CAPD therapies for excessive daytime sleepiness and QOL. This cross-sectional study included 59 PD patents (CAPD/APD 30/29, M/F 33/26, age 45±15 years, PD duration 42.0±33.6 months). Epworth Sleepiness Scale (ESS) was used. ESS scores higher than 9 were accepted as excessive daytime sleepiness. QOL parameters were assessed by the self-administered short-form SF-36 generic health survey questionnaire Concurrently, possible risk factors for sleep disturbance (demographic variables, personality traits, comorbid diseases, clinical and laboratory parameters) were analyzed. CAPD and APD groups were similar regarding the factors that affected sleep quality (age, gender, PD duration, smoking and alcohol intake, socioeconomic status, body mass index, and presence of comorbid disease, and various laboratory parameters) (p>0.05 for all). Although 1 (3.3%) patient in CAPD and 4 (13.8%) in APD had excessive daytime sleepiness, there was no significant difference between CAPD and APD in terms of ESS scores (3.9±2.5 vs 4.6±4.2, p>0.05). Also no significant difference was present in total QOL and subscale scores in CAPD and APD patients (p>0.05). A Pearson bivariate correlation analysis revealed that ESS scores were negatively correlated with total QOL (-0.291, p=0.04), social functioning (-0.384, p=0.004), and role-emotional subscale (-0.344, p=0.009) scores. Although the incidence of excessive daytime sleepiness is slightly higher in APD patients due to the nighttime dwells, it does not reach significant levels As a result. APD can be preferred PD modality as it does not have negative impact on daily activities and QOL by increasing daytime sleepiness.
Bilgic A.1, Akman B.1, Sezer S.1, Ruya O.1, Arat Z.1, Ozdemir F.N.1, Haberal M.2, Department of Nephrology1 and Department of General Surgery,2 Baskent University Faculty of Medicine, Ankara, Turkey.
In Vitro Capillary Tube Formation is Enhanced by Mesothelial Cell VEGF Secretion after RAGE Activation
Background: Peritoneal dialysis fluids (PDFs) have been shown to induce peritoneal neoangiogenesis. Glucose, glucose degradation products (GDPs), and advanced glycation end products (AGEs) are considered to to possible triggers, so we investigated whether they could modify the vascular endothelial growth factor (VEGF) production by human peritoneal mesothelial cells (HPMCs) and the capacity of human umbilical vein endothelial cells (HUVECs) to form capillary tubes Methods: AGE and VEGF concentrations in PD effluents of 5 nondiabetic patients were determined after short and long dwell. VEGF production by HPMCs exposed to different glucose concentrations, 3 deoxyglucosone (3-DG) or carboxymethyllysine-albumin (CML albumin) a high affinity receptor of AGE (RAGE) ligand was determined in vitro. HUVEC capacity to form capillary tubes was evaluated in Matrigel (3 dimensions) in a co-culture system after HPMC stimulation by CML-albumin. Some blockade experiments were performed using anti-RAGE or anti-VEGF antibodies Endothelial cell VEGF receptor (VEGFR-1 and -2) expression was measured by ELISA. Results: Compared to short dwell, AGE and VEGF concentrators in PD effluents were significantly released during long dwell In vitro, CML-albumin increased VEGF production by HPMCs (p<0.001) HUVEC capacity to form capillary tubes was enhanced when co-culture was performed with HPMCs stimulated by CML-albumin. Pre-incubation of HPMCs with an anti-RAGE or addition of anti-VEGF antibody in culture medium reversed this effect (<0.001) indicating RAGE involvement in the stimulation of HPMCs. Endothelial cell VEGFR-1 was enhanced by CML-albumin in HUVECs Conclusion: In a co-culture system, we demonstrated that VEGF production by HPMCs favors capillary tube formation through a mesothelial RAGE activation. VEGF modulation could well be considered as a new target in the prevention of neoangiogenesis and ultrafiltration failure in PD patients.
Boulanger E.1, Grossin N.2, Wautier M.P.3, Taamma R.4, Wautier J.L.2, Clinique de Nephrol,1 Centre Hosp Regional Univ, Lille; Instit Nat'l de la Transfusion Sanguine,2 Inserm U665,3 Paris: Fresenius Medical Care,4 Fresnes, France
Making Peritoneal Dialysis Equipment Conversion Fun
Purpose: To convert peritoneal dialysis (PD) patients (pts) from one product to another with the least amount of stress to the pts and staff. Methods We initially worked with our FMC-NA clinical sales specialist (CSS) to get an action plan in place for each clinic. We made sure all staff was trained on the new FMC-NA stay safe® PD systems. This was achieved through educational classes and in-services. The local hospitals were trained in the use of stay safe adapters With all staff trained, we moved forward with conversion candidate selection and training all new pts on the stay safe systems. We chose not to convert pts with terminal illness, mental confusion, or pending living-related donor transplant. We sent letters to selected pts notifying them of planned changes and inviting them to a product fair Pts were allowed to see and touch the new products and ask questions about the process. They were given schedules allowing 2-8 weeks to make their plans Pts were scheduled in small groups with commonalities within the group. With the schedule in place we had a conference call with the FMC Customer Service New Patient Team, and training kits were ordered for the pts. Individualized prescriptions were subsequently sent in. We allowed 2-3 days of training for each group. CCPD pts were also trained for back-up CAPD. We used the Newton IQcard™ for the cyclers which decreased the amount of training time needed for prescription programming. We utilized videos, lecture, demonstrations, word searches, check-off demonstrations, and post-tests in the training process We made home visits to pts having any difficulty with the cycler. A CSS was on call every day of the process for pt and staff support. We took 5 months to complete the process. Results: Our 4 clinics converted or trained more than 53 pts and had fun doing it. Conclusion: Our success proves that following the FMC-NA conversion plan allows your clinic to convert your pts in a fun, low-stress atmosphere.
Bridger S.H.1, Davis B.2, Austin K.3, Smith S.4, Huckaby S.6, RCG.1 Memphis; RCG,2 Germantown TN; RCG,3 Southaven. MS; RCG,4 Marion, AK; FMC-NA5; U.S.A.
Growing Peritoneal Dialysis: Removing the Bias toward Hemodialysis
Background: Peritoneal dialysis (PD) is widely recognized as an established form of renal replacement therapy (RRT) Over the past decade, several studies have compared the outcomes of PD vs hemodialysis (HD) and despite some conflicting reports, no major differences in patient (pt) survival has been observed. (Gokal et al., 1999; Nissenson et al., 1993). As center dialysis units reach capacity. PD, the less expensive dialysis modality is increasingly becoming the option of choice for Canadian hospitals. Data from the Canadian Organ Replacement Register indicates a 9% increase in dialysis-dependent pts in Canada between 1998 and 2001 (CIHI 2003). Since 2002 St. Michael's Hospital has experienced a 15% growth in in-center and home HD incident pts. While St Michael's is experiencing an unprecedented growth in pts choosing the HD modality, the numbers of home PD pts have tended to remain constant at 45 pts. This represents only 16% of the total pt numbers receiving dialysis at St. Michael's Hospital. Objective: This presentation describes the process/challenges of growing PD in a hospital which offers modality choices to pts, and which has historically had a strong bias toward HD. Method: A collaboration of senior management, physicians, and industry partnership was established with the goal of growing RD to 30% of the dialysis population at St. Michael's Hospital over a 2-year period. An additional nurse was hired to repatriate new starts on HD to PD along with enhanced PD education to pts in the predialysis clinic and in the failing transplant clinic Results: Within a 3-month period, 5 new pts started on PD, representing an 11% increase in the PD population. The PD program has experienced a few setbacks with human resources but patient numbers continue to grow steadily related to the increased and positive medical and nursing encouragement of PD Conclusions PD is a viable and cost effective modality choice for pts. As bias toward HD are removed, more and more pts will choose PD, decreasing costs to the health care system, while providing an effective form of RRT.
Campbell J., Kashani M., St. Michael's Hospital, Toronto, Canada
Spontaneous Hemoperitoneum Complicating Two Patients on Continuous Ambulatory Peritoneal Dialysis (CAPD)
Hemoperitoneum is an infrequent complication in patients on CAPD, and most of the time benign in outcome. We report 2 cases of spontaneous hemoperitoneum in 2 end-stage renal disease (ESRD) patients treated with CAPD. Both patients were diagnosed to have ESRD not due to polycystic kidney disease, started on CAPD for more than 5 years Both patients were hypertensive requiring medication for control They presented with blood-stained effluent dialysate and right-sided abdominal pain, without history of injuries before onset of symptoms Laboratory investigation confirmed significant drop in hemoglobin level when compared to baseline in both patients. Computerized tomography confirmed acute perinephric hematoma with extension to retroperitoneal space together with multiple renal cysts, therefore suggesting the background of acquired cystic kidney disease (ACKD) There were no active extravasations of contrast intra-abdominally to suggest bleeding sources other than the native kidneys, nor radiological features to suggest intra-abdominal malignancies Both patients underwent urgent angiographic examination and were treated successfully with selective embolization of corresponding renal arteries. One patient stayed in peritoneal dialysis immediately after the hemoperitoneum without farther drop in hemoglobin, whereas the other patient was transferred to temporary hemodialysis, in view of extensive retroperitoneal hemorrhage.
These 2 cases best illustrate this potentially fatal complication in patients with ACKD, which develop with time in dialysis. Radiological investigations such as computerized tomography may play an important role in diagnosing this condition, and may be useful to screen for dialysis patients at risk.
Chan C.K., Lo S.H.K., Wong C.K., Chow V.C.C., Mo K.L., Wong K.S., Pamela Youde Nethersole Eastern Hospital, Hong Kong, China.
The Validity of a New Practical Quality of Life Measure in Thai Patients on Renal Replacement Therapy
Objective: A 9-item Thai health status assessment instrument (9-THAI) was developed as a part of the Thai National Health and Welfare 2003 survey. The measure is a promising tool for outcome evaluation of clinical practice due to its brevity, validity, reliability and availability of Thai general population norm-based scores. To assess validity of the 9-THAI in patients receding renal replacement therapy (RRT).
Methods: Patients on RRT who attended Srinagarind hospital during March to May 2005 were interviewed. Convergent and divergent validity were assessed using the SF-36 as the concurrent measure. Concurrent validity was also assessed using hematocrit level and hospitalization history in the last year as concurrent clinical measures.
Results: 302 patients were interviewed; they were on HD (107), CAPD (62) or KT (133). The correlation between 9-THAI and SF-36 domains were as hypothesized with values of 0.37 to 0.77 for convergent validity, and lower values for divergent validity. The 9-THAI mental scores were significantly correlated with hematocrit level, as an increment of I % in hematocrit level associated with an increment of 0.05 unit in the 9-THAI mental score (p=0.028) The 9-THAI physical scores were significantly associated with a decrease likelihood of being hospitalization (adjusted OR=0.98, p=0.001). The results confirmed the validity of 9-THAI in these patients.
Conclusion: The 9-THAI is a valid generic health status measure that can be used as an ideal core in a battery of quality of life measures in clinical practice for Thai patients on RRT.
Cheawchanwattana A.1, Limwattananon C.1, Gross C.2, Limwattananon S.1, Tangcharoensathien V.3, Pongskull C.4, Sirivongs D.4, Faculty of Pharmaceutical Sci,1 Khon Kaen Univ, Khon Kaen, Thailand; Coll of Pharmacy,2 Univ of Minnesota, Minneapolis U.S.A.; Internal Health Policy Prog,3 Ministry of Public Health; Faculty of Med,4 Khon Kaen Univ Khon Kaen, Thailand.
Oxidative Stress and Mitochondrial DNA Copy Number Alteration in Peritoneal Dialysis Patients
Objective: The role of oxidative stress in the regulation of the copy number of mitochondrial DNA (mtDNA) in leukocytes is unclear. In this study, we investigated the redox factors in plasma that may contribute to the alternation of mtDNA copy number in CAPD patients.
Methods: A total of 91 CAPD patients (mean age 43.5 years, 22 males. 69 females) and 99 healthy subjects (mean age 44.8 years. 45 males 54 females) were enrolled. Plasma free thiols and indicator of lipid peroxidation, thiobarbituric add reactive substances (TEARS) in plasma were measured. The mtDNA copy numbers in leukocytes were determined by real-time PCR. Blood levels of sugar, cholesterol, triglyceride were also measured
Results: There were significant differences between CAPD and control groups in plasma thiols (1.24±0.32 vs 1.66±0.85 μmol/L, p<0.001) and TBARS (1.61±0.51 vs 1.2±10.54 μmoL/L, p<0.001) levels. The mtDNA copy numbers in leukocytes were 8.03±2.85 in CAPD patients, 6.56±4.28 in healthy subjects (p=0.006) The blood levels of sugar (99.95±39.23 vs 98.34±10.80 mg/dL) and cholesterol (201.54±35.75 vs 197.54±36.48 mg/dL) were not different between 2 groups, but triglyceride levels were higher in CAPD patents (167.93±133.50 vs 114.96±66.67 mg/dL).
Conclusion: The copy number of mtDNA in leukocytes in CAPD patients is affected by oxidative stress elicited by the alteration of plasma antioxidants/pro-oxidants.
Chen J.B., Liao S.C., Hsu K.T., Lee C.T., Lee C.H., Lam K.K., Chuang ER., Chang Gung Memorial Hospital, Kaohsiung, Taiwan
Benefits of Pre-ESRD Education in CAPD
Due to the fact that the majority of patients (pts) with CKD have a lack of knowledge about their conditions. The education of pts with pre end-stage renal disease (ESRD) focuses on the inevitability of reaching ESRD and requiring renal replacement therapy (RRT) are desperately needed. The overall goals of the pre-ESRD program include: giving available treatment options; making early choice of dialysis modality and preparation and increasing peritoneal dialysis (PD) option by education; timely initiation of RRT. We conducted a retrospective review of 172 pts who reached ESRD and initiated dialysis therapy at Chang Hua Christian Hospital from January 2002 to December 2002. Result 109 pts did not receive pre-ESRD education. 63 pts received pre-ESRD education. 20 of 63 (31.8%) pts received pre-ESRD education initiated PD, 17 pts (27%) initiated PD timely. 31(28.4%) of 109 pts without receiving pre-ESRD education chose PD for maintaining therapy after receiving introduction for PD during admission. The choices of PD modality were compared between 2 groups of pts (regardless of whether the pts have had pre-ESRD education or not), are not significantly different (31.8% vs 28.4%, p=0.073). In addition, we found that pts had pre-ESRD education had significantly shorter hospitalization days than those did not have pre-ESRD education (13.7±10.5 vs 20.5±15.1 days, p=0.002) The incidence of educated pts needed emergency hemodialysis (HD) are less than uneducated pts significantly (15% vs 45.2%, p=0.035). Compared the 3-year survival rate there was no significant difference between pre-ESRD educated pts and did not have pre-ESRD education pts (p=0.764). In those pts received RRT, the 3-year survival rate was best with pt chose to do PD as maintaining therapy: pts who chose to do HD therapy was better; pts who initiated emergency HD before PD was the least (p=0.001). Conclusion: In current retrospective review, pts received education are more intend to choose PD modality. Pre- ESRD educated pts has significantly chose of dialysis mode earlier and initiate dialysis timely; decreased risk of emergency HD, and shorter hospitalization day, choice of PD may have better long-term survival rates.
Chen Y.L., Yu Y., Huang C.Y., Yang Y., Division of Nephrology, Department of Internal Medicine, Changhua Christian Hospital, Changhua, Taiwan ROC.
IPD—is there Still a Place for It?
Objectives: The average age of ESRD patients is increasing in the U.K. Frail, elderly patients may find HDX to be too hemodynamically unstable, and the preferred choice for these patients would be CAPD, but they are unable to manage this at home. IPD was offered as an alternative therapy to these patients.
Methods: Staff at a local community hospital were taught to manage elderly patients having IPD. Ongoing training and support are provided by PD nurses, with the nurses visiting bimonthly Medical review is conducted every 4 months.
Results: Over a period of 2 years and 6 months, 7 patients have been successfully maintained on IPD, giving 121 total months experience. The average age on starting IPD was 80 years and 8 months (range 72-91 years). Average survival time was 17 months (range 4-31 months) There were no exit-site infections, and only 1 episode of peritonitis (coagulase-negative staphylococcus). Four hospital admissions, an average of 9.7 hospital days per patient, of this only 1 admission was dialysis related Although Kt/V was not checked, patients’ biochemical results remained stable with an average Hb of 11.2 mmol, and average albumin of 33.4 g/L.
Conclusion: Survival of this cohort of patients was comparable to other matched patients starting either HD or CAPD. IPD can be used as a holding place until patents are transferred to HD, and it can maintain octogenarians keeping them well, and offering them company and nursing care twice per week.
Coulthard G., Bennett J., Ipswich Hospital, Ipswich, United Kingdom.
Encapsulating Peritoneal Sclerosis (EPS) following Renal Transplantation
EPS is becoming a more frequently recognized complication in patents (pts) who have undertaken peritoneal dialysis (PD) This is characterized by progressive intra-abdominal fibrosis resulting in compromised motility and function of the bowel. Little is known about the incidence, pathophysiology, and management of this condition with suggested treatment options including enteric rest, tamoxifen, and immunosuppression Case reports and small case series have suggested that immunosuppression is associated with clinical improvement and improved survival This case series however reports 4 cases of EPS which occurred in the first 6 months post renal transplantation (Tx) at the Manchester Royal Infirmary. All pts were receiving immunosuppression with tacrolimus (Tac) and mycophenolate mofetil (MMF). Three pts received IL-2 blockade Three pts were treated with ATG for episodes of vascular rejection which resolved. In 1 pt vascular rejection lead to loss of the graft. The mean age of the pts at time of EPS diagnosis was 31 years (IQR 24-44) and the mean time on PD prior to Tx was 48.22 months (IQR 27-70). Two pts received live related donor kidneys and 2 were from cadaveric donors (Table). Clinical symptoms included vomiting, diarrhea, and abdominal pain. EPS was diagnosed following abdominal CT scans. All pts then had a peritoneotomy with adhesiolysis and showed good recovery. This case series demonstrates that EPS can occur early in the post Tx period in pts previously been treated by PD. A high clinical suspicion is required to make the diagnosis as treatment with mycophenolate mofetil resulted in diagnostic delay, due to gastrointestinal symptom overlap. In this group however successful surgical intervention resulted in no mortalities.
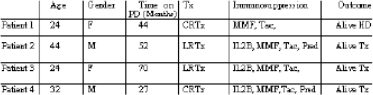
De Freitas D.G., Hurst H., Jordaan A., Tavakoli A., Brenchley P.E.C., Hutchison A.J., Summers A.M., Manchester Institute of Nephrology and Transplantation, Manchester, United Kingdom.
Economy of Renal Replacement Therapy Modalities in Iran (PD vs HD)
Background: Health care expenditure in European countries varies between 11% of GDP (Germany) and 6% of GDP (Luxemburg), whereas in Iran, this figure approaches 4% of GDP. On the other hand, dialysis costs (compared to the total health budget) vary between 36% in France and 19% in Germany, while not more than 0.04% of the general population is under dialysis. In previous studies performed by the MOH, CAPD was introduced to be more expensive (around 7900 US$ annually) than hemodialysis (HD around 5500 USS annually) in the governmental sector. As this report contradicts with the information from other regions of the world, where CAPD is at least 30% cheaper than HD, we decided to have a second thought on this issue in Iran.
Methods: According to the international guidelines we have classified all the related expenses into 6 general categories, summarized as below: (1) hardware and services (costs for HD 8 RO machines, repair/maintenance); (2) physicians & nurses (payments to the medical staff); (3) pharmaceuticals (medications, heparin, erythropoietin); (4) consumables (sanitary items, disposables, catheter/solutions); (5) complications costs: (6) others (food, transport, patients sick leave, para-clinic tests).
Results: Annual Costs/Patient: HD: 11,572 US$ vs CAPD: 10,674 USS.
Conclusion: CAPD is at least 7.5% cheaper than HD in Iran, with the low number of current PD patients being the reason for its relative expensiveness. In contrast to other countries CAPD costs (22759 in Turkey, 37000 in Canada, and 11700-28496 US$ in Europe), Iran is still one of the cheapest CAPD countries around the world.
Farhang Zangneh H., Najafi I., Manbachi M., Kasirloo M., Keyvani M., Nephrology Research Center-Shariati Hospital, Tehran, Iran.
Esophageal Moniliasis and Gastrointestinal Symptoms in Peritoneal Dialysis Patients
Gastrointestinal symptoms and infections disorders are common among patients with end-stage renal disease treated with peritoneal dialysis (PD) The prevalence of esophageal moniliasis in PD patents is not known. Objective: We aimed to evaluate the frequency of gastrointestinal symptoms and risk factors for the esophageal moniliasis in a cohort of patients treated with PD Methods. 30 patients on PD were followed far 2 years. Demographics and laboratorial (creatinine, urea. KtV, hemoglobin, albumin, calcium, phosphorus, PTHi, lymphocytes, monocytes) data, MIS (malnutrition, inflammation score), body mass index (BMI), symptoms of upper gastrointestinal system, and upper gastrointestinal endoscopy (UGE) were recorded. Data are expressed in mean±dp or percentage. Patients who presented esophageal moniliasis were compared with those who did not present using the test t Student and χ2. Differences were considered significant when p≤0.05. Results: Mean age of the group was 57±14 years. 63% were women, 37% were diabetic, 63% APD, time in dialysis 34.8±26 months, 7% were smoker, and 23% reported occasional alcohol consumption. The average MIS punctuation was 6±5, with 85% less than 10. The BMI were 26.7±5, urea 98±32, creatinine 9.3±2.7, Kt/V 1.9±0.4, albumin 3.4±0.4, and hemoglobin 11±1.7. 62% presented gastrointestinal symptom and were not correlated with the UGE. The prevalence of the esophageal moniliasis was 10%. In this study, we have demonstrated that prevalence patients with chronic renal failure on PD that presented gastrointestinal symptoms were higher. Factors were related with the moniliasis: low hemoglobin level (p=0.03), low monocytes level (p=0.04), and higher urea level (p=0.07). Conclusions: The present study suggests that esophageal moniliasis was common was generally oligosymptomatic and related with sub dialysis, even though the patents presented normal KtV. Accompanying with the UGE in this patients must also be taken into consideration.
Fernandes N.M.S., Henriques V.T., Magalhaes T., Passi F., Suassuna P., Fernandes N. S., Fernandes F., Fajardo M., Bastos M.G., NIEPEN da Fundacao IM EPEN- UFJF, Juiz de Fora, Brazil.
Pilot Study on Telecare Monitoring of Peritoneal Dialysis Patients in a General Hospital
Background: With recent advances in telecommunication technology especially in the health care sector, we piloted a study looking into monitoring of patents (pts) on peritoneal dialysis (PD) using Telecare system as part of Singapore Health Services (Singhealth) initiative to improve health care. This project is part of the Telecare initiative in Singhealth (MyTelecare) Aim: To (1) assess feasibility and safety of the system; (2) improve monitoring of PD pts, documenting trends digitally; (3) identify problems early and institute treatment. Method: Four PD pts were selected, age 22-56 years; study period 6 months. They were trained to use MyTelecare system. Pt login to send in vital signs and symptoms via MyTelecare Internet portal or mobile phone (SMS). Parameters monitored were temperature, blood pressure, blood glucose level, weight ultrafiltration, flow times, exit site, and effluent status. Data transmitted via the Internet will be accompanied by a customized symptom questionnaire The ranges far the parameter and auto-alarm indicator were customized. Upon receipt of an SMS message, the physician will I acknowledge the alert by SMS and execute appropriate treatment, conversely, the physician can login to MyTelecare portal to view pt's charts, symptom questionnaires and answer queries. Hospital Ethics Committee's approval was obtained. Results: All pts found this farm of documentation useful in providing them an insight into their daily treatment The ability to get feedback within 24 hours provided reassurance. One pt, a teenager, was noted to be noncompliant with entry and this prompted regular phone calls and home visits. Another pt was able to get his queries answered while abroad. A third pt developed vesicles akin to chickenpox and was directed to the hospital for communicable diseases By and large the main alerts were for hypertension out of specified range and ankle edema Conclusion: The study was widely welcomed by both physician and pts. Pts were more motivated with their treatment Reducing hospitalization and ad hoc visits overall reduces cost to pt and public health care services. This technology will revolutionize the way we practice medicine in the future.
Foo M W.Y.1, Suhail S.M.1, Lim F.S.2, Chua H.L.3, Yong K.M.1, Wong K.S.1, Dept of Renal Med,1 Singapore General Hosp; Singhealth Innovative Technol Application Group iTAG/Infotech2; Singapore Children's Society-SGH PD Centre,3 Singapore.
Intermittent Peritoneal Dialysis: A Therapeutic Option for Third World Patients
Objectives: To report the results of 10 years of experience of a Cuban nephrology service and demonstrate that this technique is still an alternative of treatment for most of the patients in least developed countries despite recent advances in the management of the disease.
Methods: A retrospective study that enrolled the 82 patients starting peritoneal dialysis at the service of nephrology of our institution, in the period of time between 1995 and 2005 Data are reported for these patients who were stable on peritoneal dialysis for at least 24 months and who were on intermittent ambulatory peritoneal dialysis. We present survival of the method, man complications, program withdrawals, and the rate of mortality.
Results: Mean age was 58.1 years, 56% were female, while 44% were male Hypertension was the primary cause of renal failure in 40 patients, Diabetes mellitus was in 20 patients while the rest of the subjects because different reasons. The main complications were catheter out of place peritonitis, obstruction, and sepsis. Mortality rate was of 6% of patents.
Conclusions: The success of peritoneal dialysis programs relies on many elements, most importantly an integrated approach to care by all members of the peritoneal dialysis team The peritoneal dialysis team included not just health professionals but also patients, their families their communities, and other support people. This modality is an alternative for the least developed countries.
Fors E.C., Gonzalez O., Martinez M., Lasa A., Carios J., Finlay Hospital, Havana, Cuba
Age and Bone Mineral Density in Dialysis Patients
Our earlier study displayed lower serum native parathyroid hormone (iPTH), 1-84PTH, 7-84PTH, and higher osteoprotegrin in dialysis patents older than 65 years in comparison to younger ones (J Int Urol Nephrol, in press). The aim of present study was to evaluate bone mineral density (BMD) and relate it to other parameters that may influence bone tissue. The study was performed in 14 dialysis patients divided into 2 groups according to age. Group I (n=8) consisted of patients older than 65 years (73.3±5.7 years dialysis vintage 25.6, 10.1-42.8 months) Group II (n=6) consisted of younger patents (43.6±10.8 years, dialysis vintage 38.9,12.1– 59.6 months). Both groups included 2 hemodialysis patients; the others were treated with peritoneal dialysis. BMD was examined in 2 sites by DEXA. Simultaneously the following parameters were evaluated serum iPTH, calcium-phosphate balance parameters, blood pH, markers of inflammation, bioimpedance records of body composition, serum and anthropometric markers of nutritional state Separation of patents according to T-score is presented in the Table Significant differences between groups concerned only BMD measured in N (0.663±0.078 for group I vs 0.737±0.180 g/cm2 for group II, p=0.039), T-score(-2.93,-4.06–1.55 for group I vs 1.06, -3.54, 0.37 for group II, p=0.039), and BMD as % of peak BMD (64.5%, 54.2, 81.0% for group I vs 83,4%, 61,4, 104,0% for group II), indicating lower BMD in older dialysis patients. Not significant differences between groups in iPTH and other examined parameters suggest that metrical age is the most important factor influencing loss of BMD. Higher BMD in L compared to that in N occurs probably due to age-related spondyloarthrosis.

Grzegorzewska A.E., Mlot Michalska M., Karol Marcinkowki University of Medical Sciences, Poland
Short Break-in Period: A Safe Practice
Time between peritoneal dialysis (PD) catheter insertion and initiation of dialysis is defined as break-in period. Conventionally a break-in period of 2-3 weeks is advised to prevent leaks or infections. We have been practicing short break-in period at our center for last 5 years We studied infective and no infective complications associated with short break- in period in our patents in first 6 months of break-in period A total of 44 patients of meant ±SD age 57.86±12.9 years (20-80 years), 30 males & 11 females were studied. 23 were diabetes and rest nondiabetic. Mean follow-up period was 32.9±23.6 months (6-113 months). All catheters were placed surgically by single surgeon. Straight double cuff Tenckhoff catheter was used in all cases. Patents were usually initiated on PD with 4 exchanges. 500 mL volume flush on the first day after break-in period. This was followed by 4 exchanges of 1000 mL each without dwell time on the next day. Subsequently dwell time was progressively increased so that by sixth day, regular exchanges i.e. 4 exchanges of 2 L each with dwell time of 3-4 hours were done. Mean break-in period was 7.71±9.1 days (0-47 days, n=41). After excluding patients where break-in period was delayed for more than 7 days, mean break-in period was 4.24±1.8 days (0-7 days, n=33). Among noninfective complicates there was pericatheter leak in 1, hydrocele in 1, catheter migration in 1, tunnel hematoma in 2, incisional hernia in 1, bubonocele in 1, hiatus hernia in 1 There was no episodes of peritonitis, exit site or tunnel infection. We suggest that risk of leak & infective complications are negligible with short break-in period and it is a safe practice in at least surgically implanted catheters.
Gupta A.K., Jasuja S., Indraprastha Apollo Hospitals, Delhi, India.
Video-Assisted Thoracoscopic TALE Pleurodesis for Pleuroperitoneal Communication in Peritoneal Dialysis
Acute symptomatic hydrothorax due to pleuroperitoneal fistula is a complication of peritoneal dialysis which is uncommon but well recognized There is no consensus for the best treatment We report a series of video-assisted thoracoscopic surgery (VATS) treated pleuroperitoneal fistulas in our patients. Between August 2000 and February 2006, among 618 new patients in a single center commencing peritoneal dialysis. 6 patients (all female with mean age 60±8 years) developed acute hydrothorax (all right-sided) due to pleuroperitoneal fistula. The incidence was 0.97%. The median onset of symptomatic hydrothorax was 39 days (range 7-131 days) after starting peritoneal dialysis. Analysis of the pleural fluid showed mean total protein level of 2.5±0.8 g/L and glucose level of 17.6±4.5 mmol/L. All patients were treated by video-assisted thoracoscopic pleurodesis with tale powder. There was no morbidity associated with procedure Two patients had recurrent hydrothorax at 41 and 42 days after pleurodesis respectively. They were switched to long-term hemodialysis. In our series, pleuroperitoneal fistula in peritoneal dialysis patient occurs in right side The symptomatic hydrothorax tends to occur within the first 2 months after commencement of peritoneal dialysis. VATS with tale pleurodesis is a safe and effective therapy for peritoneal dialysis patients with pleuroperitoneal fistula to continue peritoneal dialysis.
Ho E.T.L.1, Tang S.C.W.2, Chui W.H.3, Tang A.W.C.1, Wong S.S.H.1, Wong Y.1, Lam W.O.1, Cheng Y.Y.1, Chau W.S.3, Ho Y.W.1, United Christian Hospital,1 Queen Mary Hospital,2 Grantham Hospital,3 Hong Kong.
Successful Training with Use of Success @ Home Materials
Purpose: To evaluate success @ home training materials for nurses and patients. Discussion: Training materials previously utilized were photocopies of FMS training manuals. These were placed into a binder to be renewed with patients. There were no illustrations available to make learning easy and it was very unprofessional looking Method: Success @ home is a new comprehensive peritoneal educational support program now available in our clinic The materials are all packaged conveniently in an attractive storage box which is convenient for easy access by the trainer The training guide is patient friendly and easy to read The text is written at a basic level and is supported with colorful illustrations All materials use simple terminology that is appropriate for all education levels. There is a video which enhances the training. In our clinic the video is typically used in the clinic while the patient takes the manual home to begin reading at their own pace. The material is then reviewed one-on-one with the patient and their partner. Basic Training Flyers, which are included in the success @ home tool kit are provided to each patient. The flyers address such topics as Fluid Balance, Exit Site Care, and Troubleshooting. These flyers reinforce their peritoneal dialysis education. Using all the materials enables us to reinforce peritoneal dialysis concepts and procedures in a multitude of ways. This successful approach has been consistent with adult learning principles. Results: Improved patient compliance with documentation of treatment sheets a noted decrease in phone calls from patients trained with success @ home due to patients having all information available to reference to in one place. The pass rates on quizzes given at the end of training have also improved. Nursing time for training has decreased because there is no longer a need to prepare training materials. The materials are packaged in a convenient “house” for easy access to all items assisting with organization in our training area. Conclusion: We have found the success @ home training materials have enhanced our training curriculum and have resulted in improved patient retention of information.
Holloman L., FMS Rocky Mount, Rocky Mount, U.S.A.
Survey Result of Peritoneal Dialysis Patients who Experienced Niigata Chuetsu Earthquake: Tokai CAPD Nursing Association Report
Background: Result of a questionnaire to members of Tokai CAPD Association asking about the needs of study topic showed strong request on “Disaster Contingency Plan.” This requirement may result from the predicted occurrence of a disastrous earthquake in near future in Tokai area where we base on. This prediction has been referred for more than a decade still waived of its realization and leaving us in an uncertain status “waiting” for the earthquake to happen. Dialysis centers are preparing to countermeasure with a disaster whereas not knowing its true impact, may satisfy with still insufficient contingency plan. It is very important to define truly necessary action and to find the pitfalls of their plans. In order to fulfill the urgent need to formulate effective countermeasure, we intended to collect direct opinions and draw suggestion from a survey of peritoneal dialysis (PD) patients who actually experienced disastrous earthquake.
Methods: Questionnaire was sent to 44 PD patients who are treated at 3 centers in the area where struck with the earthquake. 30 were collected from patients average age of 57.3 years Items asked were as follows history of CAPD, description of their residence, evacuation procedure, damage by the earthquake, lifeline condition, treatment condition, earned out items, meal/diet, communication with the hospital how they felt.
Result and Discussion We identified issues to be solved and necessary countermeasure by collecting the impact of the disaster.
Hosono E.1, Nakabayashi Y.2, Taiseikai Medical Foundation,1 Gifu; Narita Memorial Hospital,2 Toyohashi, Japan.
The Prevalence of TT Virus and SEN Virus Infection in Patients on Peritoneal Dialysis in Eastern Taiwan
Objectives: Many reports have demonstrated transfusion-transmitted virus (TTV), SENV infection rates in hemodialysis patients, but the TTV and SENV infection rate in peritoneal dialysis (PD) patients has never been reported in Taiwan In this study, we determined the prevalence rate of TTV and SENV viremia in a PD population.
Methods: Serum samples from 47 PD patients and a control group of 43 patients at health examination were assayed for TTV, SENV-D and -H viremia by using polymerase chain reaction.
Results: The proportions of blood transfusion (p<0.0001), female gender (p=0.001), young age (p=0.0014), and serum AST level (p=0.012) were significantly higher in PD patients The prevalence of TTV infection is 37.2% in control group and 23.4% in PD patients and SENV infection is 32.6% in control group and 27.7% in PD patients. The prevalence rates of TTV or SENV-D and/or-H viremia were not significantly different between PD and controls. SENV-D (+) patients had lower mean duration of PD than SENV (-) patients. The mean ALT level was significantly lower in SENV-H (+) than SENV (-) patients (12.8±5.8 vs 19.6±12.1, p=0.025). None of the TTV or SENV-infected PD patients had overt clinical or biochemical signs of liver disease and the infection rate was not different between automated peritoneal dialysis (APD) and continuous ambulatory peritoneal dialysis (CAPD) patients.
Conclusions: These results indicate that TTV or SENV infection rate is not different between healthy individuals and PD patients TTV or SENV infection is not associated with evident liver diseases in PD patients and TTV or SENV infection rate is not different between APD patients and CAPD patients TTV or SENV transmission is likely occurs via non-parenteral routes. Different PD procedures may not be an effective way to transmit TTV or SENV.
Hsu B.G.1, Wang CH.1, Fang T.C.1, Lin H.H.2, Division of Nephrology1 and Division of Gastroenterology, Buddhist Tzu Chi General Hospital, Hualien, Taiwan.
Continuous Ambulatory Peritoneal Dialysis (CAPD) as a Model of Renal Replacement Therapy (RRT) in Children and Adults
Objective: CAPD is recently introduced in Pakistan. Our aim was to study the demographic profile and outcome of children and adults on CAPD.
Methods: Children as well as adults who underwent CAPD from January 2003 to August 2005 were studied. The demographic profile, etiology of ESRD, complications, and outcome were studied.
Results: There were 40 patients, 10 children and 30 adults Mean age of children was 9 years. Majority had FSGS followed by hypoplastic kidneys Average duration on CAPD 7.2 months Four children had peritonitis. Organism was pseudomonas in 2, fungus in one, and another had culture negative Two children had exit-site leakage, 1 had extrusion of subcutaneous cuff. Five are still active on CAPD. 3 expired 1 transferred to hemodialysis, and 1 had kidney transplant. Adults were 30, 16 males & 14 females. The mean age was 63 years. Diabetes mellitus (43%) the most common cause of ESRD followed by hypertensive nephropathy (23%) Seven had duration on CAPD from 12 to 36 months and 23 had <12 months Mean Kt/V was 1.8. PET showed low-average and high-average transports (46% & 36%). Eight had peritonitis Organism was pseudomonas (3), culture negative (2), tuberculous, Rhodococcus, and Stenotrophomonas maltophilia in 1 each Five had Tenckhoff catheter migration, 2 had abdominal wall leakage, and 1 had exit-site leakage. 18 (60%) are still active on CAPD, 3 transferred to hemodialysis, 3 had kidney transplant, and 6 expired.
Conclusion: CAPD is an effective and patient-friendly modality. This is a viable option for patents with rural background. Incidence of peritonitis is 1 episode 22 patients months. CAPD is underutilized in our country Expensive solutions, acceptability among patients, resistance among medical community are the factors most influential on this modality.
Hussain R., Naqvi S.A.J., The Kidney Foundation, Karachi, Pakistan
Recovery of Renal Function during CAPD in IgD Myeloma Patient with Kidney Failure: Case Report
IgD myeloma is a rare disease, comprising only 1%-2% of all cases of multiple myeloma and renal failure is a common complication. We report the case of a 49-year-old man admitted with anuria, hypercalcemia, and anemia. Clinical exams and laboratory findings revealed an IgD kappa multiple myeloma (64% medullar plasmocytes infiltration) with acute renal failure Conservative treatment goes to recovery of diuresis without recovery of renal function (creatinine Cl 10.1 mL/min, serum creatinine 15.4 mg/dL) Dialysis was necessary and a CAPD schedule with standard glucose-containing lactate-buffered peritoneal solutions. 4 changes/day (3x2000 mL 1.36% + 1x2000 mL 2.27%, Baxter) was performed Two monthly cures of chemotherapy of induction according to the protocol VAD (vincristine 2 mg, doxorubicin 40 mg/m2, dexamethasone 40 mg on days 1-4,9-12,17-20) allowed to achieve recovery of renal function and independence to CAPD program (serum creatinine 2.47 mg/dL, creatinine Cl 57 mL/min, without CAPD). There were no severe adverse events during CAPD. Peritoneal leak due to malignant obesity appeared in the first period after catheter insertion. No peritonitis, tunnel or exit-site infections were registered during CAPD. In this case CAPD allowed the recovery of renal function in an IgD myeloma patient. Also, this observation allows displaying the particularities of IgD myeloma remarkable preponderance of kappa-type light chains, small or no visible monoclonal spike on serum electrophoresis, renal failure and the presence of osteolytic lesions. CAPD as dialysis support should be considered whenever necessary for all newly diagnosed patients with myeloma and renal function does not improve with aggressive initial therapy.
Ionescu C.A.1, Busuioc E.1, Gilice E.1, Coriu D.2, Voiculescu M.1, Nephrology Center1 and Hematology Center,2 Fundeni Clinical Institute, Bucharest. Romania.
The Efficacy of a Neutral Peritoneal Dialysis Fluid with Less 3,4-DGE for Preservation of Peritoneal Cells in Peritoneal Rest Therapy
Objectives: To examine the effect of peritoneal rest to preserve peritoneal function, we investigated the cytotoxicity of several peritoneal dialysis fluids (PDFs) using an in vitro peritoneal resting model with human peritoneal mesothelial cells (HPMCs) and human umbilical vascular endothelial cells (HUVECs). Methods: We prepare heat-sterilized one-compartment standard type PDF (low-pH fluid pH 5.5) containing 1.36% and 3.86% glucose as well as heat-sterilized dual-chamber type PDF (neutral-pH fluid pH 6.7). HPMCs and HUVECs were pre-exposed with PDFs prepared as mentioned above for 4 hours, followed by resting in cell culture medium for 24 hours to recover from damage (peritoneal resting model) The viability of resting or non-resting cells was measured by MTT assay. Also, the affect of stimulating solution which spiked with 25 μol/L of 3,4-DGE in PBS at the different pH levels (5.5 and 6.7) was evaluated. Results: Pre-exposure of cells to low-pH fluid or neutral-pH fluid reduced the MTT viability respectively. The MTT viability of cells subsequent 24 hours recovery was not improved 4 hours pre-exposure of low-pH fluid, but was improved in the case of 4 hours pre-exposure of neutral-pH fluid 3,4-DGE-containing stimulating solution at pH 5.5 was significantly impaired the cell viability for 4 hours treatment These data demonstrated that 3,4-DGE was a critical element of PDF induced cytotoxicity. We observed previously that the reactivity of 3,4-DGE against protein was more intensive than any other glucose degradation products. Thus, modification of cellular protein by 3,4-DGE may cause irreversible injury to peritoneal cells. Conclusions: We considered the direction of neutral PDF with less 3,4-DGE was available for the peritoneal rest. It was indicated that the combination therapy of PD with neutral PDF and hemodialysis might be very effective for conservation of peritoneal function.
Iwashita T.1, Tomo T.1, Okabe E.1, Matsuyama K.1, Kadota J.1, Yamamoto T.2, Faculty of Medicine,1 Oita University, Oita; JMS Co., Ltd,2 Hiroshima, Japan.
Polyneuropathy in Diabetic and Nondiabetic Patients on CAPD
It is well known that patients with uremia as well as patients with diabetes mellitus (DM) develop polyneuropathy In the present study the signs of polyneuropathy in diabetic and nondiabetic patients on continuous ambulatory peritoneal dialysis (CAPD) were analyzed 63 CAPD patients (37 men), aged between 30 and 85 who were on dialysis from 1 month to 14 years, were analyzed Patients were divided into 2 groups group 1:20 DM patients, mean age 50.1±13.2 years: group 2:43 non-DM patients, mean age 62.3±9.7 years Biochemical parameters and dialysis adequacy (Kt/V) were determined Motor conduction velocity(MCV) of peroneal and tibial nerve, and sensitive conduction velocity (SCV) on sural nerve were measured. Diabetics were significantly younger, with lower level of creatinine and higher glucose concentration (p<0.01), but there were no deference's in gender, CAPD duration, hemoglobin, urea, and Kt/V. All analyzed neurophysiologic parameters were pathological in diabetics. In non-DM patients, prolonged latency of F wave on peroneal and tibial nerves and reduced SCV on sural nerve was found. All analyzed parameters were significantly different between studied groups (p<0.001). In diabetics significant correlation was found between peroneal MCV and duration of dialysis peroneal F wave and urea; tibial MCV and Kt/V; tibial terminal latency (TL) and duration of dialysis, creatinine and glycemia; SCV on sural nerve with Kt/V. In non-DMs significant correlation was found between peroneal F wave and urea, creatinine and creatinine clearance; tibial MCV and age tibial F wave and creatinine and Kt/V.
In conclusion, polyneuropathy was significantly worse in diabetics, and correlated with dialysis adequacy in both groups as well as with glucose concentration in diabetics and age in nondiabetics.
Jovanovic D B.1, Matanovic D.2, Stosovic M.1, Bontic A.1, Nesic V.1, Institute of Urology and Nephrology,1 Center of Physical Medicine and Rehabilitation,2 Belgrade, Serbia.
CAPD is an Acceptable Treatment Option for ESRD Induced by Glycogen Storage Disease Type 1: A Case of Long-Term (over 14 Years) CAPD Patient after Transferred from Hemodialysis
Glycogen storage disease type 1 (GSD1) results from deficient glucose-6-phosohatase activity and causes several metabolic disorders including hypoglycemia. Glycogen accumulation in the kidney causes renal disease We have reported that CAPD ameliorated metabolic disturbances of a patient with end-stage renal disease (ESRD) caused by GSD1 previously. We, here, report an excellent outcome of the patient maintained by CAPD for 14 years.
Case: The patient was diagnosed GSD1 at the age of 3. She initiated hemodialysis (HD) at the age of 28 by the loss of renal function. However, it was difficult to maintain her well because of frequent episodes of hypoglycemia and hypotension during HD session. So we expected that continuous glucose supply from the dialysates by CAPD might improve metabolic state After transfer to CAPD, she did not experience hypotension. Plasma glucose levels and metabolic acidosis were improved obviously. Also, the values of ketone, nonesterified fatty acid, blood BUN/Cr, and glucagons were improved comparing those in HD. Peritoneal equilibration test showed almost no changes during 14 years that D/PCr: 0.67 to 0.71. Therefore, high glucose dialysates were not required for maintaining optimal hydration. The patient is now ongoing stable CAPD for 14 years without CAPD-related complications.
Conclusion: CAPD is a beneficial effect by continuous glucose supply from the dialysates. Thus, it is useful renal replacement therapy (RRT) for ESRD due to GSD type 1. We have experienced a very valuable case maintained by CAPD for the duration as long as 14 years. From the successful experience shown in this case, another case of ESRD due to GSD type 1 initiated CAPD as her first RRT, now who is on going on good course.
Kawamura Y., Yamamoto H., Yaginuma T., Yoshida H., Tanno Y., Yamamoto R., Hayakawa H., Hanaoka K., Ikeda M., Yokoyama K., Kawaguchi Y., Hosoya T., Div of Kidney & Hypertens, Dept of internal Med, Jikei Univ School of Med, Tokyo, Japan.
A Multicenter Survey on Peritoneal Dialysis Patients in Yamagata Prefecture, Japan
Objectives: Peritoneal dialysis (PD) has been utilized for end-stage renal disease (ESRD) patients for more than 20 years in Japan. In this study, we summarized the current state of PD therapy in Yamagata prefecture. Japan.
Methods. A retrospective multicenter survey on PD patients treated between 2003 and 2005 was carried out in Yamagata prefecture (population 1.2 million)
Results: At the end of 2003, there were 156 patients on PD (9.2% of all ESRD patients, mean age 66.9 years) and 1684 patients on hemodialysis (HD, mean age 62.9 years). During the year 2003, 43 patients (18.5% of new ESRD patients) were newly introduced to PD Mean age at initiation of dialysis therapy was 67.8 (26-93) years for PD and 65.8 years for HD, respectively. The prevalence of PD in all or new ESRD patients and age of new ESRD patients in Yamagata were higher than those of national average (3.8%, 4.7%, and 65.4 years, respectively) As major diseases causing ESRD, the prevalence of chronic glomerulonephritis, diabetic nephropathy were 46.2%, 26.9% for PD and 26.7%, 39.1% for HD, respectively. After 2 years follow-up of 43 PD patients started in 2003, 26 patients (60.5%) were still on PD, 3 patients (7.0%) were switched to HD. 8 patients (18.6%) died and 6 patients were unknown (14.0%). The 2-year survival rate was higher (0.784) in PD than that in all ESRD patients (0.751). The major causes of death in PD patients were congestive heart failure and infections.
Conclusion: These results indicated that PD therapy was mainly used for relatively elder patients with nondiabetic renal diseases, leading to high persistence rate in Yamagata, Japan.
Konta T.1, Ito M.2, Degawa N.2, Masakane I.2, Sato K.2, Takaiwa M.2, Ikeda A.2, Oyama Y.2, Takasaki S.1, Yamagata University School of Medicine,1 Yamagata PD Group,2 Yamagata, Japan.
Renal Protective Effects of Erythropoietin in Experimental Unilateral Ureteral Obstruction
Erythropoietin (EPO) modulates a broad array of cellular processes that include progenitor stem cell development, cellular integrity, and angiogenesis. The results of recent studies show that systemically administered EPO is protective in vivo, in several animal models of renal injury Tubulointerstitial fibrosis and mononuclear cell infiltration are known as major renal pathologic findings in obstructive nephropathy. In order to evaluate the effect of EPO treatment on renal injury in experimental unilateral ureteral obstruction (UUO) model, male Sprague-Dawley rats weighing 230–260 g underwent sham operation (n=5), UUO without EPO treatment (n=6), and UUO with EPO treatment (n=7) under anesthesia. Recombinant human EPO was injected intraperitoneally once in a day as a dose of 3000 unit/kg body weight from 3 days before surgery until sacrifice, 3 days after surgery. Competitive RT-PCR was performed for the estimation of TGF-β, MCP-1, osteopontin, Fas and Bcl-2 gene expression levels of the obstructed kidneys. We also evaluated the magnitude of tubulointerstitial mononuclear cell infiltration by immunohistochemistry for ED-1. Renal gene expressions of TGF-β, MCP-1, osteopontin, and Fas in untreated control UUO rats were significantly increased compared to sham operated rats at 3 days after surgery. The level of TGF-β, MCP-1, osteopontin and Fas gene expressions of EPO treated UUO rats was significantly lower than those of untreated control UUO rats (all, p<0.05) The Bcl-2 mRNA level of EPO treated UUO rats was significantly higher than that of control UUO rats The protein level of active caspase 3 measured by Western blot in the kidney of EPO-treated UUO rats was significantly lower than that of control UUO rats (p<0.01). On microscopic examination of obstructed kidneys, EPO treated UUO rats showed significantly less interstitial ED-1 antigen positive mononuclear cells compared to control UUO rats.
In conclusion, we propose that EPO may have protective effects on renal injury process in experimental unilateral ureteral obstruction.
Lee K.W.1, Chang Y.K.2, Lee Y.M.1, Na K.R.1, Suh K.S.1, Shm Y.T.1, Renal Division,1 Chungnam National University Hospital; Internal Medicine,2 Medical College. Catholic University, Daejeon, South Korea
Managing Continuous Ambulatory Peritoneal Dialysis (CAPD) Patient Training Program
Background: CAPD is the first option of dialysis management of endstage renal disease patients in the locality. Training patients and the family for subsequent effective CAPD management at home is time consuming and manpower demanding. The center previously operated the training program as daily 8-hours trainings until both the teaching nurse and the learner patient agreed for patient commencing self-health management by CAPD at home Most patients needed at least 6 training days With the growth of dialysis service demand due to escalating number of CAPD patients, the acute hemodialysis supports needed, and the stringent nursing manpower resources available, the CAPD patient training program was reformed since June 2002. It was aimed to shorten the training hours to optimize nursing manpower utilization without jeopardizing CAPD patient outcomes while sustaining efficient hemodialysis services by the nursing team. Objectives: Instead of aiming to transfer all CAPD-related knowledge and skill, i.e. what nurses consider patients ought to know, critical information with transfer of safe techniques, i.e. what nurses consider patients need to leant, became the essence of the program. The outcomes of the new program were evaluated retrospectively to validate the effectiveness of the program. Method: Two-year outcomes in terms of peritonitis rate of the home CAPD patents recruited during the first quarters of the years 2001-2004 were monitored. Patient demographics were compared Training hours were compared. Results: The average number of patents recruited in each period was 31 (range 24-34). The nursing manpower in terms of man-hours for CAPD patient training was reduced by over 50%. The peritonitis episodes and the related hospitalization days were comparable. Conclusion The patent outcomes were not sacrificed in the reformed training program. The time and manpower utilization was optimized in the dialysis facility Long-term strategy for patient training and monitoring might deserve further exploration.
Leung D.K.C., Lee M.K.F., Lo H.H.L., Tang Y.L., Yu D.M.W., Renal Unit Tuen Mun Hospital, Tuen Mun, Hong Kong.
Acute Pancreatitis in Patients with Peritoneal Dialysis and Hemodialysis
Background: It has been postulated that the incidence of acute pancreatitis in patient with end-stage renal disease is increased. But the difference between peritoneal dialysis (PD) and hemodialysis (HD) was unclear. We try to evaluate the incidence, risk factors, severity, and outcome of acute pancreatitis in PD and HD patients.
Methods: This is a retrospective cohort study. From January 1997 to October 2005, patients who maintained on PD or HD for more than 6 weeks in a medical center of Taiwan, that developed an attack of acute pancreatitis (diagnosed by abdominal pain plus increased serum lipase or amylase 3 times higher than normal value) were enrolled The incidence, possible risk factors, severity, and outcome were analyzed.
Results: There are 634 patients maintained on HD (average follow-up 43.4 months) and 236 patients maintained on PD (average follow-up 27.5 months) in the study period In the patients on HD, 9 patients had an attack of acute pancreatitis (incidence 0.39% per year). In the patients on PD. 9 patients had an attack of acute pancreatitis (incidence 1.66% per year). In Cox model, patients on PD had a higher risk (4.3 times) of acute pancreatitis than patient on HD (p=0.007). In Fisher test, we compared the contributing factors (alcohol consumption, gall stone, serum triglyceride, and serum ionic calcium), age, sex, white blood cell count, albumin. AST. Glasgow scale. Balthazar grade, and mortality rate between 2 groups. The PD patients had a higher serum triglyceride level than HD (511±462 vs 161±60 mg/dL, p=0.003), but there are no significant differences of other parameters between patients on PD and HD.
Conclusion: The incidence of acute pancreatitis in patients on maintenance PD is higher than on HD Although there was no difference of severity and mortality between patents on PD and HD, a higher serum triglyceride level may be the contributing factor of PD patients to develop the acute pancreatitis.
Lin C.Y.1, Chang C H.1, Chen J.H.2, Division of Nephrology,1 Division of Gastroenterology,2 Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan.
Tuberculous Lymphadenitis Complicating CAPD: Review of Nine Cases
Objective: To review the clinical features of tuberculous (TB) lymphadenitis in patients undergoing CAPD in an endemic area.
Methods. The hospital records of all CAPD patients being followed up in our dialysis centers between January 1995 and December 2004 were reviewed Patients with history of TB lymphadenitis were identified and their clinical characteristics were retrospectively analyzed.
Results: Nine cases of TB lymphadenitis were identified among 910 CAPD patients over a period of 10 years. There were 4 female and 5 male patients with a mean age of 5.11±5.5 years The mean duration of CAPD was 44±44 months. The TB lymphadenitis involved the cervical lymph nodes (LN) in 6 patients, supraclavicular LN in 2 patients, and mediastinal LN in 1 patient Six patients presented with enlarged LN clinically. Four of them also had fever. Three other patients were incidentally found to have enlarged LN on CXR (1) and on ultrasound examination of the neck (2). Diagnosis of TB lymphadenitis was made by demonstrating caseating granuloma with or without positive AFB smear on excisional LN biopsy All patients were treated with isoniazid, rifampicin, and levofloxacin for 12 months and pyrazinamide for the first 3 months. The anti-TB treatment was in general well tolerated. One patient developed transient liver function derangement and 1 patient developed paradoxical reaction. None of them required discontinuation of the anti-TB treatment. The patients had been followed up for 59±30 months. None of them had developed recurrence of the TB lymphadenitis.
Conclusions: TB lymphadenitis is not an uncommon complication of CAPD in endemic area. High index of suspicion is needed to diagnose this condition early as the enlarged TB LN might be detected incidentally. Treatment with standard anti-TB drugs for an extended duration of 12 months appears to be effective.
Lui S.L.1, Yip P.S.1, Chan T.M.2, Lai K.N.2, Lo W.K.1, University Department of Medicine,1 Tung Wah Hospital. University Department of Medicine,2 Queen Mary Hospital, Hong Kong.
The Increased Risk of Glucose Metabolism Disorders (GMD) in Peritoneal Dialysis-Treated Kidney Allograft Recipients
Background and Aims: The development of GMD [including impaired fasting glucose (IFG), impaired glucose tolerance (IGT), post-transplant diabetes mellitus (PTDM)] are serious complications of kidney transplantation (kTx) associated with an increased risk of chronic transplant dysfunction and cardiovascular morbidity and mortality It is well known that both insulin resistance and insulin deficiency are involved in the pathogenesis of GMD in kidney transplant recipients. An unresolved problem associated with peritonea dialysis (PD) is glucose absorption and caloric intake The aim of the study was to assess whether mode of dialysis [hemodialysis (HD) and PD] influence on development of GMD in kTx recipients.
Materials and Methods: All consecutive patients (pts) (n=353; 139 F/214 M) who received a kTx at our center between 2003 and 2005 were studied. 288 pts (82%, 101 F/187 M) were treated by HD before kTx and 65 pts (18%; 37 F/28 M) by PD. At time of kTx diabetes mellitus (DM type 1/2) was known in 47 pts (13%; 21 F/26 M); 31 HD pts (9 F/22 M) and 16 PD pts (12 F/4 M). GMD was diagnosed according to current American Diabetic Association/WHO criteria.
Results: Among total 306 pts (118 F/188 M; 257 HD/49 PD pts) who were nondiabetic in pretransplant period, 57 pts (19%; 24 F/33 M) developed GMD after kTx: 39 HD pts (39/257, 15%; 15 F/24 M) and 18 PD pts (18/49. 37%; 9 F/9 M). The frequency of GMD was significantly higher in patients treated prior kTx with PD than with HD (p=0.0095 in chi-square test with Yates correction).
Conclusions: PD-treated patients who are candidates for renal transplantation should be tested with particular scrutiny for GMD. It will allow to implement proper therapeutic measures before transplantation and also select the less diabetogenic immunosuppressive regimen.
Madziarska K., Krajewska M., Mazanowska O., Weyde W., Kusztal M., Klak R., Trafidlo E., Golebiowski T., Bartosik H., Klinger M., Dept of Nephrology & Transplantation Medicine, Wroclaw Medical Univ, Wroclaw, Poland
Adipokines Linking Adipocytes and Vascular Function in Dialyzed Patients May Also be Possibly Related to CD146, a Novel Adhesion Molecule
Adipose tissue is a source of variety of hormones and cytokines, which may contribute to vascular complications. Adiponectin (Adipo) has antiatherogenic properties and attenuates endothelial inflammatory responses, whereas leptin had opposite properties. In renal failure, endothelial dysfunction and atherosclerosis are almost universal. Adipo, leptin, and CD146, a novel adhesion molecule localized at the endothelial junction are elevated in renal failure; however their relationships are not known. The aim of the study was to identify possible correlations between Adipo, leptin, and CD146, and other markers of endothelial cell injury in peritoneal dialysis (PD) and hemodialysis (HD) patents (pts). We assessed Adipo, leptin, markers of coagulation: TAT, prothrombin fragments 1+2; fibrinolysis: tPA PAI-1, endothelial function/injury:vWF, thrombomodulin, VCAM, ICAM CD146; markers of inflammation: TNF-α, IL-6 and hsCRP. Adipo was elevated in dialyzed and correlated significantly, in univariate analysis, with tPA, PAI-1 CD146, and Kt/V in HD and with PAI-1, TAFI, ICAM, and CD146 in CAPD. In multivariate analysis only Kt/V-marker of dialysis adequacy and PA -1 remained positive predictors of Adipo in HO and only CD146 remained a positive predictor of Adipo in all CAPD pts. Leptin was rested, in univariate analysis, with cholesterol, LDL, triglycerides (TG), Adipo, VCAM, thrombomodulin, tPA, vWF, TNF-α, C0146 BMI and tended to correlate with IL-6 in HD. In multivariate analysis, predictors of leptin were TG, tPA, and CD146. In CAPD leptin was related to BMI, cholesterol, TG. In univariate analysis CD 146 correlated with age, creatinine, hemoglobin, dose of calcium carbonate, IL-6 in HD. In multivariate analysis, predictors of CD146 were age, Hb, and Adipo. CD 146 correlated only with WF in CAPO pts. Elevated Adipo related to CD146 may be the expression of a counter-regulatory response aimed at mitigating toe consequences in endothelial damage and increased cardiovascular risk in renal failure. In addition, our results confirm a possible role for leptin in toe relationship between endothelial dysfunction and atherosclerosis in hemodialyzed pts. Our data provide further support for a link between adipocytokines, endothelial dysfunction, and renal failure. However, the pathophysicogical implications of our results should be further evaluated.
Malyszko J., Malyszko J.S., Wolczynski S., Pawlak K., Mysliwiec M., Department of Nephrology Medical University, Bialystok, Poland
Peritoneal Dialysis for Patients with Low Cardiac Function Refractory to Hemodialysis
Objectives: Patients with severe congestive heart failure (CHF) are often refractory to hemodialysis (HD). Peritoneal dialysis (PD) is usually chosen for these patients, because PD is a continuous treatment and has less cardiac burden. The aim of the present study is to elucidate the prognosis of the PD patients with CHF refractory to HD.
Methods: We retrospectively examined clinical characteristics and prognosis of patients who used PD because of their impaired cardiac function and unstable hemodynamics.
Results: Among 150 patients who started PD in our hospital from August 1982 to December 2005, 9 patients were identified with our criteria Eight started PD as their first maintenance renal replacement therapy and I switched from HD to PD because of unstable hemodynamics. They are 7 males and 2 females (average age 78 years) and comprised 6 nephrosclerosis, 2 diabetic nephropathy, and 1 polycystic kidney disease. Comorbid cardiac diseases are 5 cases of ischemic heart diseases, 5 valvular disease, and 3 dilated cardiomyopathy Five patients continued maintenance PD after discharge from the hospital, although the other 4 died during hospitalization (2 heart failures, 1 acute myocardial infarction, 1 sudden cardiac arrest). For the 5 outpatients, during 20±10 (11-34) months after discharge, there has been no aggravation of CHF, but 2 cases of nonfatal myocardial infarction, 1 unstable angina, and 1 cerebral infarction were noted. No technical failure of PD was observed Two patients died of mediastinal tumor at 16 and 26 months and remaining 3 are still on stable PD
Conclusions: PD can be used as the first-line renal replacement modality for severe CHF patients and safely accepted by most of the patients However, severe cardiovascular complications may sometimes develop early in the postoperative period.
Mise N., Mimura I., Sai K., Nishi T., Tagawa H., Sugimoto T., Mitsui Memorial Hospital Tokyo, Japan.
Experience with Program of Incremental Peritoneal Dialysis in Argentina
Objective: Evaluate the efficacy and complications of this therapy with an appropriate cost relation. Methods: Prospective study controlled paired not randomize with 16 patients in DPCA; 14 had residual renal function (RRF) (9 women and 7 men), with an average age of 56±19 years. They were followed up 28±17 months with 4 exchanges (8 L/day) (control groups) and then, they were followed up 28±4 months with 3 exchanges (6-7.5 L/day). All have catheters of swan neck coil. Peritonitis was diagnosed according to the criteria reported by ISPD. Kt/V and CCr were calculated according to Keshaviah, the V according to Watson. If the weekly Kt/V was less than 1.7 or the patient had uremia symptoms, the volume was increased and/or the number of exchanges. All the patients had simvastatin of 10 mg/day dose during the study. Results: Some patient characteristic and clinical data are shown in Table 1. Significative deference's where not found among the years 2002, 2003, 2004 in the rate of infections rate hospitalized, adequacy, arterial pressure, etc. There was a significative difference in the peritoneal glucose uptake (p>0.001), triglycerides, cholesterol (p>0.001); relation between the cost of the product and the payment for the service (p>0.001). Three patients abandoned the therapy: 1 because of transplant and 2 went to hemodialysis because of social causes Conclusion This therapy an excellent option for patients selected. It maintains adequate efficiency cost relation, which permits to maintain this technique in Argentina, but without doubts to show certain advantages of this variant vs the standard therapy it is necessary a prospective study controlled long-term.
Incremental peritoneal dialysis patient characteristics
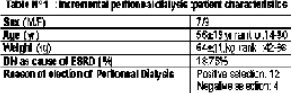
Moretta G., Pedrazz R., Flores G., Coceres M.A., Gomez B., Veniani J., Argentina.
Two Cases of Fabry's Disease Complicated Impaired Peritoneal Function
Fabry's disease (FD) is an X-linked disease caused by a deficiency of alpha-galactosidase, which leads to progressive lysosomal accumulation of globotriaosylceramide (GL3) and resulted in multiorgan damage, such as kidney, heart, endothelial cells, and more. Although FD is rare disease, it is recognized in about 1% of dialysis patients, as kidney is one of the most severely affected organ But there have been few reports about FD patients on peritoneal dialysis (PD) and especially few about peritoneal function of FD. In the first male case. PD was started at age of 37. Extremely low fluid removal rate was recognized at the initiation of PD and remained even after use of higher osmolar dialysate As chronic heart failure (CHF) hardly to improve, developed with hypertrophic cardiomyopathy PD was discontinued to alter hemodialysis (HD). At 6 years later after start of PD, FD was diagnosed and enzyme replacement therapy (ERT) was started at 2 years later but CHF did not change for better. 38-year-old male is the second case. He was admitted to our hospital because of CRF of unknown origin. PD was selected at the first He also could not remove fluid enough to decrease edema. His peritoneal function evaluated by PET was high. At 2 months later, FD was diagnosed and ERT was started After 6 months of ERT, fluid removal rate was improved concomitantly with decreased serum GL3 levels. As peritoneal function of FD is obscure by now, considering that vascular system dysfunction by GL3 accumulation in FD, peritoneal damage seems to occur like our cases Point of no return exists even under ERT but probably not at initiation of dialysis therapy So it seems important to find FD at latest by start of dialysis and treat with ERT.
Nakashima Y.1, Wakasa M.1, Goto M.1, Shishido K.2, Sekishinkai Kawasaki Saiwai Hospital,1 Sekishinkai Kawasaki Clinic,2 Kawasaki, Japan.
Subcutaneously Tunneled Catheters: Three Italian Dialysis Units’ Experience
Catheter implantation using the Moncrief technique (MT), by which it is placed in a subcutaneous pocket with subsequent externalization (extrusion) at the start of peritoneal dialysis (PD), has been suggested in order to prevent premature tunnel and catheter colonization.
Methods: Retrospective analysis of 3 Italian dialysis units’ experience in MT at 2005 with special attention to complications and catheter functionality at extrusion Selection criteria were: not being on hemodialysis or anticoagulant therapy: not having an indication for surgical insertion; and a period of at least 4 weeks before start PD.
Results: 103 Tenckhoff catheters were implanted using MT in 103 patients (pts; 40 in Alba. 42 in Milano, 21 in Rieti). Mean age was 63±14 years, 28 pts were female (1) Intra-postoperative complications: 1 peritonitis with catheter removal and 1 abdominal pain that persisted after dialysis start. Other minor complications (resolved without extrusion or catheter removal) were hematoma in 4 pts, wound infection in 4 pts persistence of blood dialysate with channelization deferred by several days in 3 pts (Alba) In all cases, after insertion, the catheter requires no treatment (2) Extrusion: of the 103 catheters implanted, 96 were extruded within 139±131 (range 3-730, median 84) days of the insertion. Upon extrusion, catheter were removed in 7 pts 3 because occlusion or malfunction (extrusion time 730, 272, and 61 days), 2 because rupture (by needle), 1 for wound and tunnel infection with peritonitis, and finally in 1 pt with extended cysto-diverticula there was a perforation of the bladder (extrusion time 81 days).
In conclusion, the increased freedom in deciding when to insert the catheter (when the dialysis start date cannot be forecast) and the easier management of MT catheter, would seem to be further if not more important motives for applying this technique.
Nen L.1, De Vecchi A.2, De Martino A.3, Viglino G.1, Ospedale San Lazzaro,1 Ospedale Maggiore IRCCS di Milano,2 Ospedale di Rieti,3 Italy.
Systematic Peritoneal Dialysis (PD) Training: An Essential Component of a Successful PD Program
Background: Multiple factors have been shown to underlie the success of a chronic PD program. Systematic training of patients, and/or caregivers for patients incapable of self-dialysis, is an important but unreported component of a successful PD program.
Aim To describe the PD training program in our unit.
Program: All new PD patients receive 4 days of PD training following dialysis counseling and insertion of Tenckhoff catheters. Training is done by a dedicated PD nurse on a one-to-one basis. Components of the training include theoretical and practical sessions. Topics covered during the theoretical sessions include: introduction to functions of the kidneys and renal failure principles of PD infectious and noninfectious complications, fluid management, blood pressure and glycemic control, medications, and dialysis adequacy. Practical sessions emphasize sterility, exchange procedures, catheter care assessment and care of exit site, and documentation. Physical demonstration is carried out by the PD nurse with subsequent return demonstrations by the patient and/or caregiver. A session on nutrition is undertaken by a dedicated dietician. Patients are educated on maintenance of APD machines (where applicable), ordering of supplies, and storage of PD fluids. Common problems encountered at home during dialysis are highlighted and patients are equipped with appropriate problem-solving skills. The final day of training involves validation of the practical skills and evaluation of the competency level of patients and/or caregivers in PD.
Conclusion: Our renal unit has trained a total of 126 PD patients (65% CAPD, 35% APD) over a 5-year period. We are able to achieve good outcomes with technique survival of above 90% at 1-year and 2-years, and low peritonitis rates of 1 in 49.2 patient months Systematic PD training is an important component that has contributed to the success of our PD program.
Ng T.G., Tan S.H., Tay M. E., Mohamed E., Ngw K., Liew A.S.T., Chionh C.Y., van der Straaten J.C., Lye W.C., Renal Medicine Unit, Tan Tock Seng Hospital Singapore.
Uremic Encephalopathy with Particular Involvement of the Basal Ganglia
Background: In patients (pts) with end-stage renal disease, uremic encephalopathy Is a common comp cation expressed by affecting mainly cerebral cortex, in which specific morphological change was not usually observed Rarely bradykinetic movement with basal ganglia lesion are reported in uremic pt, often followed by favorable outcome. Here we described a diabetic pt receiving peritoneal dialysis (PD) who developed Parkinson an feature with both basal ganglia lesions in company with a deterioration of renal function and showed rapidly improving clinical course after enhancement of the dialysis adequacy. Case History: The pt is 18-year-old man with chronic renal failure due to focal segmental glomerulosclerosis, diabetes mellitus, hypertension during 4 years. He started the PD 4 months ago In January 2006, he was referred to our hospital for an acute-onset gat disturbance and dysarthria. Two weeks earlier he had been decreasing residual urine volume and increasing BUN and serum creatinine. At admission, neurologic examination demonstrated a Parkinsonian syndrome, characterized by resting tremor, bradykinesia, and postural balance disturbance. Cognition was normal. Laboratory data showed elevated BUN {66 mg/dL} and creatinine (10.6 mg/dL) but other blood chemistry results including serum osmolarity, thyroid and parathyroid function were normal reference range. Blood glucose and blood pressure were well controlled. MRI imaging revealed bilateral and symmetrical basal ganglia lesions with edema and increased vascularity; thereby lateral ventricles were compressed. T1-weighted scan showed hypointense areas in lenticular nuclei, where a T2-weighted images documented hyperintensity in same lesions and on PET imaging the decreased glucose metabolism was noted at both basal ganglia After frequency and dose of PD were increased bradykinetic movement and tremor were improved gradually and at 4 weeks follow up MR, previous basal ganglia lesions and edema were recovered markedly. Discussion The selective vulnerability of the basal ganglia is still poorly understood. The elevated variety of toxin and metabolites may be deranged the regional cellular metabolism and decreased the dopamine turnover. Also cerebral myogenic vasoconstriction may be lead cerebral autoregulation dysfunction, then to vasodilatation and focal hyperemia. These vascular and metabolic factors contribute the pathogenesis of basal ganglia lesions Conclusion Brain MRI or PET-imaging study were useful confirmatory diagnostic tool for uremic encephalopathy. And when uremic encephalopathy was developed, immediately we must have more effort for enhancing dialysis adequacy.
Oh J.M.1, Shin S.H.1, Choi J.H.1, Kim J.E.1, Kwon K.H.1, Yoon S.J.1, Park J.M.2, Seoul Medical Center,1 Osan Korean Hospital,2 Seoul, South Korea
The Changing Pattern of Peritoneal Dialysis Population in a U.K. Regional Renal Unit
The dialysis data of our regional peritoneal dialysis (PD) patients have been kept up-to-date by the same PD unit manager since 1990. We have retrospectively analyzed the changing pattern of our PD and hemodialysis (HD) patent group. Our PD population has increased gradually from 77 in 1990 to a peak of 155 in 1999 (PD:HD 2:5) then fallen steadily to 121 (PD:HD 1:5) by 2005 largely due to a decrease in new PD patients (48 in 2005 compared to 82 in 2001). Diabetic patients which made up 30% of the PD population in the early nineties has declined steadily to 15% and leveled off in the last 7 years More young people (90% <60) were doing PD in the late 1990s but 10% of our patients are >75 years old. In the U.K., the increase in PD population in the 1990s was mainly the result of lack of HD capacity. The relatively unrestricted use of cycler/automated peritoneal dialysis (APD) in our region towards the late 1990s (51% on APD in 1999) coincided with an increase in the younger patients on PD program (90% <60 years old). The increase in elderly patients on PD program has been made possible through the introduction of more user-friendly technology and cyclers. Large patients are no longer a contraindication to PD as >10% of our PD patients have BMI>31. Similar observation of falling PD:HD ratio has been observed in other parts of northwest of England. It appears that fewer younger patients are willing to consider PD given choice Given time and support older patients are able to achieve good outcome on PD therapy. Future planning of resources must ensure adequate staff and technology for the changing pattern of PD population
Pai M.C.P., Livesley P., Marshall L., Ahmad R., Bell G.M., Royal Liverpool University Hospital, Liverpool, United Kingdom.
Organization of Peritoneal Dialysis in Oppland County, Norway
European and American guidelines recommend that approximately one third of dialysis patients are treated by peritoneal dialysis (PD). This rate has proven difficult to achieve in areas where hemodialysis (HD) is well established, in Norway PD penetration rate is only 12%. The incidence of renal replacement therapy (RRT) in Oppland County (population 185000) is 140/million, with a PD penetration of 30%-35% over the last 10 years. During the last 5 years, 62 patients have been treated by PD; average age 68.8 years, range 27-87 frequency of peritonitis 1/29.3 per month, exit-site infection frequency 1/58.6 month. HD is well established, so all patients may be offered either treatment. We believe that the organization of PD in Oppland is the main reason for the high PD incidence. (1) all nephrologists in our department consider that PD is the best choice for many patients requiring dialysis. PD is substantially cheaper than HD, patients retain more residual renal function, and can achieve a flexible lifestyle (2) A PD nurse and a nephrologist inform all patients potentially eligible for PD, about the mode of treatment. (3) One surgeon is specialized in PD-catheter implantation. (4) Only motivated patients are commenced on PD treatment (5) Patients follow up by telephone calls and home visits (6) Adequate training of patients and home nursing/nursing homes (7) Dedicated program for commencement of acute PD (8) Adequate resources in home nursing and nursing homes to aid handicapped patients with bag changes. (9) Transition to other treatment in time.
Conclusion: A well functional PD-organization depends on an extensive cooperation within the hospital system and towards primary health care and nursing home systems.
Paulsen D.1, Kronborg J.1, Solbakken K.1, Valset T.2, Hogasen K.1, Aksnes H.1, Thorud L.O.1, Department of Nephrology,1 Department of Surgery,2 Sykehuset Innlandet Hospital, Lillehammer, Norway.
Survival Prediction from Hypoalbuminemia Level in CAPD Thai Patients
Background: Serum albumin is a strong predictor of outcome in patient with CAPD A serial data of albumin concentration overtime was obtained to determine the prevalence of a persistence of hypoalbuminemia and whether hypoalbuminemia was associated with mortality.
Methods: This was a retrospective review of 200 adult patients who were 1 year or longer survivors with CAPD. At our setting, follow-up visits were set for a periods of 1 to 2 months. Hypoalbuminemia during follow-up was defined as serum concentrations of less than 3.0 mg/dL for all first 4 consecutive routine visits The effect of hypoalbuminemia at baseline and during follow-up on mortality was examined using a Cox regression model adjusted far diabetes mellitus, technology advancement and important covariates.
Results: 71 patients (35.5%) had hypoalbuminemia at baseline. The prevalence of a persistence of hypoalbuminemia during the first 4 routine visits was 14.5% (29/200) Among those who had hypoalbuminemia at baseline. 22 of 71 (31%) patients still had hypoalbuminemia during these follow-up visits The median survival times were 29 months for those who had hypoalbuminemia during follow-up and 61 month far those who had not. Hypoalbuminemia during follow-up within the first year was significantly associated with increased risk of death by hazard ratio of 2.0 (95% Cl 1.05-3.82), whereas hypoalbuminemia at baseline was associated with an increased of death by 43% (hazard ratio 1.43, 95%CI 0.82-2.50).
Discussion & Conclusion: Hypoalbuminemia after receiving CAPD was still common and it strongly related to an increased risk of death. Interventions on nutritional supports should be focused.
Promajuk P.1, Limwatananon C.1, Johns J.1, Pongskul C.2, Sirivongs D.2, Clinical Pharmacy Dept,1 Faculty of Pharmaceutical Sciences. Division of Nephrology,2 Dept of Medicine, Faculty of Medicine Khon Kaen, Thailand.
Presence of Intra-Abdominal Complications Determine the Two-Year Outcome after Transfer from Peritoneal Dialysis (PD) to Hemodialysis (HD)
Because of the lack of specific information, clinical care and management guidelines for intra-abdominal (Intra-ab) complications of PD patients (pts) are not well established. We aimed to identify the risk factors that influenced the clinical outcome of pts after transfer from PD to HD including indication for transfer, presence of Intra-ab complications, medical and interventional treatment received. 24 pts (age 48.4±13.2 years, M/F 17/17, PD duration 32.0±23.5 months, follow-up period alter HD 38.8±22.5 months) first 2 years follow-up data during and after termination of PD were analyzed Pts’ peritoneal fluid evaluation results and demographic laboratory, radiological (computerized tomographic and/or ultrasonographic examination of abdomen) data, hospitalization rates and durations were recorded. The reasons for the transfer were peritonitis (30%), mechanical problems (32%), and ultrafiltration failure (38%). During the transfer, 12 pts had Intra-ab loculated fluid collection and 9 had Intra-ab free fluid (group I) while 13 pts had no Intra-ab complication (group II) According to the 1st year data. Intra-ab collection was observed in 11 pts, 7 of whom had received percutaneous drainage. At the end of the 2nd year, 4 pts still had Intra-ab collection In group 1, 1 pt died in the 1st and 4 in the 2nd year, whereas no deaths were recorded in group II. When group I was concerned, these pts exhibited significantly lower albumin (p<0.01), higher CRP levels (p<0.02), and erythropoietin resistance at the time of transfer. During the 1st year there was tendency for an increase in albumin, decrease in CRP levels in this complicated group, but still there were significantly differences between 2 pt groups at the end of the 1st year. Group I patients had significantly more frequent and longer duration of hospitalization (p<0.001 and p<0.01). In conclusion, presence of Intra-ab complications is associated with adverse nutritional and inflammatory impact in pts transferred from PD to HD. Multidisciplinary approach is needed for improved outcomes.
Sezer S., Bilgic A., Nurhan Ozdemir F., Sasak G., Arat Z., Haberal M., Department of Nephrology Baskent University Faculty of Medicine, Ankara, Turkey
Percutaneous and Surgical technique of CAPD Catheter Insertion: A Comparison of Outcome and Complications
Background: Several techniques of catheter (C) insertion are being currently practiced with open surgical approach being the most common. Few studies have compared PGW (PGW) technique of Tenckhoff catheter insertion (TCI) with the surgical technique. Methods: We analyzed 479 double-cuffed TCIs in 471 patients (pts) either by surgical (dissection] method by nephrologists (group 1:62 catheters with a cumulative experience of 733 pt-months) and by surgeons (group 2:335 Cs with a cumulative experience of 3593 pt-mos) or by PGW method by nephrologists (group 2: 82 Cs with a cumulative experience of 1453 pt-mos) between January 2002 and November 2004. The data were analyzed far surgical and nonsurgical complications, and C outcome along with lag time between decision and insertion. Results: The incidence of C-related (mechanical and infectious) complications did not differ between the percutaneous (nephrologist, group 2) and surgical technique by surgeons (group 3). (1 episode in 104 pt-mos vs 1 epi in 39 pt-mos.), although with mild significant difference (p=0.077): although there was significantly higher mechanical complications in surgical technique (group 3) (p<0.05) with no difference in C-related infectious complications when compared to percutaneous technique. However, there was no significant difference in overall C-related arid mechanical complications when surgical technique was used by surgeons or nephrologists, cut a significantly higher early C-related infections in surgical technique used by nephrologists (p<0.001). There was significantly higher overall C-related and infectious complications when percutaneous technique was compared to surgical technique by nephrologists(P<0.005); but no significant difference in mechanical complications The incidence of C-related early infections were 1 epi in 43 pt months. 1 ep in 161 pt months, 1 epi in 89 pt-mos. In all 49 Cs (10.2%) were removed either due to mechanical or early infectious reasons. There was no significant difference in C removal when the groups were compared However, when death with C in situ was included in the analysis, there was significantly higher C loss in both surgical techniques when compared to percutaneous technique. There was significantly higher lag time between decision for CAPD C insertion and actual Procedure when surgical technique was used by the surgeons 6.1±1.96 days compared to group 1 (4.5±1.6 days) and group 2 (4.1±1.6 days), p<0.001. The overall C survival and pts continuing on CAPD were significantly higher in percutaneous group when compared to surgical group when death with C in situ was also included in analysis (log rank analysis p=0.001), but no significant difference when death with C in situ was excluded (p=0.12). Conclusions: With good technical expertise, PGW C insertion is reliably safe in terms of low mechanical complications and a better C survival and an earlier catheter insertion avoiding unnecessary delays Thus, nephrologists can safely practice the Wind PGW technique for CAPD TCI.
Sharma R.K., Somayajulu D.V.S., Gupta A., Gulati S., Kumar A., Prasad N., Sanjay Gandhi Post Graduate Institute of Medical Sciences Lucknow, India.
Continuous Ambulatory Peritoneal Dialysis (CAPD) in Nepal: Opportunities and Challenges
The options for renal replacement therapy (RRT) are limited in Nepal Most patients with end-stage renal disease (ESRD) recede hemodialysis, which are largely located within the capital of country, and renal transplantation is yet not available CAPD was started in 2002 in B P Koirala Institute of Health Sciences, a teaching university hospital in eastern Nepal. A total of 29 patients were enrolled in the program until 2004. We present initial experience barrier for development of CAPD service, and possible opportunities for the growth of CAPD in Nepal.
Patient Profile Mean age of the patients was 62±14 years. Majority had diabetes (n=20). The overall incidence rate of peritonitis was 0.43 episodes per patient-year. Staphylococcus aureus was the most common organism Isolated and 1/3 developed culture sterile peritonitis. Four patients dropped out from therapy due to financial reasons. One patient switched over to hemodialysis. Ten patients died (cerebrovascular disease 5, peritonitis 1, sepsis 2, others 2).
CAPD Service Only 1 center routinely councils the patients for CAPD as option for treatment of ESRD It has been person dependent rather than center. Major barriers in the development of CAPD in Nepal are limited expertise, physician's bias towards hemodialysis, and lack of predialysis counseling. On the other hand because of remoteness of hemodialysis centers, and the cost of setup being higher for hemodialysis. CAPD is likely to be better choice over hemodialysis in Nepal This initial experience on CAPD is encouraging and can be use to build up CAPD program in Nepal. For the growth of CAPD in Nepal we recommend creating awareness among physicians on CAPD thorough physician education, expertise development, and proper predialysis counseling of patients.
Sharma S.K.1, Manandhar DN.2, Shrestha N.R.1, Regmi R.1, Agarwal R.1, Adhikary S.1, B.P. Koirala, Institute of Health Sciences,1 Dharan; Nepal Medical College, Kathmandu,2 Nepal.
Outcomes of CAPD Patients and Hemodialysis Patients who Were Undergoing Kidney Transplantation: A Matched Case Study
Objective: Kidney transplantation (KT) is the ideal therapeutic modality for end-stage renal disease (ESRD) patients. In our facility KT was performed in both CAPD and KT patients however, it was unclear whether different dialytic modalities could affect the outcome So, to evaluate the influence of dialytic modality on the outcome in our facility, we conducted this study.
Methods: Medical records of CAPD patients who were undergoing KT were reviewed. By matching for age, gender, and timing of KT operation, KT cases who were on hemodialysis (HD) before the operation were recruited in the ratio 2:1 Clinical data of both matched group were analyzed Analyses were performed with the SPSS statistical data program. Also survival analysis was studied by Kaplan-Meier method
Results: Since 1990, 231 KT operations were performed in our hospital. 26 KT adult patients who had been treated with CAPD (CAPD group) for 4-107 months (39.6±24.5 mos) were compared with 52 KT patients who had been treated with HD (HD group) for 2-110 mos (29.7±25.7 mos) Regarding the immunosuppressive agents, we used 2-drug regimen far living related KT & 3-drug regimen for cadaveric KT in both groups The mean hospitalized duration in CAPD group versus HD group was 36.2±30.2 days vs 30.9±15.3 days Acute allograft rejection during post-operation period was comparable between CAPD and HD groups (2 episodes, 3 episodes). Even actuarial graft survival compared between CAPD with HD was 96% vs 98% at 1 year and was 40% vs 23% at 5 years, anyway there was no significant difference between the 2 groups (p=0.3). Urinary tract infection was found in high frequency in both CAPD and HD groups (38.5% 40.4%).
Conclusion: There were no significant differences between the 2 groups on graft survival, incidence of acute allograft rejection and complications Therefore CAPD is a suitable modality for patients awaiting KT.
Sirivongs D., Toimamueang U., Pongskul C., Chunlertrirth D., Renal Replacement Therapy Program Srinagarind Hospital. Faculty of Medicine. Khon Kaen University, Khon Kaen, Thailand.
Serum Cytokine Profile in Chronic Hemodialysis Patients and CAPD Patients Determined by Biochip Array Technology
Background: Uremic patients demonstrate impaired immune response which is related to high morbidity and mortality due to infections. Through contact between blood and dialyzer membrane, hemodialysis (HD) itself induces proinflammatory cytokine secretion, depending on the type of membrane. CAPD solutions can also induce immune response. The aim of the study was to determine the difference in immune response between HD and CAPD patients.
Materials and Methods: Interleukin (IL)-2, IL-4, IL-6, IL-8, IL-10 and ferritin were determined in the sera of 35 patents on chronic HD and 15 CAPD patients by using biochip array technology. The patients showed neither clinical nor laboratory signs of acute or chronic infection. The number of leukocytes in the dialysate was normal, as well as dialysate cultures HD patients were dialyzed using polysulfonic membranes, while blood samples were collected prior to HD inclusion. Patients on peritonea dialysis were dialyzed using conventional glucose solutions by Fresenius and Baxter companies Patients from both groups had negative results on hepatitis B and C markers. Dialysis (HD and CAPD) was performed for more than 3 months
Results: Both patient groups were comparable with regard to age, gender, and erythropoietin administration. No significant difference was found for IL-2, IL-4, IL-6, IL-8, and IL-10 in the sera of HD patients compared to CAPD patients. The only significant deference between the groups was established for ferritin values. HD patients had significantly higher ferritin values (p=0.0002).
Conclusion: As methods of renal replacement therapy. HD and CAPD equally stimulated cytokine production.
Slavicek J.1, Sertic J.2, Bozina N.2, Smalcelj R.1, Kes P.1, Dialysis Department,1 Center for Functional Genomics.2 UHC, Zagreb, Croatia.
An International Encapsulating Peritoneal Sclerosis Registry and DNA Bank. Why Do We Need One Now?
Peritoneal dialysis (PD) is a successful treatment modality for endstage renal failure and has seen universal application over the last 20 years. The complications of prolonged PD therapy have become more evident in the last decade with more patients experiencing long-term therapy. One of the most serious complications of PD is the development of encapsulating peritoneal sclerosis (EPS). The incidence of EPS has been variably reported as between none (in a 10-year period), to as many as 4.2/1000 patient years. In recent data from Japan, where renal transplantation is less common and duration on dialysis usually longer, the incidence and mortality rates of EPS increased with time on PD, ranging from 0% at 3 years, to 5.8% at 10 years, to 17.2% with 100% mortality in patents on PD for over 15 years. While the importance of EPS has been recognized in Japan through collection of registry data, it has clearly becoming a major issue that impacts on PD worldwide and deserves global attention. From the literature there are no validated guidelines for the diagnosis, treatment, and management of EPS. Given that only a small percentage of patients on PD develop EPS it is possible that, in addition to dialysis ‘exposure,’ genetic factors may predispose certain individuals
The aim is to enroll a number of international centers to collect a specific data set designed to address all clinical aspects of EPS. This project will interface with other studies such as GLOBAL and JFS which have pioneered prospective observational studies in PD. DNA will be collected from consenting patients and stored for future research on genetic associations with EPS. It is important to recruit a large number of centers worldwide to give statistically power Understanding the genetic component to EPS could lead to new therapies and influence clinical management.
Summers A.M., Brenchley P.E.C., Brown E.A., Davenport A., Davies S., Fan S., Hutchison A. J., Junor B., Topley N., Wilkie M., Williams P., Woodrow G., UK EPS Study Group, United Kingdom.
Outcome of CAPD Patients who Were Undergoing Kidney Transplantation in a Thai Medical Center
Objective: Our facility provides all therapeutic modalities for end-stage renal disease cases, and the major modality is CAPD. Since 1990, 231 kidney transplantation (KT) operations were performed and CAPD was a pre-KT modality in 26 cases. To analyze clinical outcomes of CAPD patients who were undergoing KT, we conducted this study.
Methods Medical records of CAPD patents who were undergoing KT were reviewed. Demographic and clinical data were analyzed. Also survival analysis was study by Kaplan-Meier method using SPSS program.
Results: 26 CAPD patents received allograft kidney from 3 living related and 23 cadaver donors. Male:female–2.25:1.0, mean age was 45.2±5.5 years. 69.2% cases had educational status above grade 12. Most of them received supports from the government. Mean duration on CAPD was 39.35±24.5 months (range 4–107 months). Dialysis was necessary in postoperative period in only 15.4% cases. No postoperative complications related to CAPD were detected The mean hospitalized duration was 36.2 days Anyway, urinary tract infection was found in 38.5% but it responded to treatment Acute allograft rejection was found in 2 cases, but it was successfully treated. Actuarial graft survival at 1 year and 5 years was about 96% and 42.3%, respectively.
Conclusion: Clinical results and outcome of CAPD patients who were undergoing KT were quite good, so CAPD is a suitable treatment for patients awaiting kidney transplantation as well as hemodialysis.
Toimamueng T., Pongskul C., Chunlertrith D., Sirivongs D., CAPD Program, Srinagarind Hospital, Faculty of Medicine, Khon Kaen University Thailand
Plasma S100A12 Concentrations in Peritoneal Dialysis Patients and Association with High Peritoneal Solute Transport Rate
Objectives: S100A12 is a ligand for the receptor for advanced glycation end products. It has been shown that S10OA12 induces expression of adhesion molecules and mediates activation and migration of monocytes/macrophages. Therefore, circulating S100A12 may be involved in chronic inflammation. We previously reported increased S100A12 levels in patients with non insulin-dependent diabetes mellitus and in patients undergoing hemodialysis. A high peritoneal solute transport rate (HPSTR) may be associated with encapsulating peritoneal sclerosis and mortality. In this study, we measured plasma S100A12 levels in patients undergoing peritoneal dialysis (PD), and evaluated possible relation between S100A12 and HPSTR.
Methods: Subjects included 45 patients (mean age±SE, 46.0±12.0 years) with no apparent inflammation and no malignancy, who had been undergoing PD for 36.5±3.9 months (range). We developed an enzymelinked immunosorbent assay system to measure plasma S10012 levels A peritoneal equilibrium test was performed and subjects were categorized as high and high-average (H) (n=15) or low and low-average (L) (n=26) transporters.
Results: Plasma S100A12 concentrations were significantly higher in PD patients (21.6±3.0 ng/mL) than in control subjects (n=42; 10.8±1.0 ng/mL).We previously measured plasma S100A12 concentrations in hemodialysis patients (19.2±2.8 ng/mL), and there was no significant difference compared to in PD patients Plasma S100A12 concentrations were also higher in the H group (282±6.1 ng/mL) than in the L group (142±2.0 ng/mL).
Conclusions: These results suggest that S100A12 may be an acute inflammatory marker and also a sensitive marker of subclinical inflammation and HPSTR.
Uchiyama-Tanaka Y.1, Mori Y.2, Kosaki A.3, Kimura T.4, Moriishi M.5, Kawanishi H.5, Matsubara H.2, Takeda Hosp.1 Kyoto Prefect Univ of Med,2 Kyoto: Kansai Med Univ,3 Osaka: Adv Life Sci Inst,4 Saitama; Akane-Found'n Tsuchiya Hosp,5 Hiroshima, Japan.
May Patient Preference Affect Peritoneal Dialysis Outcome
Peritoneal dialysis (PD) seems an alternative renal replacement therapy for patients who could not have been hemodialyzed because of vascular access or other problems. It is considered that the clinical outcome of these patents might be worse than patients who choose the treatment on their self-preference, however there is not enough data on this topic. We aimed to determine the effect of patient preference on clinical outcome on PD, by evaluating the patients who choose PD with their preference, and who are obligated to make if for some reasons. 168 patients starting PD in our unit during December 2001 to June 2005 were evaluated retrospectively. 136 of them (group 1) chose the treatment, while 32 patients (group 2) were obligated to do PD. While 22 of group 1 patients died (group 1a; 9 F, mean age 47±17 years, mean follow-up time 9.9±7.9 months), 114 patients (group 1b; 56 F, mean age 40±14 years, mean follow-up time 19.3±12.3 months) are under follow-up. In group 2 patients 11 died (group 2;: 8 F, mean age 59±15.3 years, mean follow-up time 6.3±52 months), while 21 patients (group 2b. 15 F, mean age 48±19.5 years, mean follow-up time 17.2±11.6 months) are under follow-up Clinical and metabolic parameters of all patients were evaluated at the beginning of PD and at the end of follow-up period Data of the 2 groups, both living and dead were compared. Mean age, hemodialysis period, and hypertension of group 2a patients were higher than other groups (p=0.001, p=0.036, and p=0.001, respectively). Mortality was higher in group 2 than group 1 (odds ratio: 3.3, p=0.006). Peritonitis rate was higher in group 2a than both groups 1a and 1b (p=0.016, p=0.032). While initial and final data of groups 1a and 2a were not different (p>0.05), only Hb and SBP changes were significant in groups 1 b and 2b (p=0.001, p=0.02). In conclusion, despite patients who were obligated to do PD experience more frequent peritonitis attacks, and have less diuresis no difference is demonstrated in terms of clinical and metabolic parameters, compared to the patients who voluntarily perform PD. Mortality of patients who were obligated to undergo PD were associated with age, baseline RRF, CTI, albumin levels, hypertension and prior duration of hemodialysis.
Unsal A.1, Koc Y.1, Sakaci T.1, Yetkin G.2, Ahbap E.1, Basturk T.1, Yilmaz M.1, Gurdal A.1, Sislietfal Hospital Clinic of Nephrology,1 Sisli Etfal Hospital Clinic of General Surgery,2 Istanbul, Turkey.
Risk Factors for Late Peritoneal Leakage in PD Patients
Subcutaneous leakage iron the catheter exit site is a rare but important complication of peritoneal dialysis (PD). We investigated the incidence of late peritoneal leakage and the potential risk factors, retrospectively 258 (138 females mean age 43.1±15.6) followed up at cur PD unit were included in the study. Technique of peritoneal catheter insertion was Seldinger method in 175 patents (pts) (67.8%), surgical method in 71 pts (27.5%), and laparoscope method in 12 pts (4.7%). Pts were followed up for a total of 532.8 pt-years and a mean of 24.8±20.9 months. 202 pts (78.3%) applied continuous ambulatory PD (CAPD), 19 pts (7.4%) applied automated PD (APO) whereas both treatment modalities were applied in 37 pts (14.3%). The association of late leakage with age, gender primary cause of renal disease, height, body weight body surface area (BSA), body mass index (BMI), type of peritoneal transport and the method of peritoneal catheter insertion were investigated 16 leaks were detected in 12 pts (4.7%, 10 F, mean age 39±14), with multiple leaks occurring in 3 pts. Three pts had hernia. Leakage occurrence period was 27±24 (5-91) months. 12 of 16 leaks (75%) were observed in the CAPD and 4 (25%) were observed in the APD period. No leakage was detected in the pts who applied APD only. The clinical findings were swelling at exit site, edema in the subcutaneous tissue, and impaired drainage in some pts The diagnosis was confirmed by abdominal tomography in 9 pts. In 11 of 16 leaks, pts were temporarily switched from PD to hemodialysis for 1 month. For the other 5 cases, low-volume APD was employed The symptoms resolved in 1 week with both treatment methods None of the pts with leakage required catheter removal or surgical intervention. No significant d iterance was detected between the pts with and without leakage in regard to age, primary cause of renal disease, BSA, or BMI (p>0.05). The occurrence of leakage was found to be significantly higher in female pts (p<0.05). In pts without leakage mean height and mean body weight were 162±9 cm and 62±14 kg, respectively, whereas these values were 156±7 cm and 52±12 kg respectively, for those with leakage. The difference was significant (p<0.05). No difference was detected in regard to the type of peritoneal transport (p=0.43). Leakage was observed significantly more in pts in whom peritoneal catheter was inserted via laparoscopic method (p=0.014). In conclusion, the incidence of leakage was observed to be higher in CAPO pits compared to APD pts. Females, short and thin pts, and rose in whom peritoneal catheter was inserted via laparoscopic method had a higher risk for leakage, and that employing low-volume APD would be effective in the treatment of pts with leakage, rather than shifting to hemodialysis.
Unsal A., Yilmaz M., Koc Y., Ahbap E., Basturk T., Sakaci T., Salter T., Cagatay P., Ozel A., Basak M., Nephrology,1 Sisli Etfal Hosp; Statistics,2 Cerrahpasa Medical Faculty; Radiology,3 Sisli Etfal Hosp, Istanbul, Turkey.
The Risk Factors for Hernia in Peritoneal Dialysis Patients
Hernia results from Increased intra-abdominal pressure in peritoneal dialysis (PD) patients (pts) We retrospectively investigated the incidence and potential risk factors of hernia in our PD pts, 258 pts (138 females, mean age 43.1±15.6) followed up at our PD unit were included in the study Peritoneal catheter was inserted via Seldinger method to 175 pts (67.8%), surgical method to 71 pts (27.5%), and laparoscope method to 12 pts (4.7%). Pts were followed up for a total of 532.8 pt-years and a mean of 24.8±20.9 months, 202 pts (78.3%) underwent continuous ambulatory PD (CAPD), 19 pnts (7.4%) underwent automated PD (APD) whereas both treatment modalities were employed in 37 pts (14.3%). Pts were investigated with respect to presence of association between hernia formation and the age, gender, primary cause of renal disease, body surface area (BSA), body mass index (BMI), type of peritoneal transport, and the method of peritoneal catheter insertion. Hernia was detected in 25 pts (9.7%, 15 F, mean age 45±16) Hernia formation was only observed in CAPD pts. It exhibited umbilical and inguinal localization, and incisional region at the peritoneal catheter access site in 17 (68%), 7 (28%), and 1 pt (4%), respectively. 16 pat with hernia (64%) were still under follow-up while 9 pts underwent surgical intervention (36%). Post operatively 8 pts were shifted to hemodialysis for 1 month and low-volume APD was performed in 1 pt for the same period of time. No postoperative complications developed in any of the pts No significant differences were detected between the pts with and without hernia with respect to age, gender, primary cause of renal disease, and BSA (p>0.05). However, mean BMI was 23±4.4 in pts without hernia and was 25±58 with hernia (p<0.05). According to BMI (thin, normal weight, overweight and obese), hernia was commonly observed in obese pts (p=0.05). No difference was detected in hernia formation by the type of peritoneal transport based on PET test (p=0.078). No significant deference was detected in hernia formation by the method of peritoneal catheter insertion (p=0.55). It was concluded that the incidence of hernia was detected to be higher in CAPD pts compared to APD pts and that the risk of hernia was increased in obese pts.
Unsal A.1, Yilmaz M.1, Ahbap E.1, Sakaci T.1, Koc Y.1, Basturk T.1, Salter T.1, Cagatay P.2, Yetkin G.3, Akgun I.3, Nephrol,1 Sisli Etfal Hosp; Statistics,2 Cerrahpasa Medical Faculty; Surgery,3 Sisli Etfal Hosp. Istanbul, Turkey
Our Experience of CAPD
Out of 3 modalities of renal replacement therapy (RRT) for the patients (pts) with end-stage renal disease (ESRD)–renal transplantation, maintenance hemodialysis (MHD), and CAPD–CAPD was underutilized in the region of Saurastra and Kutch in India. We have started the first CAPD in the region and to date we have started CAPD in 21 ESRD pts during last 3 years Mean age of the pts is 44±16.97 years (youngest 7 years and oldest 82 years), male female ratio is 19:2. Total 265 pt-months completed until end of February 2006. Maximum duration of CAPD in single pt in the study is 36 months Of 21 pts, 2 have undergone renal transplantation in past and had graft dysfunction. 7 pts had associated ischemic heart disease Low cost of the treatment in lifelong scheme compare to MHD is also a contributing factor for selection of the treatment in many pts Mean S. albumin in these pts 2.65±0.53 mg/dL, mean hemoglobin is 9.4±0.7 g/dL. Peritonitis rate is 11 pt-months/episode. 13 pts developed bacterial peritonitis. One had fungal peritonitis required removal of catheter and was put on MHD. All the pts who developed peritonitis had low serum albumin. 7 pts died during study period (3 had peritonitis 1 had myocardial infarction 1 had diabetic foot and sepsis, 1 had progression of chronic myeloid leukemia, and 1 had multiorgan dysfunction). All the pts who died during study period had low S. albumin. This study concludes that CAPO is a good option for RRT specifically for those who are staying tar from dialysis center, not tolerating HD, extremes of age and pts having no vascular access and it reduces the cost of the RRT. S. albumin and peritonitis are prognostic indicator for long-term viability of CAPD.
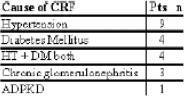
Viroja D.M., Limbasia A.D., Moteria S.B.T., Savani Kidney Hospital, Rajkot India
Evaluation of Medication Sinomenium acutum in Hs-CRP Level Variance in Peritoneal Dialysis Patients
Objective: To evaluate the result of high-sensitivity C-reactive protein (Hs-CRP) level on peritoneal dialysis (PD) patients after medication Sinomenium acutum therapy
Methods: 20 patients were selected in this study from PD center in PUMC Hospital, all patients were no infective disease no trauma no operation in recent months, and Hs-CRP level >3.0 mg/dL. We compare the difference of Hs-CRP level after 6 months medication Sinomenium acutum (20 mg t.i.d.) therapy. According to variances of Hs-CRP level, we separate the patients into 2 groups: Hs-CRP decease <50%; Hs-CRP decrease >50% groups and compare the difference. We separate the patients into 2 groups by if the PD time is less than 4 years or not, and compare the difference of 2 groups.
Results: 1 patient suffered from rash 3 days after medication, 1 patient hypotension, and they all stopped medicine. 18 patients have taken medicine for 6 months. There are 8 males and 10 females, average age (63.4±10.1) years. After half a year Sinomenium acutum medication, the Hs-CRP level is more less than before (4.0±2.3 mg/dL, 7.7±3.1 mg/dL, p<0.001). 11 patients Hs-CRP decrease >50% and 7 patients Hs-CRP decrease <50%, The PD time is shorter in Hs-CRP decrease >50% group than in Hs-CRP decease <50% group (21.7±10.2% vs 70±39.6%, p=0.003). 11 patients PD time is less than 4 years and 7 patients more than 4 years, they had significant difference of Hs-CRP level variance among the 2 groups [(-66.2±20.1)% vs (-28.2±29.6)%,p=0.005)] Logistic regression analysis showed that the medication and shorter PD time are associated with Hs-CRP level decrease.
Conclusion: Sinomenium acutum medication are safe in PD patients. Hs-CRP level can decrease after Sinomenium acutum medication.
Xu H., Bi Z.Q., Zhou Z.J., Peking Union Medical College Hospital, Beijing, China
Restoration of Peritoneal Integrity after Peritoneal Dialysis Withdrawal and the Characteristic Features of Patients at Risk for Encapsulating Peritoneal Sclerosis
The epidemiological characteristics of encapsulating peritoneal sclerosis (EPS) such as high incidence in patients with long-term peritoneal dialysis (PD) treatment and onset of EPS after being switched to hemodialysis (HD) may indicate an activated pathological process after PD withdrawal, especially in long-term PD patients. Accordingly, we aimed to observe the change of peritoneal function after stoppage of PD, and to clarify the characteristic features of the patients at risk for EPS.
Patients and Methods: 33 patients who were switched from CAPD to HD were enrolled into this trial, the changes of dialysate/plasma creatinine (D/P Cr) and CA125 levels in the effluent of peritoneal equilibration test were observed for 6 months furthermore, the development of EPS was followed up to 36 months after PD withdrawal in each case.
Results. D/P Cr decreased significantly, while CA125 levels tended to increase. Nine patients developed EPS during the follow-up period and they specifically showed significant increase of D/P Cr levels and significant lower levels of CA125 at PD withdrawal The accumulation of high transporter in the EPS group at 0 and 6 months after PD withdrawal was significant.
Conclusion: Peritoneal recovery may take place after withdrawal from PD treatment and it is indicated by improvement of transport states and rise of CA125 levels. The present study revealed that high transport state and lack of increase of CA125 in the effluent were associated with EPS development after PD withdrawal This may suggest that the lack of peritoneal recovery after PD is predictive for EPS development.
Yasushi O., Masaaki N., Masato I., Ali M. S., Keitaro Y., Hiroyasu Y., Yoshindo K., Tatsuo H., Division of Kidney and Hypertension, Department of Internal Medicine, Jikei University School of Medicine. Tokyo, Japan.
High Serum β2-Microglobulin is a Significant Risk Factor for Encapsulating Peritoneal Sclerosis in Japanese Peritoneal Dialysis Patients
Objectives: Encapsulating peritoneal sclerosis (EPS) is a serious complication for peritoneal dialysis (PD) patents. The pathophysiology of EPS is thought to be related a peritoneal inflammation and sclerosis, however that is still obscure. If we can find risk factor for EPS, PD patients with high risk factor must be avoided prolongation of PD treatment. The aim of this study was to determine the useful maker for the occurrence of EPS.
Methods: In this historical cohort study, we recruited 21 EPS patients (mean age 56 years, mean PD duration 8.8 years, male/female 16/5) and 45 age- and gender-matched PD patients without the history of EPS The clinical data analyzed age, gender, underlying disease, duration of PD, serum urea nitrogen, serum creatinine, serum β2-microglobulin (β2-MG), serum CRP, volume of urine, and a PET category at the time of change to hemodialysis (HD) from PD.
Results: Compared to control group a PD duration was significantly longer and PET category was higher permeable. In addition, serum β2- MG level was significantly higher in the EPS group. On the other hand, there were no differences in age, gender, underlying disease, serum urea nitrogen, serum creatinine, serum CRP Serum β2-MG level of EPS group was higher than that of control group significantly in 1 year before to change in HD from PD According to receiver operator characteristic (ROC) curve, the cutoff value of the serum β2-MG was 31.8 (sensitivity 0.89, specificity 0.56, area under curve 0.775, p<0.01)
Conclusion: High serum β2-MG level might be an available marker for the occurrence of EPS independent for small molecule clearances and acute inflammation. And β32-MG level was suitable as screening examination of the occurrence of EPS.