
Abstract
Background
Fluid and sodium removal is often inadequate in peritoneal dialysis patients with high peritoneal solute transport rate, especially when residual renal function is declining.
Method
We studied the effects of using simultaneous crystalloid (glucose) and colloid (icodextrin) osmotic agents on the peritoneal transport of fluid, sodium, and other solutes during 15-hour single-dwell exchanges using 3.86% glucose, 7.5% icodextrin, and a combination fluid with 2.61% glucose and 6.8% icodextrin in 7 prevalent peritoneal dialysis patients with fast peritoneal solute transport rate.
Results
The combination fluid enhanced net ultrafiltration (mean 990 mL) and sodium removal (mean 158 mmol) compared with 7.5% icodextrin (mean net ultrafiltration 462 mL, mean net sodium removal 49 mmol). In contrast, the 3.86% glucose-based solution yielded negligible ultra-filtration (mean -85 mL) and sodium removal (mean 16 mmol). The combination solution resulted in significantly improved urea (+41%) and creatinine (+26%) clearances compared with 7.5% icodextrin.
Conclusion
A solution containing both crystalloid (glucose 2.61%) and colloid (icodextrin 6.8%) osmotic agents enhanced fluid removal by twofold and sodium removal by threefold compared with 7.5% icodextrin solution during a dwell of 15 hours, indicating that such a combination solution could represent a new treatment option for anuric peritoneal dialysis patients with high peritoneal solute transport rate.
The importance of fluid management in the clinical outcome of PD patients was highlighted in several recent papers (1-6). Ates et al. (2) demonstrated that both fluid and sodium removal were independent predictors of death in a cohort of PD patients during 3 years. Medcalf, Harris, and Walls (7) showed that, over the course of 1 year, urinary output and urinary sodium excretion declined by an average of 30% in new patients starting PD. Tzamaloukas et al. (4) highlighted the importance of patient noncompliance with respect to dietary restrictions and prescribed PD schedules as the major predictor of fluid retention. The European APD Outcome Study (EAPOS) (8) in anuric patients treated with automated PD (APD) demonstrated the importance of achieving adequate peritoneal ultrafiltration (UF) targets in anuric PD patients. As expected, PD patients, especially those with high or high-average peritoneal solute transport rates, are most likely to benefit from new strategies designed to optimize peritoneal net UF (9,10). Restricting fluid and sodium intake in anuric patients with inadequate fluid and sodium balance may not be enough, and therefore new PD options are needed to ensure adequate water and sodium removal.
Thus, there is a need to find better strategies to increase water and sodium removal in patients with loss of UF capacity. The growth in the numbers of patients on APD, along with the introduction of novel osmotic agents currently represented by glucose polymer-based (icodextrin) dialysis fluid (11), has increased the interest in new methods for achieving better fluid and sodium balance in APD patients.
In APD, the rapid short-dwell exchanges may contribute to an improvement in fluid removal, which should result in better cardiovascular outcomes. However, this is at the expense of a too high energy load due to rapid glucose absorption, and a permanent and potentially harmful exposure of the peritoneal membrane to hyper-tonic solutions.
The most problematic aspect of current APD schedules is related to the fast resorption of the crystalloid osmotic gradient during the long daytime exchange. The introduction of icodextrin provides an alternative mechanism for UF by colloid osmosis, which most likely also results in enhanced solute clearances, particularly in the middle molecular weight range. Yet, although icodextrin-based UF may improve volume balance in PD-treated patients (12), there is still a high incidence of fluid overload syndrome, hypertension, and congestive cardiac failure in this population, which calls for further progression in the therapy.
The aim of the present study was to investigate, in detail, fluid and solute transport using a combination PD fluid with both icodextrin and glucose during the long dwell exchange. A secondary aim of this study was to investigate whether the sodium sieving that characterizes short-dwell APD may be reduced using the combination fluid. Following previous studies (13-15) investigating a combination dialysis fluid with both crystalloid and colloid osmotic agents to increase simultaneously the dialytic extraction of water and sodium during regular long dwells, the current study focused on the kinetics of fluid and solute transfer using combination fluid during a long (15 hours) dwell exchange.
Patients and Methods
Patients
Seven stable patients (5 females, 2 males) who had been on APD for more than 12 months (median 19 months, range 13 – 45 months) were invited to participate in the study. Written informed consent consistent with the Declaration of Helsinki was obtained from each patient. The study was approved by the Ethics Committee at the University of Caen, France. Their mean age was 72 years (range 55 – 82 years), mean body weight was 75 kg (range 66 – 88 kg), and median body surface area was 1.89 m2 (range 1.70 – 1.98 m2). Their RRF as assessed by creatinine clearance was 5.3 mL/minute (range 0 – 10.8 mL/minute), and 24-hour urine volume was 572 mL (range 0 – 1270 mL).
The underlying chronic kidney disease was diabetic nephropathy (n = 2), nephrosclerosis (n = 3), renal amyloidosis (n = 1), and graft rejection (n = 1). Peritoneal transport characteristics, obtained from the measurement of the dialysate-to-plasma concentration (D/P) of creatinine and the dialysate-to-initial concentration (D/D0) of glucose at 4 hours of a dwell using 3.86% glucose-based dialysis fluid, showed a fast transport pattern with mean D/P creatinine 0.79 (range 0.67 – 0.95) and mean D/D0 glucose 0.24 (range 0.22 – 0.33).
Study Protocol
The protocol was designed as a single-dwell exchange study. The 7 included patients were assigned to three 15-hour PD sessions using, alternatively, 2 L hypertonic glucose-based dialysate (3.86% glucose; 3.86% Dianeal; Baxter Healthcare, Castlebar, Ireland), or glucose polymer (icodextrin) solution (7.5% icodextrin; 7.5% Extraneal; Baxter), or a combination fluid containing a mixture of the crystalloid and colloid osmotic agents in a single mixed PD fluid [referred to as “combination fluid” or, in Table 2 and the Figures, as “combination icodextrin and glucose” (CIG)]. The composition of that third solution is shown in Table 1. The dialysis fluids were administrated in random order. No volume marker was used during this study. Instead, in order to assess the UF volume-over-time profile, and the instantaneous clearances and total mass transfer of solutes (sodium, urea, creatinine, phosphate, glucose, and total protein) for each of the dialysis fluid formulations, a procedure with repeated complete drainage of the dialysate followed by reinfusion of the effluent was performed at 0, 2, 4, 8, 12, and 15 hours during the dwell period. Thus, the effective dwell time was slightly shortened due to the time required for drainage and reinfusion. The drained fluid was weighed and dialysate samples were taken before reinfusion. A blood sample was taken at time 0, at 4 hours, and at the end of the dwell.
Composition of the Combination Peritoneal Dialysis Fluid
Net Fluid and Sodium Removal at the End of Dialysis (15 Hours), and Creatinine, Urea, and Phosphate Clearances with 3.86% Glucose (G 3.86%), 7.5% Icodextrin (ICO 7.5%), and Combination Fluid (6.8% Icodextrin and 2.61% Glucose; CIG)
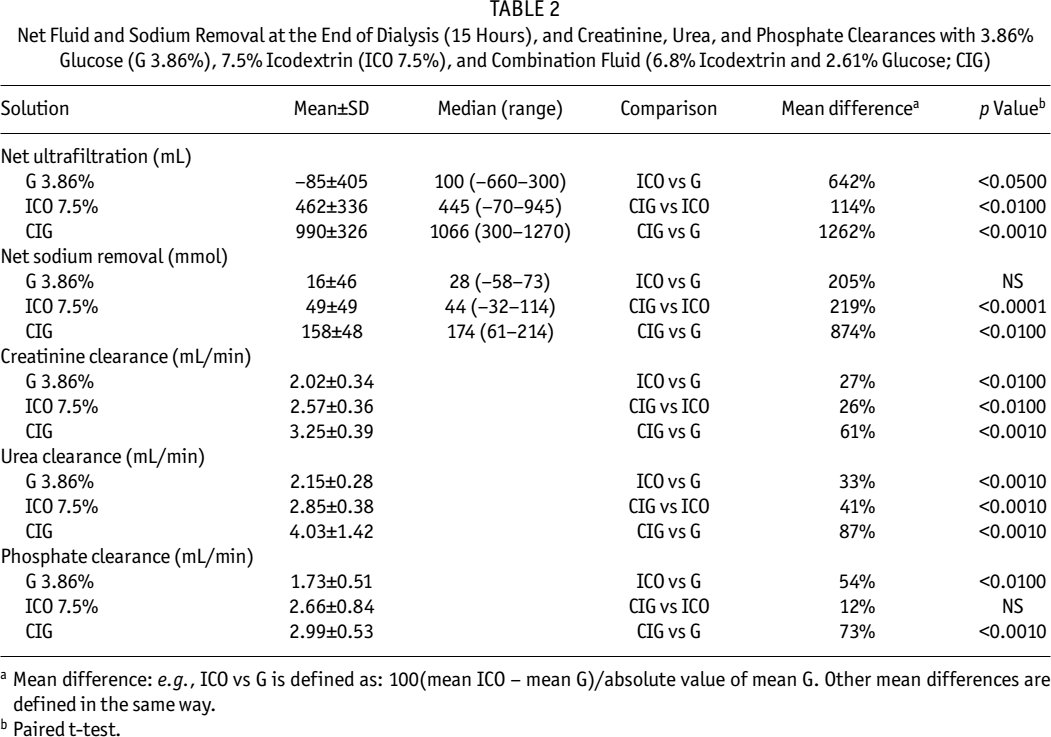
Mean difference: e.g., ICO vs G is defined as: 100(mean ICO – mean G)/absolute value of mean G. Other mean differences are defined in the same way.
Paired t-test.
Laboratory Analysis and Calculations
Dialysate volume was calculated as the difference between the weight of the drained bag (at time 0, 2, 4, 8, 12, and 15 hours) and the weight of the empty bag. Additionally, to take into account the fluid volume lost through sampling, the weight of samples taken was added to the weight of the drainage. Net drained UF volume at 15 hours was defined as the difference between the weight of the effluent (after complete drainage in sitting/supine position, with the patient rolling from side to side) plus the total volume of all dialysate samples, and the weight of the complete drainage at time 0 (just after infusion).
Glucose, urea, and phosphate in blood and dialysate were measured with an automatic analyzer (Hitachi 912; Hitachi, Meylan, France). Tests for creatinine in blood and dialysate were carried out through a specific enzymatic method. Sodium concentration was determined with a Beckman flame photometer, and osmolality on a vapor pressure osmometer.
Net drained sodium removed over the 15-hour dwell was calculated as the difference between the total amount of sodium drained at 15 hours and its measured value in the dialysate at time 0 before the initial infusion. The amount of sodium drained at any time point was calculated as the product of the drained volume times the sodium concentration in the dialysate sample obtained from the very beginning of the drainage procedure. Sodium removed at each time point was calculated using the following equation:

Mass transfers of urea, creatinine, and phosphate were calculated according to a procedure similar to that described for sodium removal (mass at time t minus mass at time 0).
Solute clearances were calculated using the following formula:

Dialysis Technique
Assessment of Peritoneal Membrane Transport Characteristics: The peritoneal solute transport profile was obtained from a standardized peritoneal equilibration test according to Twardowski; however, instead of a 2.27% glucose formulation, a 3.86% glucose-based dialysis fluid was used to document the 4-hour net UF and to characterize the role of sodium sieving during crystalloid osmosis. The glucose-based and icodextrin-based dialysis fluids were buffered with lactate.
Preparation and Composition of the Combination PD Fluid: The combination fluid was prepared by adding, in an aseptic procedure, 200 mL 30% glucose (MacoPharma; Tourcoing, France) to a 7.5% icodextrin bag with a true volume of 2100 mL, resulting in a total volume of 2300 mL. The addition of 60 g glucose from 200 mL of 30% glucose to the icodextrin solution resulted in the formulation shown in Table 1. The average values of glucose concentration (2.61%) and osmolality (412 mOsm/kg) of the fresh combination fluid were between those of 1.36% (344 mOsm/kg) and 3.86% (485 mOsm/kg) glucose dialysis fluids. For the purpose of this trial, there was no adaptation of the composition of the solution with respect to lactate, chloride, calcium, or magnesium.
Statistical Methods
Student's t-test for dependent samples was used (Statistica 5.1; StatSoft Inc., Tulsa, Oklahoma, USA). Statistical significance was accepted if p < 0.05. Data are presented as mean ± standard deviation or standard error.
Results
Fluid Kinetics
The 3.86% glucose-based solution, the 7.5% icodextrin solution, and the combination fluid (6.8% icodextrin + 2.61% glucose) were well tolerated without side effects. Net UF flow rate during the 15-hour dwell was neutral or negative with 3.86% glucose-based dialysate (-0.1 mL/min, range -0.73 to -0.33 mL/min), significantly increased with 7.5% icodextrin (0.51 mL/min, range -0.08 to 1.05 mL/min) to reach a range in keeping with previous studies, and attained twofold this volume with the combination fluid (1.1 mL/min, range 0.33 – 1.41 mL/min). Mean net UF volume drained at 15 hours increased from -85 mL (range -660 to 300 mL) with 3.86% glucose to 462 mL (range -70 to 945 mL) with 7.5% icodextrin and to 990 mL (range 300 to 1270 mL) using the combination fluid (Figure 1; Table 2). Therefore, switching from icodextrin to the combination fluid resulted in an enhancement of UF by, respectively, +184% at 8 hours, +124% at 12 hours, and +114% at 15 hours. In contrast to 3.86% glucose and 7.5% icodextrin, negative UF was not observed at any time point using the combination fluid. The difference in net UF volume between 3.86% glucose and the combination fluid was significant from 4 hours (p = 0.0016), and increased at every time point thereafter (Figure 2). The difference in net UF volume between 7.5% icodextrin and the combination fluid was significant (p < 0.01) from the beginning of the dwell at every time point.
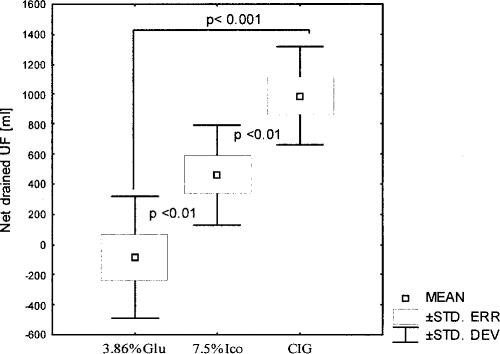
Net drained ultrafiltration (UF) volume after a 15-hour dwell in 7 patients (mean ± SD ± SE) using 3.86% glucose (3.86% Glu), 7.5% icodextrin (7.5% Ico), and a combination icodextrin (6.8%) and glucose (2.61%) solution (CIG).
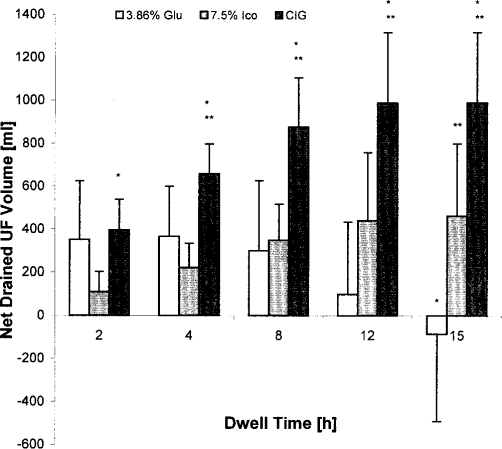
Profile of net drained ultrafiltration (UF) volume (mean ± SD) during 15-hour single-dwell exchanges using three different osmotic formulations: 3.86% glucose (3.86% Glu), 7.5% icodextrin (7.5% Ico), and a combination icodextrin (6.8%) and glucose (2.61%) solution (CIG).
Simulations of UF Volumes Using the Three-Pore Model
To elucidate whether the combination fluid exerted a specific impact on peritoneum that could explain the high net UF obtained with this solution, clinical data concerning UF volumes measured in the 7 patients were compared with data provided by simulations (prediction) performed using the three-pore model (16). The results of these simulations were presented at the 33rd Congress of the European Society for Artificial Organs, Umeå, Sweden, June 21–24, 2006.
The three-pore model, which is one of the most relevant mathematical models describing PD, is based on capillary physiology. The basic idea of this model is an assumption that transport of solutes and fluid between dialysate and blood is through three types of cylindrical pores inside the walls of peritoneal blood capillaries. Using data from clinical investigations of the 7 patients reported here, simulations were performed in three steps:
PD with 3.86% glucose: During these first simulations, previously reported specific parameters in equations describing fluid and glucose transport were adjusted to obtain the best match between simulation results and clinical data for 3.86% glucose solution.
PD with 7.5% icodextrin: During the second simulations, which concerned PD with 7.5% icodextrin, we used the values of parameters obtained during the first simulations, but, in addition, transport parameters for icodextrin fractions were adjusted in such a way that the best fit of simulation results to clinical data was obtained.
Simulations for the combination fluid were performed using all parameters obtained during the two prior simulations for 3.86% glucose and 7.5% icodextrin respectively.
The results of the simulations using previously reported values for most parameters, but with slight (not more than 30%) modification of the values of some parameters, showed that the three-pore model was able to reproduce the clinical data very well (Figure 3). These simulations confirmed that the combination fluid, compared with the two other dialysis fluids, significantly increased UF, and that this enhancement was the consequence of the UF properties of the two different osmotic agents and was not caused by a specific impact of the combination fluid on peritoneum. The detailed report of these simulations and description of the modifications of the three-pore model used to obtain this excellent fitting to clinical data will be presented in a separate paper.
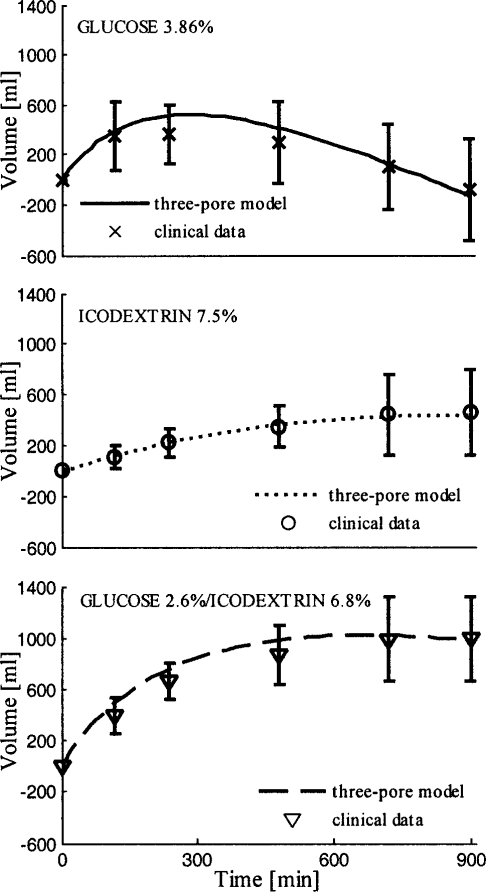
Accumulative net ultrafiltration volumes during 15-hour peritoneal dialysis with three different dialysis fluids: comparison of simulation results and clinical data (mean ± SD).
Sodium Removal
The mass of sodium removed increased when 3.86% glucose was replaced with 7.5% icodextrin [from 16 ± 46 mmol (range -58 to 73 mmol) to 49 ± 49 mmol (range -32 to 114 mmol)], but this difference did not reach statistical significance (p = 0.08). However, the mass of sodium removed with the combination fluid resulted in a much larger net sodium removal (158 ± 48 mmol), which was significantly higher than that obtained with either 3.86% glucose (p = 0.001) or 7.5% icodextrin (p < 0.0001) (Figures 4 and 5). Interestingly, the profile of dialysate sodium using the different PD fluids confirmed that maximum lowering (sieving) of dialysate sodium occurred with the glucose-based dialysis fluid after 2 hours of dwell, while a progressive and constant increase in dialysate sodium was observed during the long dwell with the combination fluid. In contrast, the use of the 7.5% icodextrin solution resulted in only marginal lowering of the dialysate sodium concentration (data not shown). No significant modification of plasma sodium (values not shown) over the long dwell time was noticed using the three solutions.
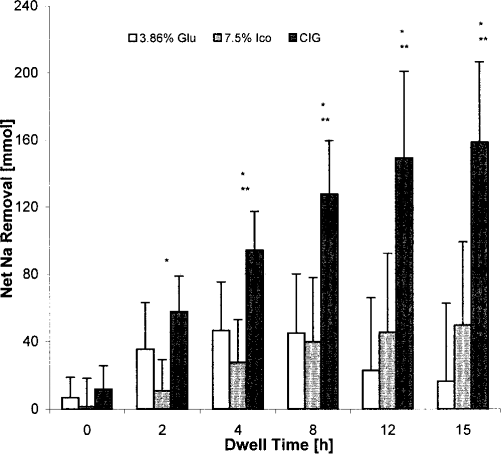
Net sodium removal (mean ± SD) during 15-hour single-dwell peritoneal dialysis (PD) exchange using three different osmotic formulations: 3.86% glucose (3.86% Glu), 7.5% icodextrin (7.5% Ico), and a combination (6.8% icodextrin & 2.61% glucose) PD solution (CIG).

Comparisons of mean net sodium removal (mmol) among three different peritoneal dialysis solutions: dialysis with 7.5% icodextrin (Ico) versus dialysis with a combination of icodextrin (6.8%) and glucose (2.61%) (CIG) (A); dialysis with 3.86% glucose (3.86%G) vs dialysis with CIG (B); dialysis with 3.86%G vs dialysis with Ico (C). ST. DEV = standard deviation; ST. ERR = standard error; MEAN = mean value. Statistical analyses by paired t-test.
Transport of other Low Molecular Weight Solutes and Proteins
Comparison of creatinine, urea, and phosphate clearances with the different solutions is shown in Table 2. Switching from 3.86% glucose-based to 7.5% icodextrin-based fluid resulted in a 27% increase in creatinine clearance. An even higher increase (61%) was observed using the combination fluid compared with the 3.86% glucose-based solution. Compared with the 7.5% icodextrin solution, the combination fluid resulted in a 26% increase in creatinine clearance.
For urea clearance, the switch from 3.86% glucose-based to 7.5% icodextrin-based solution resulted in a 33% increase in urea clearance after 15 hours, whereas replacing 7.5% icodextrin by the combination fluid increased this parameter by 41%. Comparing 3.86% glucose to the combination fluid, urea clearance increased by 87%. Based on these results, it was calculated that, in an average patient treated on a daily basis with a common APD schedule (24-hour cycle includes a 9-hour nocturnal session and a 15-hour-long day dwell), the combination fluid increased weekly urea and creatinine clearances by 7.8 L and 11.8 L, respectively, compared with the values of weekly clearances yielded by the 3.86% glucose-based dialysis fluids.
The increase in phosphate transport was 54% on changing from the 3.86% glucose-based solution to 7.5% icodextrin, 12% on switching from 7.5% icodextrin to the combination fluid, and 73% on moving from 3.86% glucose to the combination fluid. Mean loss of total protein during the dwell was 6.17 g with the 3.86% glucose-based solution, 4.02 g with 7.5% icodextrin, and 4.23 g using the combination fluid. Total protein clearance was 104, 75, and 73 μL/min with 3.86% glucose, 7.5% icodextrin, and the combination fluid, respectively.
Osmolality
As shown in Figure 6, one of the most important features of the combination fluid is that high peritoneal net UF can be maintained at a relatively low dialysate osmolality during a long dwell. The osmolality of the combination PD solution decreased throughout the dwell, and after 4 hours it was not significantly higher than the osmolality of the icodextrin solution at the same time.
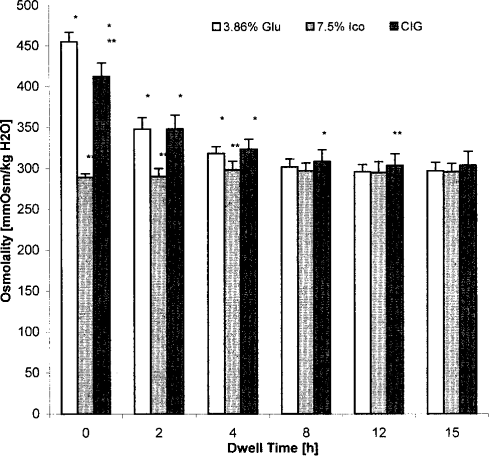
Osmolality (mean ± SD) during 15-hour single-dwell peritoneal dialysis (PD) exchange using three different osmotic formulations: 3.86% glucose (3.86% Glu), 7.5% icodextrin (7.5% Ico), and a combination (6.8% icodextrin & 2.61% glucose) PD solution (CIG).
Discussion
As demonstrated in this study, a major advantage of the combination fluid over the glucose-based and icodextrin-based dialysis solutions is that it enhances net UF and sodium removal during a 15-hour-long PD dwell exchange. This is in general agreement with results from previous studies using a combination fluid (13-15), where a similar advantage was seen for much shorter dwell times. The profile of net UF and sodium removal using 3.86% glucose-based and 7.5% icodextrin-based solutions was in keeping with expectations based on previous dwell studies (9,17) showing that, after 8 hours of dwell, net UF volume and net sodium removal with 3.86% glucose-based solution and 7.5% icodextrin-based solution were equivalent.
The unsatisfactory result of the 3.86% solution with respect to fluid and solute removal during a 15-hour dwell was an expected finding in our patients who displayed a rapid peritoneal small solute transport rate. When using a 3.86% glucose solution, the osmotic gradient declines rapidly due to glucose diffusion across the numerous small pores in the endothelium of the peritoneal capillaries (18). In contrast, the 7.5% icodextrin-based solution induces colloid osmosis, which causes slow but sustained fluid and sodium transport across the membrane. Nevertheless, the slow but continuous backflow of fluid due to reabsorption of dialysate during a long PD dwell exchange imposes a limitation on the 24-hour net water and sodium extraction also in patients treated with 7.5% icodextrin solution (19). The combination fluid not only provided a very efficient means to promote UF but, moreover, simultaneously enhanced sodium removal. In the current study, the low sodium concentration (121 mmol/L) in the combination fluid is likely to have further contributed to an additional increase in the diffusion of sodium, but without generating hyponatremia as generally observed in studies on glucose-based low sodium dialysate for APD and continuous ambulatory PD (CAPD) (20-23).
The use of the combination PD fluid during the 15-hour dwell yielded as much as 80% – 100% of the desirable daily UF volume and of the sodium removal required in an average anuric patient. The present results show that this strategy may be much more effective than any other therapeutic option investigated and/or clinically adopted during the past 25 years of PD practice.
A fast peritoneal transport rate is associated with the risk of UF capacity loss, making PD treatment less attractive in high transport patients, who represent a considerable portion of PD patients (24). The prescription of more hypertonic exchanges in CAPD may generate major damage to the peritoneal membrane, which in turn may lead to a high rate of withdrawal from PD programs. For a long time, this has been one of the reasons for preferring short-dwell APD over CAPD in high transporters, and it has also resulted in increased attention to the nocturnal APD schedule in an attempt to optimize fluid and sodium removal, which is linked with the ratio of fill volume to number of cycles in average-sized high transporters (25).
Switching to “intermittent mode” (with dry day) in order to prevent the net fluid loss from the cavity that characterizes very long dwells is not recommended in anuric patients since the absence of dialysate significantly reduces small solute clearance and, in addition, reduces the clearance of middle sized molecules. A study in 9 APD patients with high transport profiles using a low sodium formulation (126 mmol/L) highlighted the efficacy of increasing the diffusive gradient of sodium to enhance sodium removal, but failed in achieving a parallel increase in water transport, eventually resulting in significant hyponatremia (20). Note that, in our short-term study, plasma sodium did not change significantly in patients receiving the combination fluid.
The widespread use of 7.5% icodextrin during the long dwell provides a significant advance in volume management of PD patients (3,10,26-31), especially in comparison with 1.36% and 2.27% glucose-based dialysis fluids. In a recent study carried out in 46 patients with a high transport profile, Finkelstein et al. (9) found that 7.5% icodextrin was significantly more effective during 14- to 16-hour dwells than 3.86% glucose with respect to fluid and sodium removal, and that the greatest improvement was seen in high transporters. Yet, in spite of this progress, PD patients with minimal urine production or complete anuria have an increased risk of complications related to cardiovascular disease and uncontrolled hypertension.
In the current study, the net UF gained by switching from 3.86% glucose solution to 7.5% icodextrin solution was 420 mL, and the icodextrin-based solution removed 41 mmol of sodium more than the glucose-based solution. Considering the deleterious effect of prolonged exposure to high glucose tonicity on peritoneal membrane structure and function — even when using more biocompatible glucose-based solutions — as well as the metabolic consequences of an increased glucose load, there is presently no reason to support the prescription of hypertonic glucose solutions for the long dwell, except if there is a history of intolerance to icodextrin (32). However, without neglecting the evidence-based advantages of icodextrin over hypertonic glucose, there are many reasons to explore novel PD solutions in attempting to surpass the effects gained by using the glucose polymer (29).
As early as the year 1997, with the aim of reducing glucose exposure, ML Laboratories (Manchester, United Kingdom) set up a project investigating the use of mixed solutions of icodextrin plus glucose for continuous use in CAPD. Peers (13) reported data for single dwells of 7.5% icodextrin plus 0.35% glucose, 2% icodextrin plus 0.68% glucose, and 2.5% icodextrin plus 0.68% glucose. Recently, Jenkins et al. (14,15) conducted an elegant study using a combination of 1.36% glucose and 7.5% icodextrin, and also presented results of computer modeling based on the three-pore theory by Rippe (16). However, unlike the present study, the dwell time was limited to 7 hours and 8 of 11 patients in the study population had peritoneal transport characteristics ranging from low-average to low transport rate. The extension of this trial in the form of a 4-week crossover study (15) established that the use of the combination solution resulted in a 33% increase in long-dwell net UF and a 29% increase in 24-hour net UF. Fluid absorption from the peritoneal cavity to the adjacent tissue capillaries (19) is of major importance, as underlined by Abu-Alfa et al. (33), and the finding that the combination fluid seems to balance fluid absorption during the latter part of the dwell (see Figure 3) may explain, at least in part, the dramatic increase in fluid and sodium removal when using this solution compared to the use of its two osmotic components individually.
In light of the results of the simulations presented above (see Results) showing that the combination fluid does not seem to have any specific impact on peritoneum, the likely explanation of the excellent performance of the combination fluid with respect to the high net UF volume at 15 hours is therefore as follows: The glucose component in the combination fluid resulted in an expected rapid initial rise in peritoneal volume. During the latter part of the dwell, the icodextrin component compensated for glucose dissipation as well as for fluid absorption. Therefore, the peritoneal dialysate volume rose during the first half of the dwell and then changed only a little during the second half (Figure 3). The results of these simulations have been published in abstract form (34) and will be described in greater detail in a forthcoming paper.
In conclusion, during a single-dwell exchange of 15 hours, a combination fluid with 6.8% icodextrin, 2.61% glucose, and sodium 121 mmol/L yielded twofold greater net UF and threefold greater sodium removal compared to a 7.5% icodextrin-based solution. This novel strategy seems able to effectively alleviate the difficulties in reaching fluid and sodium balance in anuric CAPD/ APD patients with a rapid peritoneal solute transport rate. As much of the daily need for fluid and sodium removal can be reached during a long dwell with the combination fluid, this strategy also provides the advantage of reducing exposure of the peritoneal membrane to high-tonicity glucose-based dialysate during the remainder of a 24-hour CAPD/APD treatment cycle. This could lead to better preservation of the peritoneal membrane and fewer metabolic alterations. The clinical effects of this new treatment mode on hypertension, left ventricular hypertrophy, and other consequences of fluid overload, as well as potential risks of too excessive removal of fluid and sodium, which, in some patients, could result in hyponatremia, need to be evaluated in long-term clinical trials. Furthermore, there is a need to study the effects of the combination fluid on total glucose exposure over 24 hours, as well as how much glucose is absorbed with this regimen compared to conventional regimens. Finally, it cannot be ruled out that, because of the dramatic increase in fluid and sodium removal, the combination fluid could have a negative effect on residual renal function if used too early in the course of a patient's dialysis history.
Footnotes
Acknowledgment
Jose C. Divino Filho and Bengt Lindholm are employed by Baxter Healthcare.