
Abstract
Objective
Elevated C-reactive protein (CRP) level is an independent predictor of all-cause and cardiovascular mortality in peritoneal dialysis (PD) patients. Statins have been demonstrated to have anti-inflammatory properties by virtue of their CRP lowering effects in hemodialysis patients. However, whether statins have an anti-inflammatory effect in PD patients is unknown.
Design
All prevalent PD patients at our center were reviewed. Eligible (257) patients were categorized into 2 groups: those on statin therapy (n = 137) and those not on statins (n = 120). Data were abstracted for hemoglobin, albumin, phosphates, cholesterol, CRP, Kt/V, and erythropoietin dose, along with relevant clinical data.
Results
The two groups had similar concentrations of hemoglobin, albumin, and phosphates. They were also matched for dialysis adequacy and duration of dialysis but the statin group patients were older (57 ± 13 vs 52 ± 17 years, p = 0.01). Serum cholesterol was lower in the statin group (4.74 ± 1.05 vs 5.02 ± 1.17 mmol/L, p < 0.05). Single-point (14 ± 13 vs 19 ± 18 mg/L, p < 0.02) and serially measured CRP (9 ± 7.4 vs 12 ± 10 mg/L, p < 0.02) levels were significantly lower in the statin group despite increased comorbidity (0.84 vs 0.54, p < 0.02) and greater incidence of diabetes mellitus (52% vs 25%, p < 0.01).
Conclusion
Statin therapy is associated with low single-point and serially measured CRP levels in PD patients, thereby suggesting that their anti-inflammatory properties persist in PD. These data have implications for considering statin therapy in PD patients as an anti-inflammatory agent in addition to a cholesterol lowering drug.
Keywords
A single elevated level of C-reactive protein (CRP), a marker of inflammation, is an independent predictor of all-cause and cardiovascular mortality in end-stage renal failure patients on continuous ambulatory peritoneal dialysis (CAPD) (2).
3-Hydroxy-3-methylglutaryl coenzyme A reductase inhibitors (statins), potent cholesterol lowering agents, have been shown to have pleiotropic effects, including anti-inflammatory effects. The anti-inflammatory effects of statins, as assessed by serum CRP levels, have not been evaluated in peritoneal dialysis (PD) patients. In this study, we aim to ascertain the effects of statin therapy on serially measured and single-point serum CRP levels in PD patients.
Methods
The study was performed in accordance with the Ethics Committee guidelines set out by the East London and The City Health Authority. A review of all 257 prevalent patients on PD on 1 May 2003 at our center was performed. Clinical data, including comorbidity data submitted to the Renal Registry, United Kingdom, were collected from our quarterly updated detailed computerized records and review of patient medical and nursing notes.
Comorbid conditions collected included history of angina, myocardial infarction within the previous 3 months, myocardial infarction more than 3 months ago, cerebrovascular disease, diabetes (not causing established renal failure), chronic obstructive pulmonary disease, malignancy (excluding basal cell carcinoma), current claudication, smoking (current or history of smoking within the previous year), and angioplasty/ stenting/vascular grafts (all non-coronary). Presence of each disease was assigned a score of 1 and Davies comorbidity score was calculated from the data (Table 1).
Baseline Demographics Characteristics
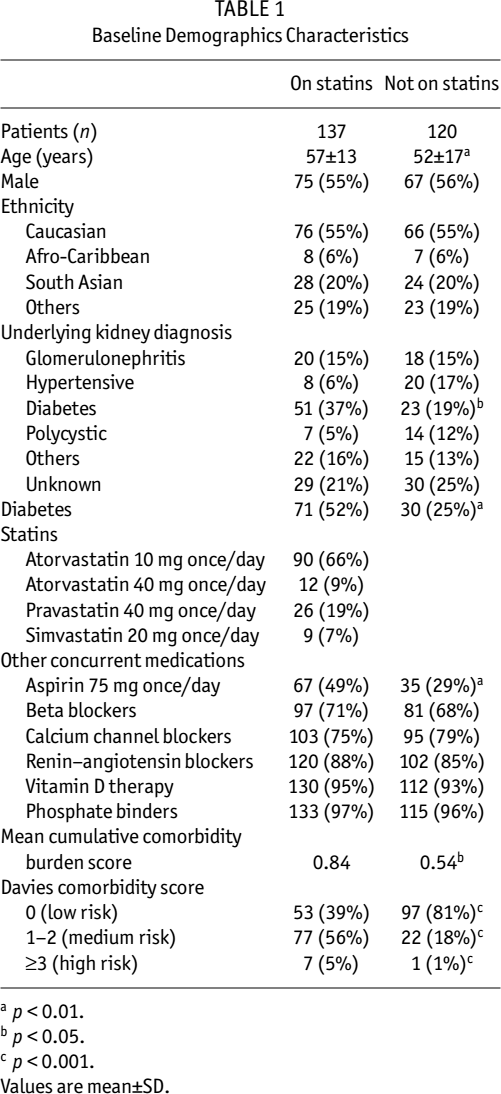
p < 0.01.
p < 0.05.
p < 0.001.
Values are mean±SD.
The patients were categorized into two groups: statin group and non-statin group. The statin group comprised 137 patients who were taking statins (atorvastatin, simvastatin, and pravastatin) and the non-statin group comprised 120 patients who were not on statins. Historical laboratory values were collated from the Pathology database but samples were excluded if the patients had ongoing acute infection, including peritonitis and severe exit-site infections. Patients with severe acute intercurrent illnesses were also excluded. Data collected included the latest serum CRP value (single-point CRP) and the latest three serial CRP values taken at least 30 days apart but within the previous 6 months. Serum CRP concentrations were analyzed by the immunoturbidimetric method (Olympus Diagnostics, Hamburg, Germany). An elevated CRP was defined as greater than or equal to 5 mg/L, which is the upper limit in the general population. Albumin concentration was determined by the bromcresol green method (Olympus AU640 chemistry immuno analyzer). Cholesterol and phosphates were determined by cholesterol esterase method and phosphomolybdate method respectively (Olympus AU640).
Dialysis dose (Kt/V) was calculated from 24-hour dialysate collection using computer software (PD Adequest, Baxter Healthcare, Deerfield, Illinois, USA). Peritoneal membrane transport was calculated from peritoneal equilibrium tests and residual renal function was measured from standardized 24-hour urine collection (calculated as mean of urea and creatinine clearances and expressed normalized to 1.73 m2 body surface area).
The significance of differences in clinical and laboratory data between the two groups was tested by unpaired t-test, Mann–Whitney U test, Wilcoxon signed-rank test, and chi-square test as appropriate. A p value less than 0.05 was considered statistically significant.
Results
Baseline demographic characteristics of the original study cohorts are shown in Table 1. Patients on statins were significantly older (57 ± 13 vs 52 ± 17 years, p = 0.01) and had significantly higher incidence of diabetes (52% vs 25%, p < 0.01) compared to the non-statin group. Average comorbidity burden score was significantly greater for the statin group compared to the non-statin group (0.84 vs 0.54, p < 0.02).
On comorbidity scoring according to the Davies scoring system, a significantly higher proportion of patients in the statin group were in the medium to high risk category compared to the non-statin group. The latter group had a significantly higher proportion of patients in the low risk group (Table 1.)
Biochemical and dialysis parameters are shown in Table 2. Serum cholesterol was significantly lower in the statin group (184 ± 41 vs 195 ± 45 mg/dL, p < 0.05; 4.74 ± 1.05 vs 5.02 ± 1.17 mmol/L, p < 0.05).
Baseline Relevant Biochemical and Dialysis Indices
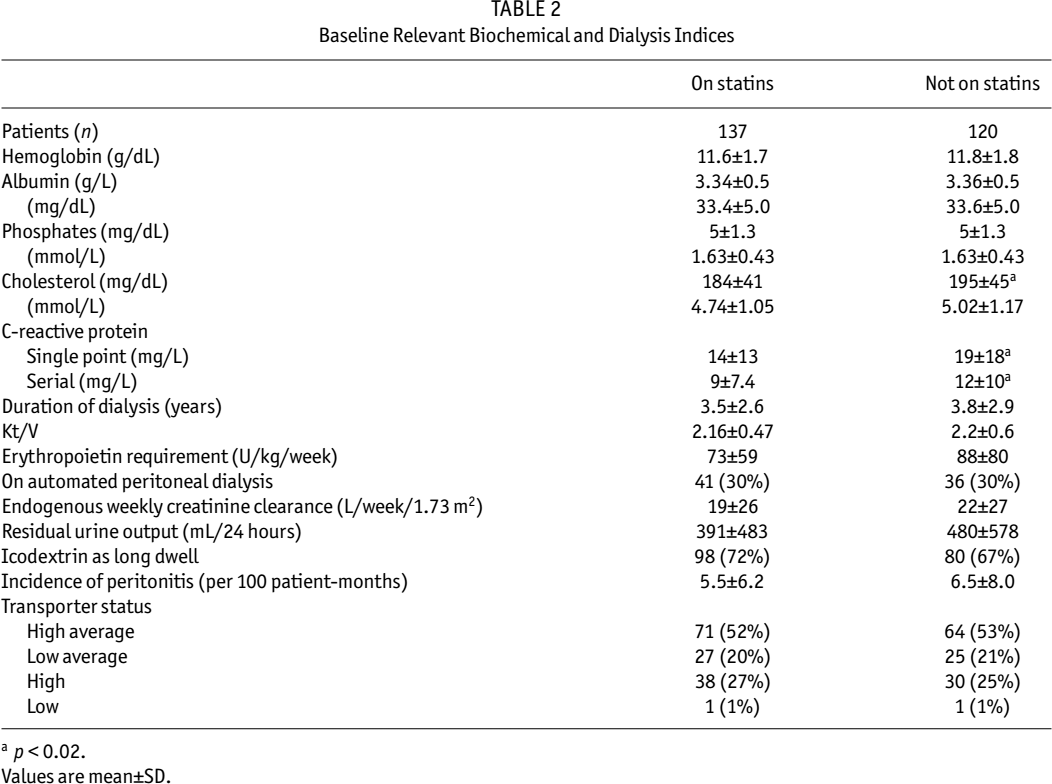
p < 0.02.
Values are mean±SD.
Single-point CRP (the most recent value) was 14 ± 13 mg/L in the statin group versus 19 ± 18 mg/L in the non-statin group (p < 0.02). The mean of the serial CRP levels was also significantly lower in the statin group: 9 ± 7.4 vs 12 ± 10 mg/L, p < 0.02 (Table 2).
Subgroup Analysis
A subgroup consisting of 46 patients was identified in the statin group where a definitive date of commencement of statin therapy was available and in whom we had biochemistry available prior to commencement of statin therapy. In this subgroup, mean duration of treatment with a statin was 18 months. We compared this subgroup with patients from the non-statin group who also had at least 18 months of historical biochemical values (n = 96). After the start of statin therapy, CRP fell significantly, from 14.5 ± 8.2 to 10.4 ± 4.5 mg/L at the last follow-up (p < 0.01), while cholesterol levels fell from 193 ± 66 to 170 ± 43 mg/dL (p < 0.05) (5.0 ± 1.7 vs 4.4 ± 1.1 mmol/L) (Table 3). In the control cohort (non-statin group), there were no statistically significant changes in cholesterol (193 ± 1 vs 191 ± 1 mg/dL) or CRP (8.8 ± 8.1 vs 10.7 ± 9.3 mg/L) over the 18-month study period. However, both groups experienced a similar reduction in serum albumin: from 3.67 ± 5.3 to 3.21 ± 4.4 vs from 3.94 ± 5.0 to 3.46 ± 4.8 g/dL in the statin and non-statin groups respectively.
Subgroup Analysis of Patients with 18 Months of Treatment with Statin (Statin Group): Changes in Relevant Biochemical and Dialysis Indices in the Statin and Non-Statin Groups over a Mean Duration of 18 Months. Control Group Comprised of Patients Who Were Never Prescribed Statins (Non-Statin Group)
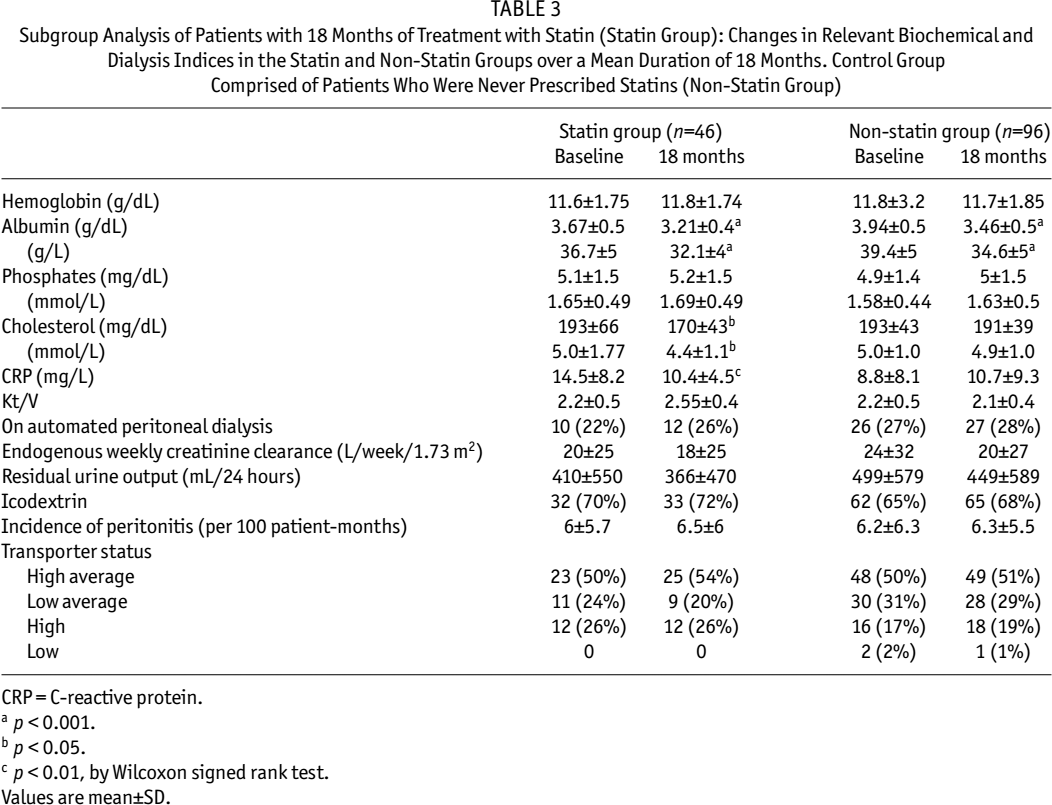
CRP = C-reactive protein.
p < 0.001.
p < 0.05.
p < 0.01, by Wilcoxon signed rank test.
Values are mean±SD.
Discussion
To the best of our knowledge, we have conducted the first study to evaluate the effects of statins on CRP in PD patients. Our results showed that, despite demographic differences (increased incidence of diabetes mellitus and higher comorbidity burden) that might lead to bias toward higher CRP, the patients treated with statins had lower serum CRP concentrations (both single and serial). Moreover, initiation of statin correlated with a significant reduction in CRP, although causality has not been strictly proven.
The limitations of our study must be acknowledged. This was a retrospective analysis of results available from routine clinical investigations. “Ultrasensitive” assays for CRP were not available to us during the study period. Nevertheless, we believe our data remain valid as a similar CRP assay was used and was found to be an independent marker of atherosclerotic disease in this group of patients. Moreover, the fact that a significant statistical difference was detected using a “non-ultrasensitive” CRP assay strengthens the assertion that the difference is likely to be of clinical relevance. Because of the retrospective nature of the study, data for other markers of inflammation (such as interleukin-6 or tumor necrosis factor-alpha) were not available. However, we believe that the “time averaged” CRP (i.e., average of 3 serial readings over a 6-month period) is a good index of chronic inflammation in our patients.
Allocation of patients to the study groups was determined by the clinical use of statins, the indications being first-line treatment for dyslipidemia and for secondary prevention of cardiovascular disease along the guidelines set by the International Society for Peritoneal Dialysis (ISPD) (3). This has obviously skewed the demographics of the two groups and explains the high prevalence of diabetes mellitus and the higher burden of comorbidity in the treated group. Studies have shown that diabetics on PD have higher CRP levels than nondiabetics (4) and, intuitively, higher comorbidity might also be expected to correlate with higher CRP. The comorbidity score we used was derived from the quarterly submission to the UK Renal Registry. This is more comprehensive and comprises all factors that make up the other validated co-morbidity indices of Khan, Davies, and Charleston. Thus, the fact that CRP (measured either as a single time point or as a time-averaged mean) is lower in the statin group is particularly significant.
We considered other factors that might have accounted for such a difference. Residual renal function (5), use of biocompatible PD solutions (6,7), and malnutrition (4) are all known to influence CRP. However, in our study there were no differences in residual renal function as defined by 24-hour urine collections (both creatinine clearance and urine volume). During the study period, the only “biocompatible” PD solution widely used in our unit was icodextrin, but there were no statistical differences in its use in the two groups. Although imperfect, the biomarker of nutrition that we used was albumin, and it was not statistically different in the two groups. This might appear somewhat surprising as, overall, there was a statistically significant inverse correlation between albumin and CRP (Spearman r = -0.25, p < 0.0001). It is possible though, that differences in nutritional status might account for the lower CRP in the statin group; however, this group exhibited a greater comorbidity than would normally be associated with more malnourished patients and lower serum albumin.
A significantly greater proportion of patients were on aspirin therapy in the statin group. This is not surprising because of the aforementioned baseline differences in the two groups with respect to diabetes mellitus and comorbidity score. So far, the only published study involving patients on CAPD, a randomized trial (8), revealed that aspirin (200 mg once/day) therapy for 8 weeks did not affect high-sensitivity CRP levels in 86 CAPD patients. In a prospective, randomized, placebo controlled, double-blind study (9), low dose aspirin (81 mg every day or 325 mg every other day) failed to lower highly-sensitivity CRP levels in 32 healthy volunteers in spite of the profound anti-platelet effect of low doses of aspirin, as demonstrated by a marked dose-related decline in platelet-derived serum thromboxane B2. Hence, it is extremely unlikely that, in our study, low dose aspirin (75 mg once/ day) is responsible for low CRP levels (measured by “non-ultrasensitive” assay) in the statin group.
In an attempt to address whether statins lower CRP levels, we performed a cohort analysis of patients starting statins therapy compared with those never prescribed statins. We identified patients in the study that had 18 months of data (after initiating statin therapy) and compared them with patients who never had statins but with similar follow-up (18 months). We demonstrated that, after starting statins, both CRP and total cholesterol fell significantly (by 31% and 28% in 18 months). However, control patients (patients who were never prescribed statins) experienced a 22% increase in serum CRP levels during a similar duration. It should be acknowledged that our study was not adequately powered to detect intergroup differences in CRP and our conclusion is at risk of type II statistical error.
Both groups demonstrated similar reduction in serum albumin (12.8% vs 12.1% in statin vs non-statin). The statin-treated patients demonstrated a decrement in CRP despite falling albumin. This suggests that statins are having direct anti-inflammatory effects and that the fall in CRP is not related to changes in nutrition induced by the statin. Nevertheless, there remains the possibility that unidentified confounding factors may have caused the lower CRP in the statin patients. It is also of interest that the statin patients had a higher baseline CRP level, although this did not reach statistical significance. As discussed above, this would be more in keeping with expectations for patients with lower serum albumin and greater comorbidity.
Our results are generally in agreement with the results of studies in hemodialysis patients: significant reduction in CRP levels after simvastatin (10) and atorvastatin (11) have been demonstrated.
In summary, despite the limitations of retrospective and cohort studies, our studies showed statins to be associated with a lower level of CRP, a marker of inflammation. Although causality cannot be proven, we believe our study provides circumstantial evidence that statins have an anti-inflammatory action in PD patients. Nevertheless, randomized controlled trials are required.