
Abstract
Pregnancy in end-stage renal disease patients is infrequent and is associated with fetal loss, premature delivery, intrauterine growth restriction, and lack of control of or exacerbation of or onset of hypertension. Even after replacement of renal function, the prognosis for the patient and the fetus is poor. A point of controversy is the renal replacement therapy method. This report is based on two clinical cases of pregnancy in peritoneal dialysis patients that resulted in full-term delivery. Adequate metabolic and blood pressure control was achieved during pregnancy, the only mutual complication being the presence of polyhydramnios. However, both infants were healthy for their gestational age and without neonatal complications. We may conclude that peritoneal dialysis is an acceptable therapeutic option for pregnant patients and their fetuses.
Keywords
Other points to solve in this type of patient are the possible complications of pregnancy, such as onset or exacerbation of systemic arterial hypertension, which may evolve into preeclampsia or even eclampsia, premature delivery, or failure of the product to grow.
We report here the cases of 2 pregnant patients treated in our hospital who were diagnosed with ESRD and whose renal function was replaced with PD.
Clinical Cases
Case 1
A 28-year-old female patient who had been pregnant for 12 weeks, as dated by the last menstruation, and who had an important history of bilateral nephrolithiasis since the age of 7, diagnosed in the Central Military Hospital (Hospital Central Militar), but who abandoned treatment for 20 years, was admitted.
In 1996 she became pregnant, with outpatient control to term. The pregnancy was complicated with placenta previa was terminated by caesarean section; a female product weighing 2300 g was obtained. An intrauterine device after termination of the pregnancy provided contraception until 2 years prior to her next pregnancy. The patient came to the outpatient Nephrology Clinic under referral by the Female Specialties Clinic due to pregnancy of 16 weeks with renal disease.
Notable during her examination upon admission were blood pressure 110/70 mmHg, heart rate 80/minute, temperature 36.5°C, weight 45 kg, height 162 cm, body surface area 1.41 m2; facies of nephropathy, Subjective Global Assessment class C, pallor, and globose abdomen at the expense of the uterus, with pubis fundus diameter 15 cm, with no edema. Laboratory studies on admission are shown on Table 1. Urine culture was positive for Escherichia coli, 24-hour creatinine clearance was 5 mL/minute, urine volume was 2 L. On renal ultrasound, right kidney was 79 x 30 mm, showed loss of corticomedullary differentiation and presence of multiple calculi in the pelvis; left kidney was 94 x 54 mm, with hydronephrosis of 78 x 48 mm and a single stone in the interior. Obstetric ultrasound showed a single live product compatible with 16 weeks by measurement of biparietal diameter and cephalic circumference, normal placenta inserted with maturity degree 0, and normal amniotic fluid. The patient was hospitalized with the following diagnoses: pregnancy compatible with 16 weeks of gestation by ultrasound, ESRD secondary to obstructive nephropathy due to renal lithiasis, urinary tract infection, and normocytic normochromic anemia.
Summary of Laboratory Values on Admission and 24 Hours Prior to Delivery in Two Patients
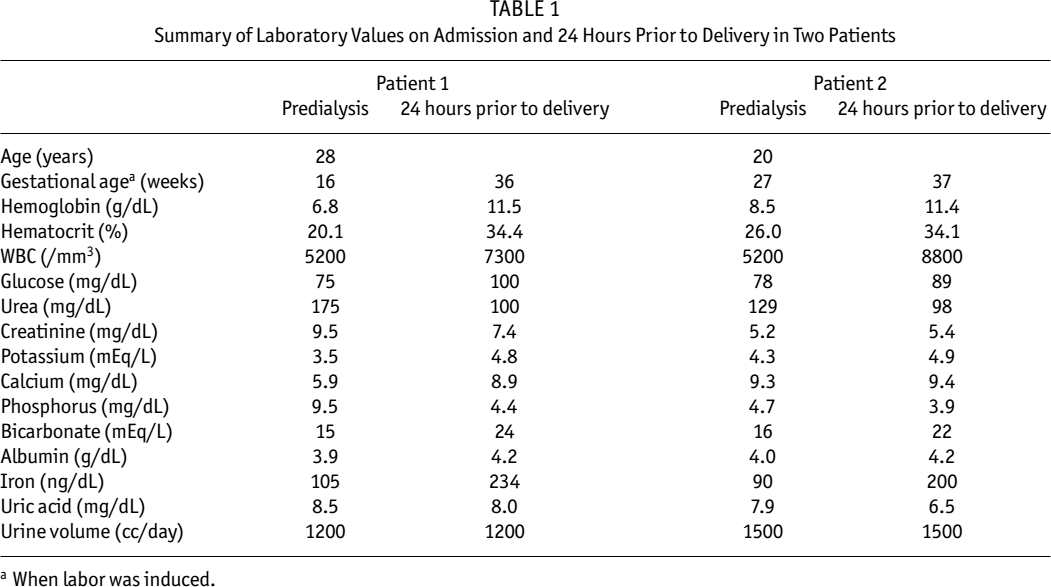
When labor was induced.
Due to the foregoing, a multidisciplinary approach was taken by the Urology, Obstetrics, and Nephrology Services as follows: Urology Service placed a double-J catheter in the left kidney; Obstetrics Service, considering the mother's decision to continue the pregnancy despite the risks, ordered control of the pregnancy by continuous inpatient monitoring; Nephrology Service ordered dietary management, blood transfusion with two units of packed cells, ampicillin, vitamin supplements, calcium, oral iron, calcitriol, and erythropoietin. It was decided to begin PD. The Tenckhoff catheter was placed on 13 June by the transplant surgeon using the laparoscopic technique. Peritoneal dialysis was started immediately with 6 exchanges of 1.5% glucose PD solution in 24 hours. Since the patient mentioned dizziness and abdominal pain due to the dialysis volume, the infused volume was gradually increased, beginning with 750 mL. By the end of 1 week, the patient was tolerating 1.5 L; dwell time in the abdominal cavity was also progressive. The patient was discharged from the Central Military Hospital on 29 June, being hospitalized in the Female Specialties Clinic to continue supervision of the pregnancy as well as her dialysis treatment.
The patient was monitored weekly during the pregnancy by obstetric ultrasound, which documented polyhydramnios. The following nephrologic care was given:
Diet calculated for proteins 1.5 g/kg body weight, phosphorus 800 mg/day, 45 calories per kg body weight, and total liquids 1500 cc/day.
PD dose was set to six exchanges per day, five with 1500 mL 1.5% PD solution with a dwell time of 3 hours, and one 1500 mL exchange of 4.25% PD solution with a dwell time of 4 hours, a weekly Kt/V being obtained of 1.9 and a weekly creatinine clearance of 58 L. Mean urea and creatinine levels during pregnancy were 100 mg/dL and 7 mg/dL respectively. She also had residual urinary volume of 1.2 L daily.
Treatment for anemia was based on erythropoietin 3 times per week plus parenteral administration of iron once per week, which resulted in a hemoglobin value of 11.5 g/dL at the end of the pregnancy.
The main complications during the pregnancy were a gastrointestinal feeling of fullness during dialysis and urinary tract infections on four occasions, documented by positive urine culture for E. coli in the four cases. She never had signs of peritonitis or infection of the tunnel, or catheter dysfunction. Polyhydramnios was documented by obstetrical ultrasounds. She was normotensive without medication.
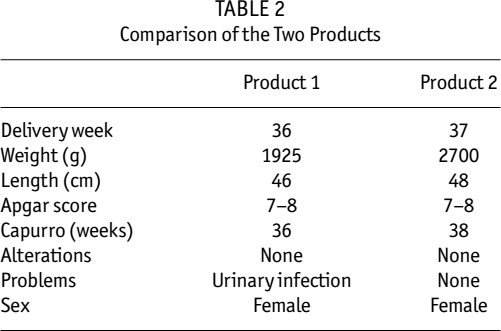
Laboratory studies were performed 24 hours prior to delivery and are summarized in Table 1. Delivery was induced in the 36th week of pregnancy. A female was born weighing 1925 g, length 46 cm, Apgar score 7 – 8, Capurro 36 weeks (Table 2); she had neonatal sepsis treated with cefepime and was later discharged without complication. At the time of birth, the infant's creatinine was 7.8 mg/dL and it took 10 days to normalize at 0.2 mg/dL. The mother was transplanted 1 year after delivery and currently has normal kidney function.
Comparison of the Two Products
Case 2
A 20-year-old primigravid patient with pregnancy of 27 weeks was admitted. She came for pregnancy control for the first time 17 July 2005 and was found to be azotemic. She was consequently hospitalized for study and treatment. During the admission examination, she had blood pressure 120/80 mmHg, heart rate 79/minute, temperature 36°C, weight 74 kg, height 155 cm; globose-form abdomen at the expense of a 2 cm subcutaneous fat layer, gravid uterus with pubis fundus diameter of 26 cm, and no edema of the limbs. The admission laboratory studies are summarized in Table 1. Creatinine clearance was 13 mL/minute/24 hours, with urine volume of 1500 mL. Ultrasound showed right kidney 80 x 50 mm with loss of cortex, left kidney 78 x 30 mm with loss of cortex, and no dilation of either collector system. Obstetrical ultrasound showed a single live product compatible with 27 weeks by measurement of biparietal diameter and cephalic circumference, normal placenta insert with degree of maturity 1, and normal amniotic fluid. Because of the foregoing, we considered the following: primigravida with pregnancy of 27 weeks and complicated gestation and ESRD of unknown etiology. The therapeutic approach began with control by the Pregnancy Clinic associated with strict weekly monitoring by the Obstetrics Service. The Nephrology Service established the following:
Diet calculated for calories 30 kcal/kg/day, proteins 1.3 g/kg/day, lipids under 30% polyunsaturated, sodium chloride 3 g, potassium 2 g, phosphorus 800 mg, free liquids.
Strict blood pressure monitoring.
Vitamin supplementation.
For treatment of the anemia, intravenous iron dextran and erythropoietin 3 times per week.
Mineral metabolism: calcium carbonate 1 g with each meal, and calcitriol 0.25 μg/day.
Surgical placement of a Tenckhoff catheter by the Transplant Surgery Service.
Evolution of the pregnancy was as follows: Following Tenckhoff catheter placement, PD was begun with six exchanges of 750 mL 1.5% PD solution. The PD solution infusion volume was increased by 250 mL each week until 1.5 L was reached. On 1 August 2005, there was a dialysate leak through the surgical wound and PD was therefore discontinued for 5 days, restarting on 6 August with the same solution and with a volume of 1000 mL for 1 week; the following week, 1.5 L was reached. The total dose of PD was six exchanges of 1.5 L: five exchanges with bags of 1.5% and one with one bag of 2.5%.
Obstetrical ultrasound was performed each week in order to monitor the evolution of the product; polyhydramnios was documented beginning in the third week after continuous ambulatory peritoneal dialysis (CAPD) began. The PD dose was maintained with ultrafiltration of 1000 mL/day and urine volumes of 1700 mL/day, as well as serum urea below 70 mg/dL and creatinine 5.9 mg/dL as an average until 24 hours prior to delivery. Correction of hemoglobin was achieved a month after the start of erythropoietin. At the end of the pregnancy, hemoglobin was 11.4 g/dL and hematocrit 34.1%. Mineral metabolism was maintained with serum calcium 9.4 mg/dL, phosphorus 3.9 mg/dL, and parathyroid hormone 99 pg/dL. As for PD, no signs of peritonitis appeared.
Laboratory studies were performed 24 hours prior to delivery (Table 1). Peritoneal dialysis was suspended at the end of week 38 of the pregnancy and labor was induced with two intravaginal doses of misoprostol. Normal vaginal delivery occurred after 18 hours. A female was born weighing 2700 g, length 48 cm, Apgar score 7 – 8 at 1 minute and at 5 minutes, and Capurro 38 weeks (Table 2). The patient started PD again 48 hours post delivery. She was discharged 72 hours after delivery without complications. The infant did not present complications and was discharged at the same time as the mother. The mother was given a transplant from a related living donor 6 months postpartum and is currently without complications.
Discussion
Possibilities of Pregnancy
Pregnancy in patients with ESRD is infrequent. The understanding of the physiopathology of infertility in this type of patient is that this infrequency is due classically to anovulation and hyperprolactinemia being responsible for the oligomenorrhea seen in female patients on dialysis (5). Another factor mentioned is the reduced libido of these patients, which, according to some authors, is caused by alterations in human chorionic gonadotropin pulses due to increased endorphins, which in turn are due to reduction of renal clearance (6). Notwithstanding, there are other studies in which the reduction in renal leptin clearance seems to have a relationship with its consequent serum elevation, which alters the hypothalamus–pituitary axis through the “Y” neuropeptide, and its high affinity for some sites in the hypothalamus (7).
Conception Rate and its Outcome in Dialysis Patients
Another point to define is the full-term pregnancy in patients using some dialytic procedure. The international medical community has scarce data on this subject because registries are limited. However, there are some references: According to the United States Renal Data Systems, in 1992, of 12 992 women under 44 years of age who were receiving dialysis, there were 344 pregnancies (2.6%); of these, 209 women were already receiving dialysis, 58 women became pregnant before beginning dialysis, and for 77 of the women, onset of dialysis was unknown. Of these total pregnancies, 42% were full term, 32% had spontaneous miscarriage, 10.5% were aborted therapeutically, 7.5% were neonatal death, and 6% stillborn (8-11). A publication in 1998 by the Nephrology Department of Rush Presbyterian Hospital in Chicago, Illinois (2), established that, in a 4-year period between 1992 and 1995, of 6230 women between the ages of 14 and 44 years (4531 on HD and 1699 on PD) in 930 dialysis centers, only 128 (2%) managed to become pregnant [109 (2.4%) on HD and 19 (1.1%) on PD]. Of these 128 patients, 48 (37.5%) who became pregnant after starting substitution therapy managed to conclude the pregnancy successfully, as did 72.6% of the 57 patients who began dialysis during their pregnancy (2). This is not an encouraging prognosis for pregnancy in patients who are already in renal replacement therapy; however, it seems that prognosis is better for patients who begin dialysis after the onset of pregnancy. In the Central Military Hospital of Mexico, 5 pregnant patients with renal disease, with or without renal function replacement therapy, have been treated over a period of 6 years; 3 were on HD and miscarriage ended their pregnancies; the remaining 2 are the cases herein described.
Choice of Renal Replacement Therapy
Due to anatomical and functional changes that occur during pregnancy and their possible repercussions on the mother and the product, the next question to evaluate is which renal function substitution method is best in this type of patient. The substitution method to begin with (4) is controversial. There are some reports in which PD could have a better outcome, but we did not find comparative, randomized, prospective studies between HD and PD that determine the best method. In our case and considering the scant experience in the management of this type of patient, PD was preferred. With the first patient, we chose the renal function substitution method that we use most often in the Institution and with which we have more experience in patient management. In the second patient, the choice was based on the successful treatment of the first patient.
Dialysis Management and Complications
Further issues to be solved in the optimization of the outcome of pregnancy are adjustments to be made concerning problems secondary to renal disease, adequate dialysis dosage, and special care and complications inherent in pregnancy. In 1997, for the first time, recommendations were published for the most appropriate treatment of these patients (5) (Table 3). Together with the Kidney Disease Outcomes Quality Initiative (K/DOQI) guidelines published by the National Kidney Foundation for management of patients with renal disease, they were the basis for the treatment of both patients.
Guidelines for Optimizing the Outcome of Pregnancy in Patients on Dialysis
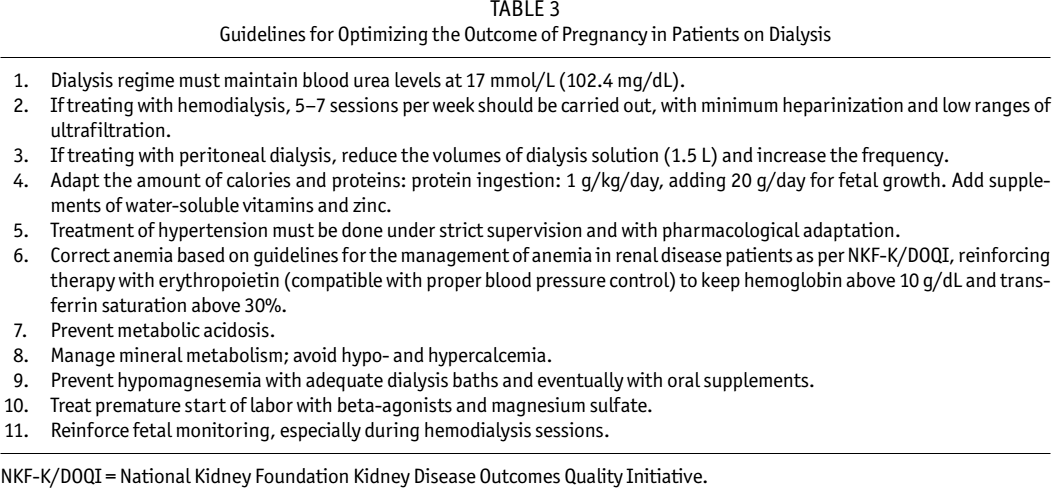
NKF-K/DOQI = National Kidney Foundation Kidney Disease Outcomes Quality Initiative.
Improvements to these initial guidelines have been suggested, such as those proposed by Hou, which include more precise data, such as 20 hours of dialysis/week in the case of HD; strict monitoring of calcium, phosphorus, and magnesium; and, as an objective for adequate fetal development, a target serum bicarbonate level of 18 – 20 mEq/L (11).
The dialysis prescriptions in both patients were with volumes of 1.5 L, and complications appeared only at the beginning of dialysis: abdominal pain in the first patient and leakage in the second. To deal with these problems, progressive volumes of PD solution were used and the length of the dwell time was progressively prolonged.
Both patients’ diets were prescribed following the recommendations of the dialysis guidelines in Table 3. The patients’ weights increased progressively in accordance with their gestational age and, furthermore, serum albumin levels were maintained at a minimum at 4 g/dL (Table 2).
As can be seen in Table 1, the secondary problems common in renal disease were handled in both patients and adequate results were obtained since anemia was resolved, there were no major problems in mineral metabolism management, metabolic acidosis was corrected and maintained above the lower limit proposed for this type of patient as established in the indicated guidelines. In large measure, this was due to the ample urinary volumes maintained. Polyhydramnios, substantiated with obstetrical ultrasound, was the only complication that both patients experienced during gestation on PD. The urinary infections in the patient of the first case were recurrent (4 times) and were always caused by E. coli. In fact, prior to inducement of labor, the patient presented with new symptoms; consequently, the infant had early neonatal sepsis, which was handled successfully with antibiotics. It is important to point out that the blood pressure figures of both patients were normal and no drugs were required to control it.
Finally, both infants were female; only one was premature with low weight and the complication in the first infant was not directly related to ESRD or to its treatment with automated PD.
Conclusions
In this report we point out that managing the progression of CAPD dosage is necessary in order for the mother to adapt progressively. In the particular cases we dealt with, both patients had characteristics that influenced the success of their pregnancies, such as (1) the complications inherent in renal disease in the 2 patients were not very extensive at the time of diagnosis of renal disease; and (2) urine volume was very ample, something that unquestionably contributed to the dialysis dosage being attained without much difficulty. Also, fluid management was very important and, to a large extent, this influenced the fact that neither patient experienced hypertension (12). The products of both pregnancies differed in terms of birth weight, perhaps related to the duration of CAPD: the first patient had 11 more weeks of therapy.
Peritoneal dialysis is the main renal function substitution method in Mexico, and the Central Military Hospital is no exception. In the case of these 2 patients, CAPD demonstrated to be an efficient method to treat their ESRD problems, without major complications arising for either the mother or the fetus during pregnancy.