
Abstract

Current North American recommendations are that physicians disclose mortality data to patients embarking upon dialysis (1); however, only a minority of physicians disclose the information to patients that do not specifically ask for it (2). Although the recommendation (for disclosure) is in keeping with current ethical principles (3) and judicial decisions (4,5), scant data exist to support this recommendation in potential dialysis patients.
Recently we reported in a cohort of patients seen at a nephrology clinic for the first time that patients would want their physician to disclose, without prompting, prognostic information should they require dialysis in the future, whether the prognosis be good or bad (6). Unfortunately, our University Ethics Board would not allow us to study patients with chronic kidney disease (CKD) stages 3 and 4, so that most of the patients studied had little chance of requiring future dialysis. An accompanying editorial (7) recommended that the study be repeated in a CKD cohort. We have repeated this study in a cohort of patients with CKD stages 3 and 4.
Patients and Methods
Patients attending a multidisciplinary CKD clinic were studied. Consecutive patients with CKD stages 3 and 4, calculated from serum creatinine [Cockroft–Gault (8)], were chosen. Patients were excluded from the study if, in the view of the MD, a significant language barrier existed, the patient was medically or psychologically unstable, or if it was deemed that educational levels precluded meaningful understanding of the questionnaire. A research nurse obtained written consent. The questionnaire was completed in the clinic without further input from the research nurse.
Full details of the questionnaire are given in our previous publication (6). This research project was approved by the Health Research Ethics Board of the University of Manitoba.
Results
Of the 127 patients screened, 105 consented and 100 of these completed the questionnaire; 72% had stage 4 CKD and 28% had stage 3 CKD. Mean age was 66 ± 16 years, with 42% females; 28% of patients had been to renal education classes, 53% had received some instruction at the clinic, and 17% had had no teaching; 46% of patients had not graduated from high school, 29% had post high school education; 37% of patients knew someone on dialysis.
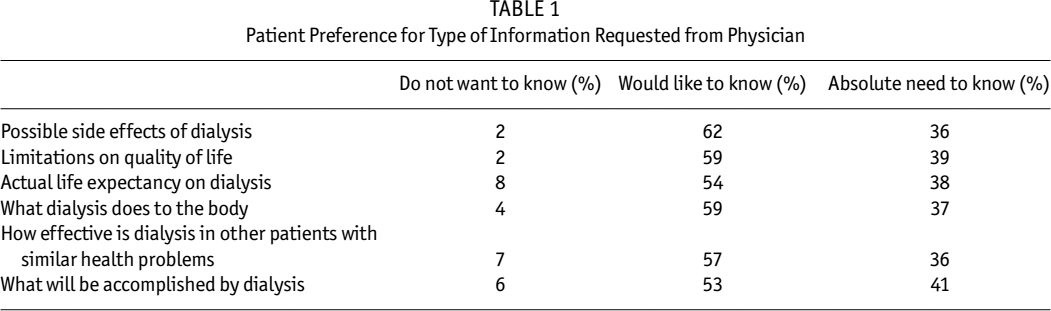
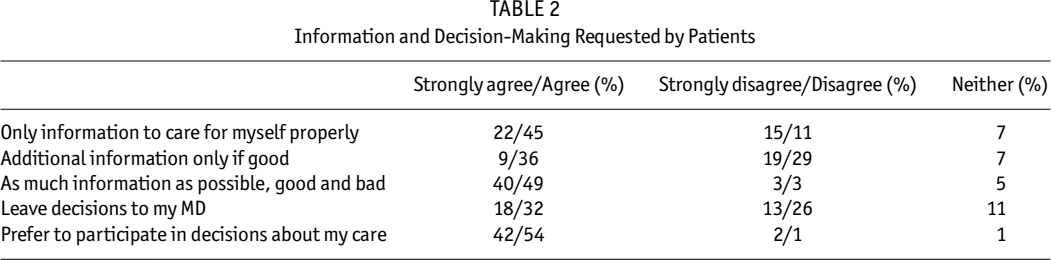
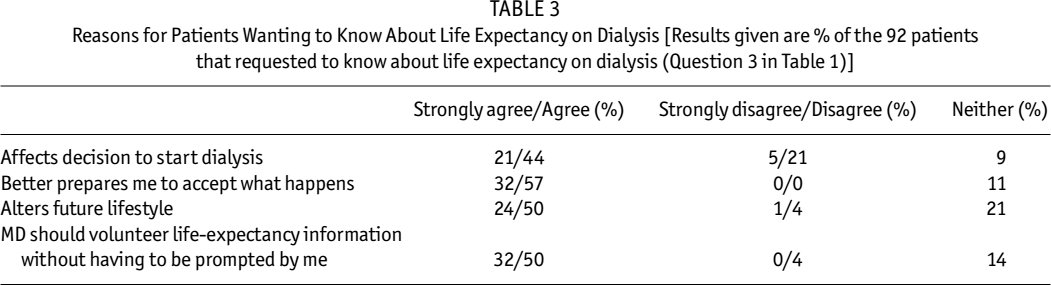
The responses to the questionnaire are given in Tables 1 – 3. Most (92%) patients wanted to know life expectancy on dialysis; 98% wanted to know limitations on quality of life on dialysis; 89% of patients wanted disclosure of as much information as possible, whether good or bad. The most common reason (89%) for wanting disclosure of life expectancy was to be better prepared to accept what happens on dialysis; 82% of patients wanted their physician to disclose life expectancy without having to be prompted. There were no apparent differences between the responses from those who had attended renal education classes and those who had not been exposed to any educational activities (the nature of these data preclude statistical analysis).
Patient Preference for Type of Information Requested from Physician
Information and Decision-Making Requested by Patients
Reasons for Patients Wanting to Know About Life Expectancy on Dialysis [Results given are % of the 92 patients that requested to know about life expectancy on dialysis (Question 3 in Table 1)]
Discussion
The results are virtually identical to those obtained from general nephrology patients (6) but are more relevant because all the patients were aware of needing dialysis in the future. The results demonstrate that the vast majority of (Canadian) patients want disclosure of relevant morbidity and mortality data without having to prompt the physician. Fully informed patients may well be able to cope better with the vicissitudes of life on dialysis.
A full discussion of the issues raised by our findings has been given in our previous paper (6).
In summary, our findings are in keeping with American Society of Nephrology guidelines (1), observations in other conditions such as cancer (9,10), and legal opinions (4,5). Indeed, because of the latter, physicians not performing this duty could be charged with negligence or failure to meet professional standards (11).
Our study demonstrates a dichotomy between what patients want and what they obtain (2) with respect to full disclosure. To continue current practice could be construed as paternalistic. By contrast, informed decision-making has been described as an “essential ingredient of good patient care” (3).
Footnotes
Acknowledgment
This research was supported by an unrestricted grant from Baxter Canada.