
Abstract
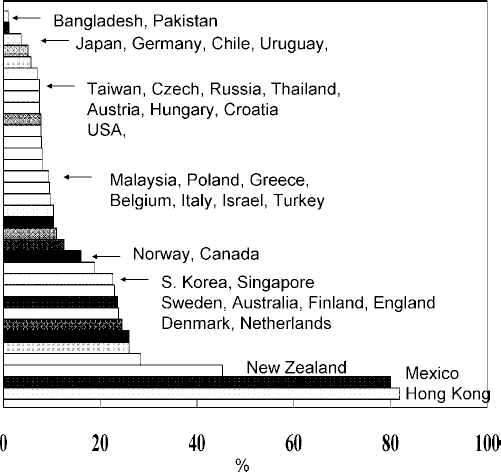
The percentage penetration for peritoneal dialysis among prevalent dialysis patients in the year 2003. Data are derived from the U.S. Renal Data System report, the European Dialysis and Transplant Association report, the U.K. Renal Registry report, and the Hong Kong Renal Registry report.
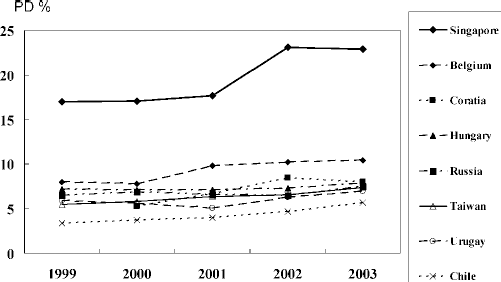
Countries with a rising trend of percentage peritoneal dialysis (PD%) penetration among prevalent patients.
Discussion
Declining PD Utilization Trend
In contrast with the rising trend in Asia, PD utilization is seen to be declining in North America, many Western European countries, and Australia and New Zealand (Figure 3). The reasons for this decline have not been well studied and may vary between countries.
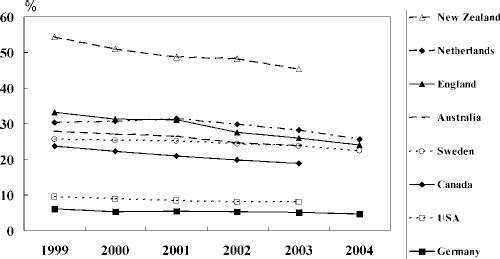
Countries with a declining trend of percentage peritoneal dialysis penetration among prevalent patients.
In the United States, PD utilization rose from the 1980s until the mid-1990s. From the mid-1990s, PD penetration progressively declined to 8% from 15%, coinciding with the publication in 1997 of the U.S. National Kidney Foundation (NKF) Dialysis Outcomes Quality Initiative (DOQI) guideline on adequacy of peritoneal dialysis. Many believe that the DOQI guideline contributed to the decline in PD utilization because the minimal weekly Kt/V target of 2.0 cannot be reached easily in many patients. As a result, patients were shifted away from PD to HD. It should be noted that the minimal weekly Kt/V target has been re-adjusted to 1.7 in all 2005 and 2006 published guidelines [European Best Practice Guidelines, NKF Kidney Disease Outcomes Quality Initiative (K/DOQI), and the International Society for Peritoneal Dialysis (ISPD)] (3-5).
PD Outcome: Patient Survival
Another negative factor affecting PD utilization may be the data from reported survival studies.
Debates are ongoing about the survival comparison between PD and HD. Theoretically, large-scale randomized controlled trials (RCTs) should provide the best answer, but unfortunately, no such RCTs are available. The report from Korevaar et al., in which only 38 of 773 patients were willing to be randomized, indicated that launching another RCT of sufficiently powered sample size will be quite impossible in the near future (6). Reliance on survival reports or registry analysis studies will be the norm, but the conclusions from those types of reports often vary and may even contradict one another.
Table 1 shows a summary of survival comparison conclusions from various reports (7-18). The variations are probably related to differences in patient type, case mix, modality selection criteria, and even the practice of PD.
Summary of Survival Reports Comparing Peritoneal Dialysis (PD) Patients with Hemodialysis Patients a
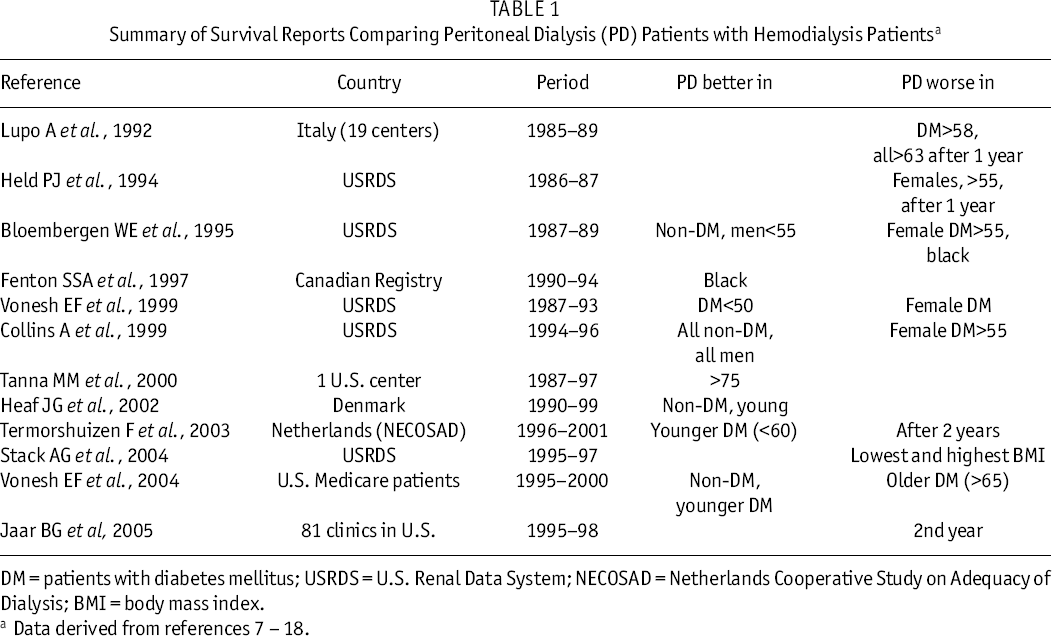
DM = patients with diabetes mellitus; USRDS = U.S. Renal Data System; NECOSAD = Netherlands Cooperative Study on Adequacy of Dialysis; BMI = body mass index.
Data derived from references 7 – 18.
In 1997, using the Canadian Renal Registry, Fenton et al. reported better survival for PD patients in the first 4 years of dialysis (10). This finding of better survival of PD patients in the first few years has subsequently been confirmed by many other reports, although the period of initial survival advantage varies (12,14,15). The foregoing data formed the basis for the “PD first” policy. But such findings did not positively affect the PD utilization rate in the Western world. The fact that the PD survival rate becomes similar to the HD rate after a few years means that risk of death for PD-to-HD patients increases with time. And so, despite overall survival for PD patients during the first 5 years still not being inferior to HD [as indicated by the latest U.S. Renal Data System (USRDS) report], the increase in mortality risk for PD over time as compared with the risk for HD has been emphasized in many survival reports and has become a negative factor weighing against the choice of PD for many doctors.
This selective attitude in translating survival data into practice is also reflected in subgroup survival analysis and utilization. Although some reports show that PD may be a worse choice in older and diabetic patients (19), there is little argument about the better survival of young and nondiabetic PD patients—and yet PD utilization continues to decline in young and nondiabetic patients in the United States (20).
Improvement in PD Patient Outcome
The USRDS report for 2005 compared 5-year survival data for two cohorts of patients who started dialysis during 1989 – 1993 and during 1994 – 1998 (21). An overall improvement in 5-year patient survival was observed for the cohort of patients started dialysis during 1994 – 1998 as compared with the 1989 – 1993 group, with the greatest improvement being seen in the PD patients (PD 14%, HD 9%, transplant 9%). In the same report, the 5-year survival for nondiabetic PD patients in the 1994 – 1998 cohort exceeded the survival for a parallel group of HD patients. Moreover, among diabetic patients, although survival on PD still fell below survival in the HD counterpart group, the difference was much smaller than in the comparable 1989 – 1993 cohorts. The younger age group (20 – 44) of PD patients clearly had a lower cumulative probability of death at 5 years, and in the other age subgroups (45 – 64, 65 – 74, 75+), the probability was very similar to that for the HD patients.
The exact cause of the survival improvement was not discussed in the USRDS report, but may be related to the attention paid to adequacy of dialysis after the mid-1990s. If the trend of improvement in the survival of PD patients over HD patients dialyzed after 1998 persists, even better survival for PD patients over HD patients may be expected to appear. With the availability of icodextrin peritoneal dialysate in the United States since 2002, further improvement in outcome is anticipated. A few more years’ wait for more update data on patient survival in the 2000s will tell the tale.
Better Survival in Asian PD Patients
It has to be pointed out that the USRDS survival data cannot be generalized to other parts of the world. Asian patients—whether on PD or HD, and whether living in Asia or in North America—are well recognized to experience better survival than Caucasians do (22-24). The 2-year patient survival of PD patients in Japan, Korea, and Hong Kong was between 80% and 90%. It was about 70% – 80% in many European countries and even lower in North America (Figure 4). However, few published analyses have compared the survival of PD and HD patients from Asian countries.
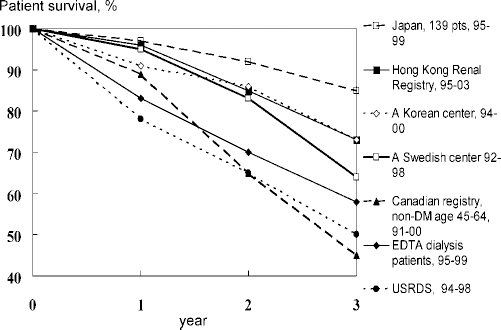
Unadjusted patient survival rate of peritoneal dialysis (PD) patients in various parts of the world. Data are derived from the U.S. Renal Data System (USRDS) report, the European Dialysis and Transplant Association (EDTA) report, and the Hong Kong Renal Registry report. No national registry data from Japan are available. The Japanese data presented here were extracted from a multicenter study on eight dialysis centers (27). In Korea, PD registry data are available only for patients who star ted dialysis from 2001 onwards, and the data for Korea come from reference 26. The one Swedish center result was also retrieved from reference 26. non-DM = patients without diabetes mellitus.
A recent publication from a single center in Taiwan showed superior survival for PD patients over HD patients, with or without diabetes (25). These data suggest that Asian PD patients can have better survival than HD patients do. On the other hand, Caucasian patients on PD may do as well as Asian patients, as reported in a direct comparison of patient survival from a Korean and a Swedish PD center (26).
The real questions are “Why?” and “How?” What are the factors that produce better survival in Asian patients, and can those differences be overcome? More studies need to be conducted to shed light on this issue.
PD Costs Less than HD
As has been seen, survival data do not provide strong support for the decline in the PD utilization rate. Could the decline be attributable to non-medical factors?
In terms of patient choice, studies have shown that, if given an adequate explanation of the pros and cons of PD and HD well before dialysis, close to 50% of patients would choose PD and that patients who receive counseling are more likely to choose PD (28). Unfortunately, patients may not be given an optimal education in dialysis modality selection, or the option of PD may not be available to them in many dialysis programs.
In terms of cost, PD is generally cheaper than HD in most developed, and even in many less developed, countries (Table 2). In the United States, the annual cost per patient for PD is only about 70% of the cost for satellite HD, but this cost benefit does not translate into utilization choice. Therapy with PD is cheaper, because it is home-based, with many fewer clinic attendances; but, unfortunately, PD then usually generates less income for the clinics, hospitals, and doctors because of its less frequent clinic visits and treatments on which payment or reimbursement is often based. These factors reduce the financial incentive for nephrologists and center administrators to put patients on PD, which is believed to be a major reason for the low PD utilization rate in many countries.
Cost Comparison (US$ per Patient–Year) Between Hemodialysis (HD) and Peritoneal Dialysis (PD) in Various Countries a
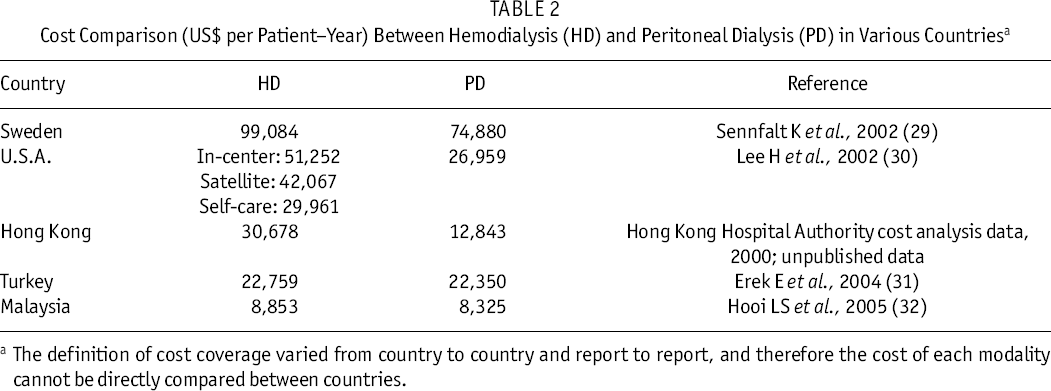
The definition of cost coverage varied from country to country and report to report, and therefore the cost of each modality cannot be directly compared between countries.
Conclusions
The decline in PD utilization is unjustified from both a medical and a non-medical point of view. It must therefore be related to many identified or unidentified factors, particularly non-medical factors. Full investigation into these factors is warranted. To improve PD utilization, survival analyses need to be further updated, reimbursement and payment systems must change to favor home dialysis therapy, dialysis facilities need the appropriate set-ups and expertise for PD, the structure and content of pre-dialysis patient education must change, and of course PD therapy and care must continue to be improved.