
Abstract
Epidemiology
The numbers of infants needing dialysis are small— although in centers with a high incidence of congenital nephrotic syndrome, they may represent one third of the pediatric ESRF population (7). In the United Kingdom, numbers varied between 15 and 27 in any year during 1988 – 1997, an annual incidence of 3 per 1 million population (8). These figures are comparable to those in the United States, where 6 new patients per 1 million population of the same age start dialysis each year (9).
The real incidence of severe renal-tract abnormalities is not known because no details have been published of the numbers of related spontaneous abortions and pregnancy terminations or of the numbers of infants with severe comorbid conditions who are not referred for RRT. However, it does seem that parents are increasingly expecting all available treatments to be offered to their infants. In a study of 20 infants starting peritoneal dialysis (PD), more than half of the families had been offered termination of pregnancy and all had refused, including two families who subsequently went on to refuse RRT (3).
Diagnoses
Diagnoses are predominantly structural abnormalities of the urinary tract such as dysplasia with or without reflux or obstruction (60% – 80%). Congenital nephrotic syndrome is the next most common diagnosis, and cortical necrosis is the third. Thereafter, small numbers of infants are diagnosed with autosomal recessive polycystic kidney disease and renal venous thromboses, and then come even smaller numbers of diagnoses of conditions more commonly seen in older children (2,8).
Over the last few years, the percentage of infants whose renal abnormality is diagnosed antenatally has risen to more than 50%, but earlier discovery has had little impact on either the incidence or spread of diagnoses, which have both remained stable (8).
Issues Specific to the Management of Infants with ESRF
In addition to all the problems that affect older children, other specific issues arise concerning infants who require RRT:
Is RRT justified?
Which RRT modality should be chosen?
How are nutrition and growth to be managed?
Justification for RRT
Whether to initiate RRT is one of the most difficult questions facing pediatric nephrologists (10), and the ethics surrounding withdrawing or withholding treatment have been eloquently discussed (6,9). That decision is a particular issue for infants with other co-existing congenital abnormalities, who represent about one third of the infant renal failure population.
In 20 infants on PD at our center, 14% had developmental delay; 7%, congenital heart disease; 3%, gut problems; 2%, hypothyroidism; 2%, respiratory problems; and 2%, blindness and deafness. There were also individual cases of CHARGE and VATER association, Wilms tumor, and other syndromes (Down, Jeune, Alagille) (2). Such abnormalities contribute to morbidity and mortality in their own right, and these infants are the ones who do particularly badly on RRT.
Some families may decide that they do not wish to inflict further pain and suffering on their infant, and they choose conservative management rather than RRT. In the United Kingdom, about 3 families choose this option each year (8). Arriving at such a decision requires careful counseling (6). In addition to comorbidity, factors that are important in influencing decision-making include pulmonary hypoplasia and oliguria, which also limit survival (2,8,11-14). On the other hand, many infants, particularly those with congenital structural abnormalities, are polyuric, and so the ongoing electrolyte and water losses mean that such infants may survive many months even if untreated—but at considerable cost to their growth and development. Furthermore, some improvement in renal function may occur over the first year of life, as in normal infants, and so outcome may be difficult to predict. Indeed, some are able to come off dialysis—as many as 4% in a U.K. series (8). Parental bonding with an infant can lead to reversal of a decision for conservative management, by which time irreversible damage to growth and development may have occurred.
Some families opt for intensive management of their infant, with dialysis and early transplantation. However, even in a child with no comorbidity, the input required from the family and multidisciplinary team (emotional, time-related, and financial) cannot be overestimated. Nonetheless, strict attention to nutrition, the dialysis program, and medications can result in a successful outcome for the infant with ESRF.
It has to be remembered that, because of the very rapid growth in children of this age, only very frequent contact with the family can ensure adequate dialysis and nutrition. For example, the expected weekly weight gain during the first 6 months of life is 200 g—that is, over a week, an infant weighing 3.8 kg should increase in weight to 4.0 kg. Based on a daily feed volume of 150 mL/kg, the daily feed should increase from 570 mL to 600 mL. Estimates suggest that 6 contacts per month by a dietitian are necessary per patient in children under 5 years of age, and so even more contacts are likely to be required in infants (15). Furthermore, if the dialysate fill volume is 40 mL/kg, then over the course of the week, that volume should increase from 152 mL to 160 mL. It can therefore be seen that, without frequent medical, nursing, and dietetic attention, the infant on PD will rapidly become underdialyzed and underfed.
Most infants will go home dialyzed by cycling machines overnight and with feeds that are administered both during the day and overnight by feed pump. These factors, together with medication administration and the need to be able to assess the importance of small changes in weight and blood pressure, present a huge burden for the family. Although some infants managed with such intensity may start dialysis and run a course that is relatively straightforward until transplantation, escaping complications entirely is rare.
Choice of RRT Modality
The purpose of RRT is to optimize growth to allow early transplantation, which has been shown to be successful even in patients under 2 years of age (16). However, ensuring that vaccinations are complete is important, and so transplantation before 15 months of age is unusual.
In the United Kingdom, overnight cycling PD is selected in more than 80% of infants (8). This choice stems from the difficulty of obtaining vascular access for hemodialysis (HD) in small blood vessels and from the need to prime HD lines with blood, which confers a risk of HLA sensitization. Problems in maintaining vascular access are also very common. We found a revision ratio of 40% in 18 infants on long-term HD. Furthermore, although growth rates are maintained, the catch-up seen on PD is not evident (17).
Access complications are less common in PD, although at our center, 35 catheters were placed in 20 infants over a mean of 17.3 months, and 24 episodes of peritonitis occurred in the 20 infants, 10 of whom required catheter replacement once, and 2 of whom required replacement twice (3). Ultrafiltration failure occurred in 4 infants who had to transfer to HD. Peritoneal dialysis is easier to establish, and the ability of automated PD to deliver short cycles, high dialysate flow rates, and high intraperitoneal volumes make it particularly good for the high fluid intake of the infant diet. Readers are referred to two excellent reviews of the practicalities of PD management in infants (7,18).
Nutrition and Growth
Only during fetal life is growth as rapid as during infancy. Growth rates at birth can exceed 25 cm per year, falling to an average of 18 cm per year at 12 months of age, and 10 cm per year by the age of 2 years. Half of adult height is achieved by the age of 2 years, and so irrecoverable loss of growth potential can occur during this phase.
Nutrition is particularly important during the infant phase, when growth is less dependent on growth hormone than during the childhood and pubertal phases. At birth, 170 kcal are stored in new tissue daily. That number falls to 50 – 60 kcal at 6 months, 30 – 40 kcal by 12 months, and 20 – 30 kcal by the age of 2 years. These requirements can be difficult to achieve because of anorexia, vomiting, and episodes of poor intake attributable to infections and urologic procedures (19).
Table 1 shows the U.K. daily dietary reference values for energy and protein for normal children and the recommendations for children on PD (19). There is no evidence to suggest that energy requirements for infants on PD should be any higher than those for normal children. Indeed up to 12 kcal/kg may be obtained daily from the glucose in dialysate, and that intake should be considered when calculating feed requirements (20). If the child is below the 2nd percentile for height, using the estimated average requirement for height–age is advisable to ensure adequate energy intake.
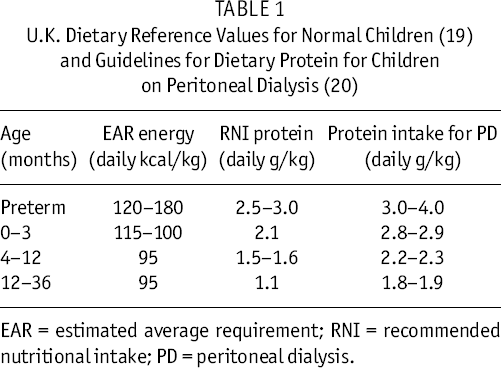
EAR = estimated average requirement; RNI = recommended nutritional intake; PD = peritoneal dialysis.
Protein requirements for infants on PD are higher than those for normal infants, and these young patients are at greater risk of protein malnutrition than are their peers treated with HD (21) because of an inverse correlation between peritoneal surface area and peritoneal protein losses. Infants have nearly twice the peritoneal protein losses per square meter of body surface area than do children weighing more than 50 kg. Such protein losses will impair normal growth if not replaced and may contribute to permanent loss of growth potential (22). Prescribing a protein supplement to reach the normal dietary requirement for all children on PD is therefore usual—again using the recommended protein intake for height–age if the child is below the 2nd percentile for height.
Feeds can be based on a normal, complete, whey-based infant formula [SMA Gold (SMA Nutrition, Maidenhead, U.K.), Cow & Gate Premium (Nutricia, Trowbridge, U.K.)] or, rarely, a low-potassium feed [Kinder-gen PROD (SHS International, Liverpool, U.K.)], supplemented with energy either as a glucose polymer [Maxijul (SHS International) or Caloreen (Nestle, Vevey, Switzerland)] alone or in combination with a long-chain fat emulsion [Calogen (SHS International)] or a combined fat and carbohydrate product [Duocal (SHS International)]. Protein can be supplemented as a whey protein concentrate with amino acids [Maxipro (SHS International)]. The reader is referred to a review of nutrition for vitamin and mineral requirements (19).
In many infants, achieving adequate intake is not possible without supplemental feeding, either by nasogastric tube or gastrostomy. Many infants with chronic renal failure have abnormal gastric motility, delayed gastric emptying, and gastroesophageal reflux, and as much as 30% of feeds may be lost with the associated vomiting (23). The use of ranitidine or prokinetic agents such as domperidone may help. However, if vomiting is so severe as to compromise nutrition, Nissen fundoplication and gastrostomy are indicated.
In our center, more than 50% of infants on PD are managed with gastrostomies, and nearly 50% of those, with Nissen fundoplication (2,3). Complications of gastrostomy are uncommon, but include gastrocolic fistula and paraesophageal hernia. It is preferable to undertake gastrostomy before PD starts, because the risks of post-surgical peritonitis, exit-site infection, and dialysis catheter removal are increased if this surgery is undertaken after PD has started. The risk may be reduced if open surgery rather than percutaneous placement is used (24,25). After removal, the track usually closes spontaneously.
Renal Osteodystrophy
Calcium requirements are relatively high in the rapidly growing infant. Also, care must be paid to the premature infant, who may have rickets of prematurity. Our center aims to maintain phosphate just below the 50th centile for age through dietary phosphate restriction [<400 mg (13 mmol) daily] and use of calcium carbonate or acetate. Parathyroid hormone is titrated against the lowest possible dose of activated vitamin D (0.01 μg/kg daily), with the aim of maintaining levels within the normal range as far as is achievable. In our infants, 79% had a parathyroid hormone level within the normal range after 1 year of PD (3).
What is the Long-Term Outcome?
Mortality
The mortality rate in infants starting dialysis is as much as 4 times that of children beyond infancy (27), with most deaths occurring in the first year of life. A 1-year survival of about 85% was reported by the North American Pediatric Renal Transplant Cooperative Study and a U.K. series, as compared with 95% in children starting dialysis after infancy (2,28). That higher death rate persists, survival rates being 74% and 68% after 2 and 3 years respectively, as compared with 90% and 86% in children who start dialysis at older ages. No increase in mortality is observed in infants starting dialysis in the first month of life (8).
Death may be attributable to treatment withheld, treatment withdrawn, or death on dialysis. Most infants in whom treatment is never started die within 1 year, and most of those deaths (more than 70%) occur in infants with associated comorbidity. A significant incidence of comorbidity (more than 50%) is also seen in patients in whom treatment is withdrawn; although, in some, the withdrawal occurs because of an unacceptably poor quality of life. Again, most of the deaths occur within 1 year. Causes of death in children actively treated with dialysis are similar to those reported in older children, predominantly sepsis or biochemical or fluid-related disturbances, and no difference in outcome is evident in infants who are otherwise normal in comparison with older children (2,8). The life expectancy for these infants is unknown; it is possible that the complications that develop after years of RRT will simply occur at a proportionately earlier age.
Growth
Severe growth retardation can occur even before an infant is referred to a pediatric nephrology service. Growth retardation can have a long-lasting effect on height potential. Approximately one third of the reduction in height occurs during fetal life. Another one third occurs during the first 3 months following birth and is accompanied by a similar decline in head circumference (29-31). However, infancy is when the potential for catch-up growth, with intensive nutritional input, is at its greatest.
In 20 infants starting PD, we reported an improvement in height and weight standard deviation scores (SDSs) to, respectively, –1.1 and –0.3 at 1 year and –0.8 and 0.3 at 2 years from –1.8 and –1.6 at baseline (3). Over a similar time frame, 13 infants on PD showed a change in height SDS to -1.24 from –2.17 (2). Other centers have also reported catch-up growth in infants on PD, although an initial decline followed by stabilization of growth, no change, and a declining height SDS have also been reported (19). Poor nutritional status and growth are associated with starting PD at a younger age (32). Interestingly, infants who grew well continued with catch-up in early childhood (2,33).
Development
Clearly, the developmental outcome is more likely to be adverse if renal failure is associated with a disorder such as neonatal hypoxia or certain syndromes and chromosomal abnormalities. Malnutrition can also compromise head growth; although, with intensive nutrition, an increase in head circumference to –1.3 at 6 months and –0.9 at 1 year from –1.9 at baseline was observed in our center's 20 infants (3).
Overall, reports demonstrate relatively good outcomes. Of 28 survivors among 34 infants dialyzed before 3 months of age, only 1 was significantly delayed at 1 year of age. Of the 16 that reached 5 years of age, 15 were attending regular school (34). In our unit, 85% of infants had developmental scores within 2 standard deviations of the mean (mean IQ: 87), but 50% demonstrated borderline abnormal psychosocial adjustment (35).
In a U.K. infant series of 105 children old enough to assess, 91 attended a regular school or were expected to, although 16 required individual support. The other 14 attended special schools, 11 for developmental and emotional needs and 3 for physical reasons (8).
Conclusions
It can be expected that, during childhood, approximately one third of infants with ESRF will die, nearly half will undergo transplantation, and the rest will have returned to dialysis. If survivors are to achieve the best possible outcomes, attention must be paid to nutrition, prevention of renal bone disease, preservation of dialysis access sites and the peritoneal membrane, and most importantly, provision of support to the families of these infants.