
Abstract
Keywords
More liberal acceptance criteria for dialysis is a major factor contributing to the rapid growth of the elderly dialysis population (6,7). The comparable outcomes in elderly and younger dialysis patients have made nephrologists aware that older age is, in itself, no longer a reason for not accepting elderly patients for renal replacement therapy (8-10). A previous survey also showed that 84% of elderly patients would choose dialysis treatment and that 74% of them would prefer home dialysis if they had been well informed about the nature of end-stage renal disease (ESRD) and treatment options (11).
The aging population has significant implications for the community; the increase in elderly dialysis patients poses special challenges for the renal team. Medical and social issues both have to be considered in providing appropriate care to elderly dialysis patients.
Most continuous ambulatory PD (CAPD) patients perform their exchanges at home by themselves. The success of CAPD relies mainly on the exchange technique. Elderly people have physiologic changes related to normal aging, and certain common health problems—anxiety, depression, dementia, and eye problems, for example—occur frequently. A previous study showed a high prevalence of cognitive impairment in elderly CAPD patients (12).
Some nephrologists may be reluctant to start CAPD for elderly ESRD patients because of worries about their ability to perform self-care CAPD. Elderly patients who cannot adequately perform self-care CAPD need either good family and social support for assisted CAPD or long-term institutional care.
To obtain a clearer picture about clinical outcome in elderly CAPD patients, we carried out a retrospective study of all patients who started CAPD over a 5-year period in a single PD unit in Hong Kong. We also investigated the effectiveness of self-care CAPD in elderly ESRD patients.
Patients and Methods
Patients
All patients newly diagnosed with ESRD who started CAPD between 1 January 2000 and 31 December 2004 in a single renal center in Hong Kong were included in the study. Every patient was assessed individually for likelihood to benefit from a CAPD program. Under Hong Kong's “PD first” policy, PD is arranged for all patients who need dialysis support and who have no contraindications to PD.
Patients who started CAPD during the study period were divided into two groups based on age: patients who had reached at least the age of 65 years at the start of CAPD were included in the elderly group, and patients under 65 years of age at the start of CAPD were included in the control group. Patients were not included in the study analysis if
they had been withdrawn from CAPD by nephrologists within 90 days of treatment start, for reasons unrelated to PD complications.
they had been transferred into our unit after their CAPD training.
they had been referred out to another unit within 90 days of CAPD start.
To investigate the effectiveness of self-care CAPD in elderly patients, the patients in the elderly group were further divided into two comparison groups based on their ability to perform their own CAPD exchanges: a self-care CAPD group, and an assisted CAPD group. The patients were followed until death, permanent switch to hemodialysis, renal transplantation, withdrawal from CAPD, or study end (1 January 2006), for a minimum follow-up of 12 months.
Data Collection
We retrieved pertinent information from the hospital records of all patients who started CAPD between 1 January 2000 and 31 December 2004, including case notes and data from the hospital database. The first day of CAPD training was accepted as the study entry date. Baseline demographic and clinical data retrieved included age, sex, underlying renal disease, weekly total Kt/V, normalized protein catabolic rate (nPCR), residual renal function, serum albumin level, CAPD connection system, duration on CAPD, use of a helper for exchanges, and length of CAPD training in days. Outcome measures included patient mortality, technique failure, peritonitis episodes, and training duration in days.
Statistical Analysis
We used the SPSS software package (SPSS, Chicago, IL, U.S.A.), version 12.0, for statistical analysis and deemed p < 0.05 to be statistically significant. Results are expressed as mean ± standard deviation unless otherwise stated. Baseline demographic data, baseline clinical data, and training data were compared between groups by the chi-square test, Fisher exact test, t-test, or Mann– Whitney U-test, as appropriate. Patient survival, technique survival, and peritonitis-free period were analyzed by the Kaplan–Meier life-table method, and we assessed the differences between groups by the log rank test.
Results
Demographic and Baseline Clinical Data
Over the 5-year period, 328 patients (170 men, 158 women) met the study criteria. Median age of the patients at the start of CAPD was 60 years. The elderly group consisted of 121 patients, and the control group, of 207 patients. Table 1 shows demographic and baseline clinical data for the study patients.
Demographic and Baseline Clinical Characteristics of the Incident Elderly and Control Patients on Continuous Ambulatory Peritoneal Dialysis, 1 January 2000 – 31 December 2004
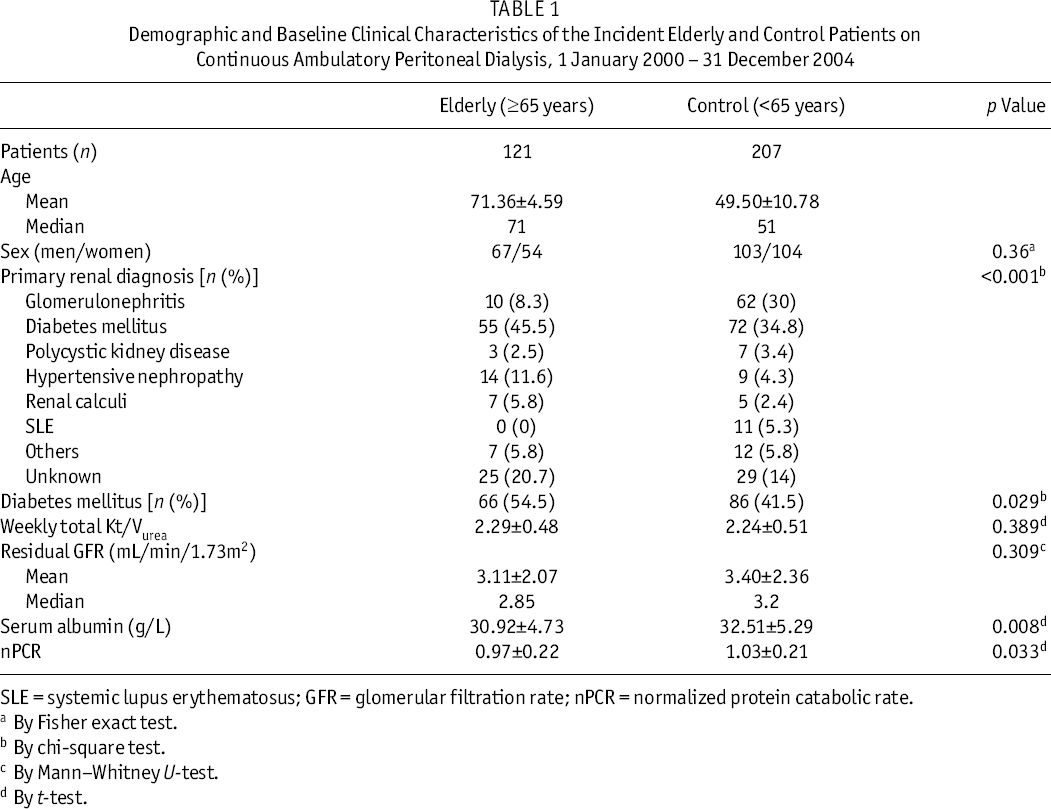
SLE = systemic lupus erythematosus; GFR = glomerular filtration rate; nPCR = normalized protein catabolic rate.
By Fisher exact test.
By chi-square test.
By Mann–Whitney U-test.
By t-test.
We observed no significant difference in weekly total Kt/V (p = 0.389) and residual renal function (p = 0.309) between the elderly group and the control group. However, the patients in the elderly group had a significantly lower level of serum albumin (p = 0.008) and of nPCR (p = 0.033) than did the patients in the control group. Elderly patients in this study more often had diabetes as the underlying primary cause of renal failure. Patients in the control group more often had glomerulonephritis and systemic lupus erythematosus as the underlying renal disease. The elderly group had a significantly higher prevalence of diabetes (p = 0.029).
Comparisons of Clinical Outcome
Figure 1 shows the Kaplan–Meier curves for cumulative patient survival, technique survival, and peritonitis-free period in the elderly and control groups. We observed no statistically significant difference between the elderly group and the control group in any of the three outcomes. The 2-year and 5-year rates of patient survival were 89.3% and 54.8% respectively in the elderly group and 92.2% and 62.9% in the control group [p = 0.19,Figure 1(a)]. The 2-year and 5-year rates of technique survival were 84.0% and 45.7% respectively in the elderly group and 80.9% and 49.1% in the control group [p = 0.75,Figure 1(b)]. The probability of a 12-month peritonitis-free period was 76.6% in the elderly group and 76.5% in the control group [p = 0.75,Figure 1(c)].
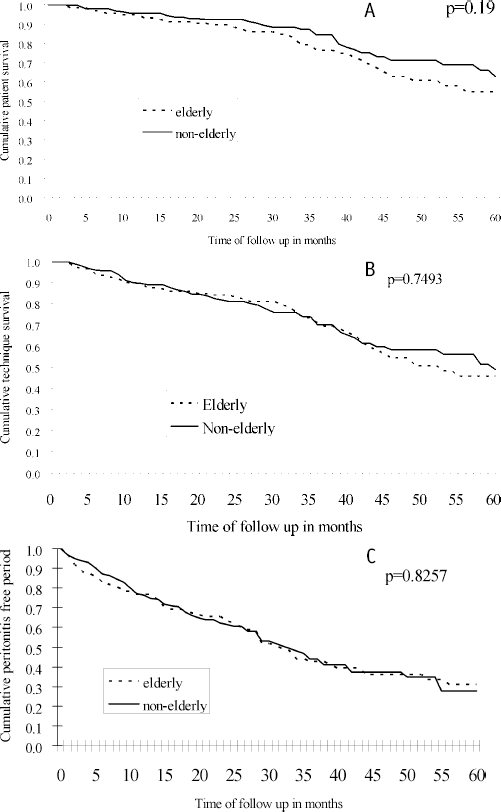
(a) Kaplan–Meier analysis of patient survival for elderly and control patients on continuous ambulatory peritoneal dialysis (CAPD). (b) Kaplan–Meier analysis of technique survival for elderly and control patients on CAPD. (c) Kaplan– Meier analysis of peritonitis-free period for elderly and control patients on CAPD.
Figure 2 compares elderly self-care CAPD patients and elderly assisted CAPD patients with regard to cumulative patient survival, technique survival, and peritonitis-free period. We observed no statistically significant difference between the elderly self-care CAPD and the elderly assisted CAPD patients. The 2-year and 5-year rates of patient survival were 88.3% and 56.4% respectively in the self-care group and 95% and 36.6% in the assisted group [p = 0.81,Figure 2(a)]. The 2-year and 5-year rates of technique survival were 84.7% and 48.3% respectively in the self-care group and 80.9% and 26.0% in the assisted group [p = 0.44,Figure 2(b)]. The probability of a 12-month peritonitis-free period was 77.7% in the self-care group and 71.4% in the assisted group [p = 0.61,Figure 2(c)].
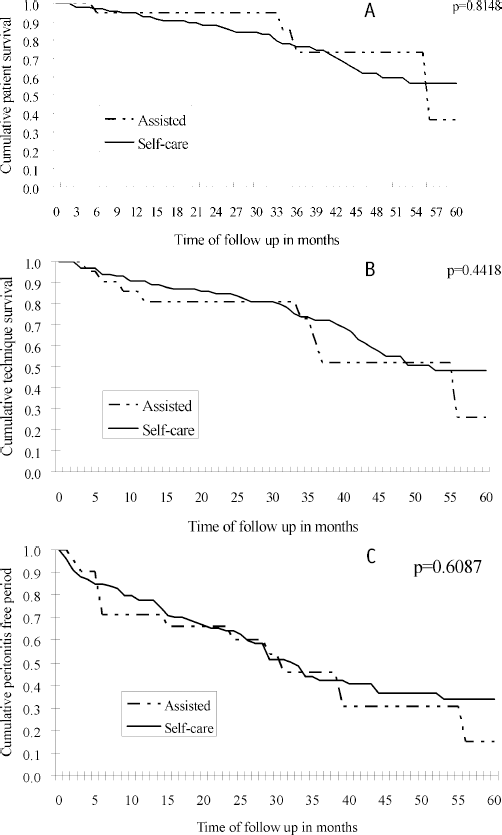
(a) Kaplan–Meier analysis of patient survival for the self-care and assisted-care groups of elderly patients on continuous ambulatory peritoneal dialysis (CAPD). (b) Kaplan– Meier analysis of technique survival for the self-care and assisted-care groups of elderly patients on CAPD. (c) Kaplan–Meier analysis of peritonitis-free period for the self-care and assisted-care groups of elderly patients on CAPD.
Training and Ability to Perform Capd
All patients except one were put on double-bag disconnect systems [the single exception was on the UV-Flash system (Baxter Healthcare Corporation, Deerfield, IL, U.S.A.)]. Of the patients in the study, 294 could perform their exchanges by themselves, including 100 (55 men, 45 women) of the 121 patients (82.6%) in the elderly group, and 194 (99 men, 95 women) of the 207 patients (93.7%) in the control group. More elderly patients needed a helper for performing CAPD (17.4%, p = 0.002). For the self-care CAPD patients, the median training period required in the elderly group was 5 days, which was significantly higher than the 4 days required in the control group (p < 0.001).
Discussion
Choosing the appropriate dialysis modality is important in elderly ESRD patients who are unlikely to receive a renal transplant and who will live on dialysis until the end of life.
A frequent concern in the care of elderly ESRD patients is their ability to have an independent life on dialysis. A previous study in a renal unit with a “PD first” policy for elderly patients found that 84.6% of their PD patients used home PD, but that 94.9% of the patients required a helper for exchanges (13).
Our study showed a high percentage of elderly self-care CAPD patients (82.6%). This phenomenon can be explained by local factors, including a “PD first” policy and other cultural factors. Chinese have strong family cohesiveness and prefer to stay at home with family until they become dependent on others for their activities of daily living. Chinese do not like to feel that they are burden to others, and so that trait would make our patients keener to perform self-care CAPD. Another possible reason for the high proportion of self-care CAPD patients in our study may be our definition of elderly as ≥65 years of age [the earlier study defined elderly as ≥75 years (13)].
Because training was one of the outcome measures in the present study, we excluded from the analysis patients who had been transferred into our unit after their CAPD training. We also excluded patients that had been transferred out to other units and those in whom dialysis had been withdrawn by a nephrologist within 90 days of CAPD start for reasons unrelated to CAPD complications. We chose the latter exclusion criteria to meet the standard definition of 90 days of continuous dialysis for chronic patients; this choice was important because we included survival as an outcome measure. Early deaths (within the first 90 days) are typically attributable to pre-dialysis factors rather than to dialysis modality (14).
Of the patients newly accepted into the CAPD program during the 5-year study period, 36.9% belonged to the elderly group. The major primary renal diagnoses in this cohort of patients were diabetes mellitus and glomerulonephritis. The pattern of age distribution and the underlying renal diagnoses for patients in this study were similar to those found in the Hong Kong Registry Report (15). The similarities suggested that little patient selection bias occurred in this study.
We found no difference in dialysis adequacy and residual glomerular filtration rate between the elderly and control groups. Elderly patients had a lower serum albumin level and nPCR than did patients in the control group. The higher prevalence of diabetes in the elderly group may explain the difference in nutrition status.
In the evaluation of clinical outcomes, the data are consistent with other published reports showing that elderly PD patients can have a reasonable survival rate (9,10,16). We found no significant differences between the elderly group and the control group in regard to the clinical outcomes of patient survival, technique survival, and peritonitis-free period.
The second focus of our study was to determine the effectiveness of self-care CAPD in elderly ESRD patients. We found no significant differences in clinical outcome between the self-care CAPD patients and the elderly assisted CAPD patients.
In preparation for dialysis, our team—which includes doctors, nurses, and medical social workers—assesses the clinical and socioeconomic background of every individual about to enter the program. Dietitians, occupational therapists, and physiotherapists also work to support these patients. Patients who have the ability to do CAPD exchanges by themselves are trained for self-care CAPD. Otherwise, arrangements are made for the patient to have assistance with CAPD at home or to be considered for institutional care when they become dependent on others for activities of daily living.
Although significantly more patients in the elderly group than in the control group required a helper for exchanges (p = 0.002), the elderly group still contained a very high percentage of self-care CAPD patients (82.64%). We observed no significant difference in clinical outcome between the elderly self-care CAPD patients and the elderly assisted CAPD patients. The median training period was 5 days for the elderly self-care CAPD group, a duration that is quite reasonable and similar to the training time required in our previously reported study of double-bag systems in the overall ESRD population (17).
Conclusions
Our results illustrate that most elderly ESRD patients 65 years of age and older have the ability to perform their own exchanges. Careful patient assessment, pre-dialysis education, and appropriate CAPD training methods for elderly patients are important in helping this population to have an independent life. Elderly patients are more likely to adhere to the treatment regimen, and they tend to have greater motivation for dialysis treatment (11). The CAPD modality is appropriate for these patients, and good technique and patient survival are observed whether exchanges are performed by the patients themselves or by a helper.
Nephrologists should no longer use age alone to determine whether to offer or withhold dialysis for elderly ESRD patients. The CAPD modality is a good option that can be offered to elderly patients. Respecting the needs and rights of elderly patients and maintaining their ability for self-care are other important aspects to consider when planning for long-term dialysis (18). Renal team members should be prepared for a slightly longer training time when providing CAPD to elderly ESRD patients.
The present study confirmed that CAPD is an effective dialysis modality for elderly ESRD patients. Self-care CAPD is possible in most cases, and assisted CAPD provides comparably good clinical outcome in terms of patient and technique survival and peritonitis-free period.
Footnotes
Acknowledgments
The present study was supported in part by the Chinese University of Hong Kong Research Grant Account 6900570. The authors thank the entire peritoneal dialysis team of Prince of Wales Hospital—doctors, nurses, medical social workers, dietitians, occupational therapists, and physiotherapists—for their care of the center's CAPD patients.