
Abstract
Conversely, PD clearance is almost insignificant in multivariate Cox regression models for all-cause mortality and cardiovascular death (1). That finding provided important evidence that the contributions of RRF and of PD clearance to the overall survival of PD patients are not equivalent. Indeed, a further re-analysis of data from the CANUSA study clearly showed that predictive power for mortality is attributable to RRF and not to PD dose (4).
Those results should not lead to the assumption that the dose of PD is unimportant; however, it does suggest a more important contribution of RRF than of PD clearance to the overall survival of PD patients. The present article provides evidence to support the importance of preserving RRF in PD patients and suggests potential mechanisms that explain the associations between RRF and overall and cardiovascular survival in PD patients (Figure 1).
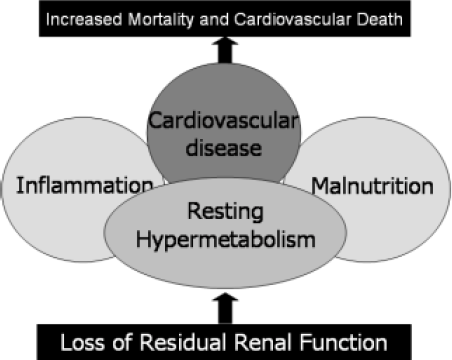
Mechanisms of associations between loss of residual renal function and mortality in peritoneal dialysis patients.
Residual Renal Function and Left Ventricular Hypertrophy
Left ventricular hypertrophy (LVH) is well recognized as an important predictor of mortality and cardiovascular death in PD patients, as confirmed in a previous survey, which showed that more than 90% of prevalent PD patients have LVH (1). Moreover, LVH was observed to have an important inverse relationship with RRF, in that anuric PD patients suffered the most severe degree of LVH, and no relationship was found between PD clearance and degree of LVH (5).
Several mechanisms may potentially explain the association between RRF and LVH, one of which is the role of RRF in maintaining fluid balance. The link between RRF and volume control is evidenced by the extracellular volume expansion found in PD patients with a lesser degree of RRF (6). Extracellular volume overload is increasingly recognized as a frequent complication in chronic PD patients that has important prognostic implications (7). Indeed, one study observed worse LVH and dilatation and worse systolic and diastolic function among PD patients who had a previous history of volume overload (8). Anuric PD patients have been noted to have worse blood pressure than patients with RRF, and that situation may again be partly attributable to poor volume control (9,10).
In the re-analysis of the CANUSA study data, every 250 mL of urine output was associated with a 36% reduction in overall mortality. In addition, the presence of urine output displaced renal small-solute clearance from the multivariate Cox regression model (4), providing indirect evidence that any degree of sodium and water removal by the diseased kidneys continues to have a major influence on the survival of PD patients.
Alternatively, the link between RRF loss and worsening of LVH may be partly explained by greater anemia with loss of erythropoietin production, greater hypoalbuminemia, and higher arterial pulse pressure (5,10), all of which are known risk factors for LVH in PD patients. The findings that RRF (but not PD small-solute clearance) was significantly associated with LVH independent of hypertension, anemia, and hypoalbuminemia (5) suggest that some non-dialyzable uremic toxins may play a role in mediating LVH in PD patients.
Residual Renal Function and Inflammation
Inflammation plays a pivotal role in the initiation and progression of atherosclerosis, and inflammation is considered a major nontraditional risk factor for accelerated atherosclerosis in dialysis patients (11,12). A previous study by my group showed that more than one third of prevalent Chinese PD patients had evidence of inflammation as denoted by a high-sensitivity C-reactive protein (CRP) serum level 5 mg/L or higher. In addition, CRP is an important predictor of mortality and cardiovascular death in PD patients (13).
The degree of inflammation is not only closely linked with atherosclerotic vascular disease, it is also associated with RRF, in that anuric PD patients show the greatest inflammatory response as measured either by CRP (13) or by soluble vascular cell adhesion molecule 1 (14). The exact mechanism underlying this latter association remains unclear. Loss of RRF (or uremia per se) has been suggested to possibly enhance an inflammatory response by increasing oxidative stress—a response that may lead to monocyte activation and cytokine production (15). The involvement of the kidneys in cytokine handling, as evidenced by impaired cytokine clearance in nephrectomized rats (16), has also been suggested as another possible mechanism that can explain the link between loss of RRF and inflammation.
On the other hand, inflammation has been closely linked with arterial stiffening, LVH and dilatation, and systolic dysfunction in PD patients (1). Importantly, loss of RRF, inflammation, and LVH are not only closely interrelated, they also combine adversely to increase the mortality and cardiovascular death risk in chronic PD patients (1). Similarly, circulating soluble vascular cell adhesion molecule 1 is also associated with RRF and LVH in PD patients.
In addition, the association between loss of RRF and increased mortality and cardiovascular event risk is partly mediated via the close associations of RRF with inflammation and endothelial activation (14). In PD patients, the combination of inflammation and endothelial activation confers a higher risk of mortality and of cardiovascular event occurrence than either factor does alone (14).
Residual Renal Function, Phosphorus Control, and Valvular Calcification
Cardiovascular calcification is increasingly recognized as a frequent and important complication in patients on dialysis. It is largely attributed to deranged mineral metabolism with resulting abnormal calcium–phosphorus control. A previous survey showed that, in at least 40% of chronic PD patients, serum phosphorus was elevated above 1.78 mmol/L (17), the target currently recommended by the Kidney Disease Outcomes Quality Initiative. More importantly, that study observed a strong inverse relationship between residual GFR and phosphorus control even when the average residual GFR of the PD patients fell below 2 mL/min/1.73 m2 (17). Among patients with well-preserved RRF, residual GFR was second to dietary protein intake as the most important determinant of phosphorus control. However, because PD clearance becomes the only means of phosphorus removal in anuric patients, and because such removal may be inadequate, the result is a greater prevalence of valvular calcification observed in the anuric PD population (unpublished data).
Another survey reported that at least one third of prevalent PD patients had heart valve calcification (18). Apart from the important association with CaxP product, heart valve calcification was demonstrated to be closely linked to inflammation and malnutrition in PD patients. Even among patients without an excessive CaxP product, the presence of inflammation and malnutrition was associated with an increased risk of valvular calcification (18), providing further evidence to support the involvement of inflammation in valvular calcification. Indeed, evidence is accumulating that, rather than being passive, degenerative processes, vascular and valvular calcification are dynamic and active cell-mediated processes that involve a switch in the phenotype of vascular smooth muscle cells to osteoblast-like cells.
A recent study showed that serum fetuin-A, a circulating calcification inhibitory protein and a negative acute-phase reactant, is inversely associated with valvular calcification independent of CRP and a high CaxP product. Furthermore, serum fetuin-A is predictive of mortality and cardiovascular death in PD patients. However, no association was observed between RRF and serum fetuin-A (19), suggesting that increased valvular calcification in anuric PD patients is unlikely to be mediated by depletion of circulating fetuin-A.
Valvular calcification was recently identified as an important predictor of mortality and cardiovascular death in PD patients (20). Notably, PD patients exhibiting both valvular calcification and atherosclerotic vascular disease (as compared with patients having either or neither of these complications) had the highest mortality and cardiovascular death. Furthermore, for patients with either valvular calcification or atherosclerotic vascular disease, overall survival and cardiovascular event-free survival were comparable (20). Those results, together with recent findings of an association between heart valve calcification and carotid atherosclerosis (21), provide important evidence that valvular calcification represents a marker of atherosclerosis as well as a reflection of poor calcium and phosphorus control in PD patients.
Residual Renal Function and Nutrition
Residual renal function makes an important contribution to the overall nutrition status of PD patients— whether assessed using serum albumin, subjective global assessment, or handgrip strength (22-24). A previous study showed that handgrip strength, a reliable marker of lean body mass, was strongly predictive of survival and cardiovascular outcome in PD patients, independent of inflammation and RRF (24).
Using a locally validated food frequency questionnaire, an important association was demonstrated between total weekly urea clearance and dietary protein and energy intake in PD patients (23). Intake of micro-nutrients, including vitamin A and most water-soluble vitamins (B1, B2, B6, B12, folic acid, niacin, and C), plus minerals including calcium, phosphorus, iron, and zinc, was also associated with total weekly urea clearance (25). More importantly, the associations of total weekly urea clearance with dietary macronutrient and micro-nutrient intake were largely attributable to RRF and not to PD urea clearance (23,25).
Peritoneal urea clearance, when considered as a separate factor, showed no relationship with any of the nutritional indices, including subjective global assessment, handgrip strength, or dietary macronutrient or micronutrient intake (23-25). That finding provides important evidence that the contributions of RRF and PD clearance to the overall nutrition status of PD patients are indeed not equivalent and not simply additive. Whether this indicates a differential capacity of PD and RRF to remove middle-molecule uremic toxins remains to be determined.
Loss of RRF may also contribute to malnutrition in PD patients through its close relationship with increased resting energy expenditure (26). Resting energy expenditure accounts for 60%–80% of total energy expenditure. A sustained increase may lead to an energy imbalance and malnutrition if not compensated for by an increase in energy intake. Previous work by my group showed that resting energy expenditure not only increases in patients with malnutrition–inflammation–atherosclerosis syndrome, but more importantly, shows a strong inverse relationship with RRF in PD patients. No association was observed between resting energy expenditure and PD clearance. In addition, resting hypermetabolism mediated increased mortality and cardiovascular death in PD patients partly through its close association with RRF (26).
Conclusions
Previous work has clearly demonstrated that residual renal clearance and PD clearance cannot be assumed to be equivalent in PD patients. Apart from providing small-solute clearance, RRF continues to serve important metabolic and hemodynamic functions and plays a crucial role in maintaining cardiovascular health, nutrition status, and wellbeing (10,27). It also contributes significantly to the overall survival of PD patients. These data suggest that the important goal of preserving RRF should continue even after ESRD patients are started on long-term PD. More effective therapeutic strategies are needed to preserve RRF in PD patients.
Footnotes
Acknowledgment
The work described here is supported by funds from the Hong Kong Health Service Research Grant Number 6901023, Hong Kong Society of Nephrology Research Grants and the Baxter Extramural Grant Program, of which Angela Yee-Moon Wang is the principal investigator.