
Abstract
Tuberculous Peritonitis
Patients with chronic kidney disease are immunocompromised and more prone to developing opportunistic infections, including tuberculosis (2). A high prevalence of tuberculous infection has been reported in patients undergoing CAPD, especially in areas of the world where tuberculosis is endemic (3-7). In contrast to the general population, dialysis patients more commonly experience extra-pulmonary tuberculosis (8). Tuberculous peritonitis is the second most common form of tubercular infection in CAPD patients, accounting for 30% – 40% of cases (4,5).
Diagnosis
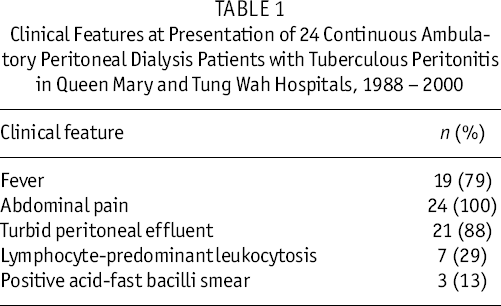
The initial clinical presentation of tuberculous peritonitis in CAPD patients is often indistinguishable from that of bacterial peritonitis. Table 1 summarizes the clinical features of 24 cases of CAPD-related tuberculous peritonitis presented in our hospitals over a period of 12 years.
Most of the patients presented with abdominal pain, cloudy peritoneal dialysate, and fever. Lymphocyte-predominant leukocytosis in the ascitic fluid, which is a typical feature of tuberculous peritonitis in the general population, was present in the dialysate of only about 30% of our CAPD patients with tuberculous peritonitis. Dialysate smears from most of the patients were negative for acid-fast bacilli.
Definitive diagnosis of tuberculous peritonitis relies on positive growth of Mycobacterium tuberculosis from the peritoneal dialysate. Early diagnosis of tuberculous peritonitis is often difficult because the clinical features are nonspecific, acid-fast bacilli are seldom seen on direct smear of the dialysate, and the culture process for acid-fast bacilli often takes 4 – 6 weeks to complete. Rapid diagnosis of tuberculous peritonitis in CAPD patients using gene amplification for M. tuberculosis DNA complex by polymerase chain reaction has been reported (9); however, the sensitivity and specificity of this test in the dialysate of CAPD patients remains to be established. Some authors have advocated the use of laparoscopic peritoneal biopsy for the rapid diagnosis of tuberculous peritonitis in CAPD patients (10), but that approach is relatively invasive and requires temporary interruption of CAPD. The tuberculin skin test is also of limited value because a high proportion of dialysis patients are anergic to tuberculin because of impaired cellular immunity (11).
Clinical Features at Presentation of 24 Continuous Ambulatory Peritoneal Dialysis Patients with Tuberculous Peritonitis in Queen Mary and Tung Wah Hospitals, 1988 – 2000
Another means to achieve early diagnosis of tuberculous peritonitis in CAPD patients is a therapeutic trial of antituberculosis drugs. We maintain a high index of suspicion for tuberculous peritonitis in our CAPD patients. A therapeutic trial of antituberculosis drugs is considered in patients with culture-negative peritonitis who have shown a partial response to intraperitoneal antibiotics (especially regimes containing aminoglycosides) and whose dialysate shows lymphocyte-predominant leukocytosis (either at initial presentation or evolved during the course of the peritonitis). Obviously, the threshold for initiating a therapeutic trial of antituberculosis drugs depends on the local prevalence of tuberculosis.
Treatment
No consensus has yet developed on the optimal drug regimen and duration of treatment for tuberculous peritonitis in CAPD patients. Our usual treatment regimen consists of isoniazid (200 – 300 mg daily), rifampicin (450 – 600 mg daily), and levofloxacin (200 mg daily) for 12 months, with pyrazinamide (1.5 – 2 g daily) for the first 3 months (3,4). Streptomycin is not used because of its potential ototoxicity and adverse effect on residual renal function. Ethambutol is also not included in our treatment regimen because of its enhanced ocular toxicity in renal failure patients (12). Nevertheless, for patients who fail to respond adequately to the usual first-line antituberculosis drugs, ethambutol can still be used with careful monitoring for ocular toxicity. Pyridoxine at 100 mg daily is routinely given to prevent isoniazid-induced neurotoxicity (13). Our treatment regimen has, in general, been well tolerated by patients. No recurrence of tuberculous peritonitis has been observed in patients who completed 12 months of antituberculosis therapy.
In the past, removal of the peritoneal dialysis catheter was recommended in all patients with tuberculous peritonitis (14). Recent studies indicate that primary removal of the peritoneal dialysis catheter is not mandatory and that long-term continuation of CAPD is possible after tuberculous peritonitis (4,5,15). This treatment strategy is particularly relevant in places where most of the patients are on CAPD and the availability of temporary hemodialysis support is limited. Continuation of CAPD in patients with tuberculous peritonitis also allows the response to antituberculosis treatment to be monitored by serial measurement of white cell count in the peritoneal dialysate.
The mortality rate before completion of treatment of our CAPD patients with tuberculous peritonitis has been about 30%. Most of the deaths were not directly related to the underlying tuberculous peritonitis. Among patients who completed antituberculosis treatment, about 75% were successfully maintained on CAPD.
Summary
Tuberculous peritonitis is an uncommon complication of CAPD. A high index of suspicion is needed for early diagnosis. Treatment with standard antituberculosis drugs for an extended period of 12 months appears to be effective. Removal of the peritoneal dialysis catheter is not mandatory, and long-term continuation of CAPD after tuberculous peritonitis is possible.
Fungal Peritonitis
Fungal peritonitis is an uncommon but serious complication of peritoneal dialysis. It is associated with significant morbidity and mortality (16). The incidence of fungal peritonitis in patients undergoing CAPD ranges from 3% to 7% in most reported series (17-22). Candida species (mainly C. parapsilosis, C. albicans, and C. tropicalis) are the most common causative agents of CAPD-related fungal peritonitis, accounting for 70% – 80% of all cases (17-22). A variety of other fungi such as Trichosporon, Penicillium, Aspergillus, and Acremonium species make up the remaining 20% – 30% of cases.
Diagnosis
The most important predisposing factor for the development of fungal peritonitis in CAPD patients is prior exposure to antibiotic therapy, especially for the treatment of bacterial peritonitis. The reported incidence of prior antibiotic exposure in CAPD patients with fungal peritonitis ranges from 34% to 80% (17-22). It has been postulated that broad-spectrum antibiotics suppress the normal intestinal flora, leading to an overgrowth of intestinal fungi, which migrate across the intestinal wall to reach the peritoneal cavity and cause fungal peritonitis.
Notably, though, a substantial proportion of fungal peritonitis occurs without recent exposure to antibiotics. The causes of these de novo cases of fungal peritonitis vary and may include direct contamination of the dialysis catheter during the exchange procedure, underlying intestinal pathology such as diverticulosis in the host (17), and environmental contamination (23).
Treatment
The peritoneal dialysis catheter should be removed as soon as possible after a diagnosis of fungal peritonitis is made. Recent reports have shown that leaving the catheter in situ is associated with higher rates of mortality and technique failure (19,21). The suggestion is that fungal peritonitis results in formation of a biofilm around the dialysis catheter, rendering the eradication of the fungal infection difficult without removal of the catheter (24). Isolated cases of successful continuation of CAPD without catheter removal have been reported with the use of various regimens of intraperitoneal antifungal agents (25); however, the overall success rate of this approach is low, and many patients still eventually require catheter removal. Treatment of fungal peritonitis without catheter removal is probably justifiable only in patients who are very old and frail and hence unlikely to be able to tolerate temporary hemodialysis.
The conventional empirical treatment for fungal peritonitis was a combination of intravenous amphotericin B and flucytosine or oral fluconazole and flucytosine (26), but recent studies have suggested that, for fungal peritonitis caused by Candida species, oral fluconazole alone, 200 mg daily, is as effective as the conventional combination therapy (19,22). Patients who fail to respond to oral fluconazole can be treated with intravenous amphotericin B (30 mg daily for 21 days). Anti-fungal treatment should continue for 3 – 4 weeks after catheter removal. For fungal peritonitis caused by non-Candida species, the choice of antifungal agents needs to be individualized, taking into account the fungal species isolated and their pattern of sensitivity to antifungal agents. The roles of newer antifungal agents such as caspofungin and voriconazole in the treatment of CAPD-related fungal peritonitis remain to be determined.
Fungal peritonitis in CAPD patients is associated with high rates of mortality and technique failure. The mortality rate in CAPD-related fungal peritonitis ranges from 5% to 40% (17-22). Many patients are unable to resume CAPD after fungal peritonitis because of peritoneal fibrosis (17-22).
Antifungal Prophylaxis
Given that recent antibiotic exposure is a recognized risk factor for fungal peritonitis in CAPD patients, administration of antifungal prophylaxis with every antibiotic prescription may help to reduce the occurrence of fungal peritonitis. Lo et al. (27) showed that 4-times-daily oral nystatin 500,000 U with every antibiotic prescription significantly reduced both the overall incidence and the antibiotic-related Candida incidence of peritonitis in CAPD patients; however, two subsequent studies failed to confirm a benefit for nystatin prophylaxis (28,29). It appears that, although antifungal prophylaxis is desirable in CAPD patients, the optimal prophylactic strategy remains to be established.
Summary
Fungal peritonitis is a serious complication of CAPD. Early removal of the peritoneal dialysis catheter is recommended in all patients. Peritonitis caused by Candida species can be treated with oral fluconazole. The treatment for peritonitis caused by non-Candida species needs to be individualized. The role of antifungal prophylaxis remains to be clarified.