
Abstract
Objective
To describe our experience with hernioplasty in peritoneal dialysis patients and to identify possible risk factors for surgical complications.
Design
A 4-year retrospective chart review of data.
Setting
Peritoneal dialysis unit of a university hospital.
Patients and Methods
58 hernias in 50 patients were included. Detailed surgical technique and complications were recorded. Possible risk factors included age, gender, weight, height, body mass index, previous surgery, diabetes, time on dialysis, emergency surgery, hospital stay, type of hernia, mesh use, blood hemoglobin, and serum urea, creatinine, and potassium.
Results
Complications occurred in 12 hernioplasties (4 wound infections, 2 peritonitis, 4 catheter dysfunction, and 5 re-operations). Recurrence rate was 12% without mesh use and 0% with mesh hernioplasty. Dialysis was re-instituted in 96% of cases within 3 days postoperatively. Identified risk factors for complications were diabetes, low weight, low height, small body mass index, and low serum creatinine.
Conclusions
Mesh hernioplasty in peritoneal dialysis patients is advisable. Postoperative dialysis with low volume is feasible after surgery. Prospective studies will corroborate our risk factors for morbidity.
Keywords
The reported prevalence of hernia in PD patients ranges from 9% to 32% in most series (3-10), with an incidence of 0.06 hernias per dialysis-year at risk (4). Based on the hernia's location (umbilical, inguinal, and/or incisional), the hernia sac may gradually enlarge, exacerbating hernia symptoms and signifying morbidity. Therefore, rapid repair is warranted because of patient discomfort due to fluid accumulation in the patient's hernia sac and tissues, erratic fluid resorption, and conventional hernia complications such as recurrence, which can be as high as 27% (5,11).
There is controversy as to whether PD treatment can be safely continued after hernioplasty or should be held for a period of days to weeks post-operation in order to avoid stress in the repair (10,12-14). Tension-free hernia repair with polypropylene mesh reinforcement allows the patient to commence or continue PD as early as 24 hours after surgery (13,15-18), thus avoiding the need for a change in dialysis modality and offering advantages both to patients and to hard-pressed hemodialysis programs.
Abdominal wall hernia repair is a procedure with low morbidity and mortality in healthy individuals (19). Estimated morbidity rates for cardiac and general surgery in patients with end-stage renal disease range from 14% to 64%, secondary to fluid and sodium retention, volume overload, hyperkalemia, hemodynamic instability, bleeding, anemia, and infection (20). The aim of our study was to describe our experience with abdominal wall hernia repair in PD patients in order to assess the safety and effectiveness of our approach and to identify potential risk factors for morbidity in patients undergoing hernioplasty.
Material and Methods
Patients
We retrospectively reviewed charts from end-stage renal disease patients on continuous ambulatory PD (CAPD) who underwent abdominal wall hernioplasty from May 2003 to February 2007. All patients underwent surgery within a month after hernia diagnosis was established. All operations were performed under regional anesthesia. Cefotaxime (1 g, intravenous, single dose) was given to all patients preoperatively. Hernias were classified preoperatively as umbilical, incisional, or inguinal based on anatomical location. Inguinal hernias were also classified intra-operatively according to the Gilbert/Rutkow–Robbins system (21,22).
Follow-Up and PD Initiation and/or Restoration
Patients were followed up at 7 days, 30 days, and every 6 months after hospital discharge by clinic appointment, with history and physical examination. Treatment with PD was started the same day as the surgery in patients that had acute dialysis indication (hyperkalemia and/or uremic syndrome) and in patients in whom hernia orifice size was considered small (<2 cm). Treatment with PD was paused for the day of surgery in patients with preexisting PD catheter with medium and large size hernia defect. Over the next days, when PD was reinitiated, low volume (1.0 – 1.5 L), 1.5% dextrose, high frequency exchanges (6 exchanges per day) were ordered by the attending nephrologists. All the patients’ original PD regimens were gradually reinstated over the next 2 weeks after PD was initiated during the postoperative period, unless they required temporary hemodialysis or the PD catheter could not be utilized.
Surgical Procedure
A different approach was used for each type of hernia. Special care was taken in order to avoid opening the peritoneum. For small umbilical hernias (<2 cm), a curved infraumbilical incision was used, preserving the umbilicus. When possible, a straight tissue re-approximation or “vest over pants” repair was performed. Larger umbilical hernias were approached through midline incision and most were treated as incisional hernias.
An open anterior tension-free onlay patch technique previously published by the authors was used for inguinal hernia repair (23). Briefly, identification and management of the inguinal hernia sac is done properly and the posterior wall of the inguinal canal (transversalis fascia) is incised, identifying and clearing Cooper's ligament. A pre-cut standard polypropylene mesh, designed and patented by one of the authors (H.E.R.D.) is used. The medial end and lower edge of the mesh are configured to match the medial corner of the inguinal canal, the posterior wall, and the femoral area, creating a triangular extension with rounded borders (Figure 1). The mesh is sutured and anchored to the pubic tubercle, Cooper's ligament, inguinal ligament, and internal oblique aponeurosis and muscle (23).
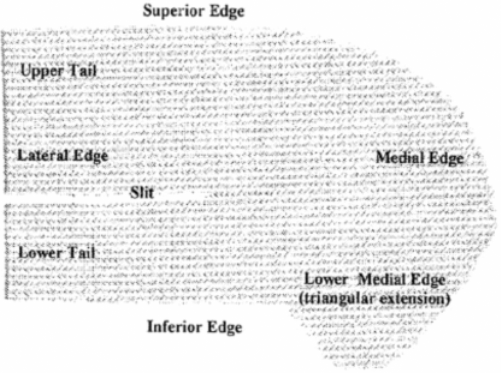
Precut polypropylene sheet of mesh used in the herniorrhaphy; 2–0 polypropylene is used to suture the mesh.
For incisional hernias, an extraperitoneal approach was used unless indicated by hernia sac incarceration or strangulation. The hernia orifice was clearly demarcated and dissected 2 cm away from it. If opened, the peritoneum is closed. A supra-aponeurotic onlay polypropylene mesh, anchored 1.5 – 2 cm outside the hernia orifice with 2–0 polypropylene, was used with or without tissue re-approximation with size 1 polyglycolic acid sutures. If extensive dead space was created, a closed suction drain was left in place until no further drainage resulted.
Surgical complications were defined as infection (wound and/or peritonitis), bleeding, dialysis fluid leakage, PD catheter dysfunction within 30 days after surgery, re-operation for any of the previous, and hernia recurrence. The following variables were studied as possible risk factors for surgical complications: age, gender, weight, height, body mass index, previous abdominal surgery, diabetes mellitus, time on PD, elective or emergency surgery, length of hospital stay, type of hernia, polypropylene mesh use, blood hemoglobin, and serum urea, creatinine, potassium, and albumin.
Statistical Analysis
Simple descriptive analysis of the data was undertaken. Proportions were reported for categorical variables; mean (standard deviation) and median were used to describe normally and non-normally distributed continuous variables respectively. The unpaired Student's t-test and Mann–Whitney U tests were used to assess differences between continuous variables with normal and non-normal distribution respectively. Categorical variables were analyzed by chi-square test to identify those related to the development of surgical complications. Multivariate regression analysis was performed on those variables identified in the bivariate analysis as statistically significant for surgical complications. A probability value of p < 0.05 was considered statistically significant. Data were analyzed using SPSS 11.0 software (SPSS, Chicago, Illinois, USA).
Results
A total of 58 hernia repairs were performed in 50 patients. Patients’ demographic data and hernia classifications are summarized in Table 1. Umbilical and incisional hernias were the most common type of hernia. Type IV hernia according to the Gilbert/Rutkow– Robbins system was the most common type of inguinal hernia. Most (72%) patients (n = 36) had had at least one previous abdominal surgery. The most common type of surgical abdominal procedure was a previous PD catheter placement, followed by cesarean section and previous hernioplasty (data not shown). Seventeen of 58 (29.3%) hernias were repaired at the time of PD catheter placement. Fourteen (28%) patients underwent a PD catheter replacement before hernioplasty. Mean time on PD before hernioplasty was 14.1 ± 17.03 (range 0 – 86) months. Preoperative kidney disease data are shown in Table 2.
Patients’ Demographic Data and Hernia Classifications
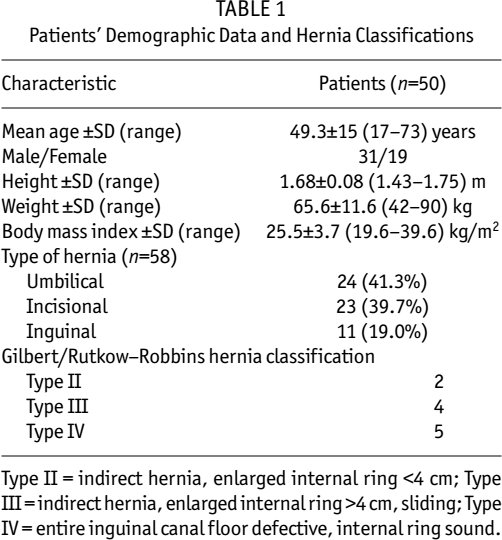
Type II = indirect hernia, enlarged internal ring <4 cm; Type
III = indirect hernia, enlarged internal ring >4 cm, sliding; Type
IV = entire inguinal canal floor defective, internal ring sound.
Preoperative Herniorrhaphy Kidney Disease Parameters
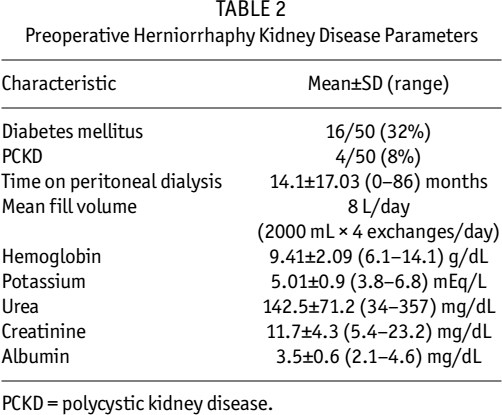
PCKD = polycystic kidney disease.
Most hernias (51/58; 87.9%) were repaired as elective procedures. Mean hernia orifice was 3.1 ± 2.02 (1 – 10) cm Mean surgical time was 73 ± 43 (25 – 300) minutes. Mesh hernioplasty was performed in 29 procedures, which included all inguinal hernias. Postoperative length of stay in hospital was 3.4 ± 3.9 (1 – 30) days. Peritoneal dialysis was initiated the same day as surgery in 22 hernioplasties, based on small hernia orifice size and/or acute dialysis indication (37.9%), including all patients that had their hernia repair at the time of PD catheter placement (n = 17). Peritoneal dialysis was reestablished within 72 hours after surgery in 34 hernia repairs (58.6%) and 1 patient was withheld from PD for 6 days. Hemodialysis was planned preoperatively and utilized in 1 patient for 120 days after surgery and PD was resumed afterwards.
Twelve of 58 (20.6%) hernioplasties suffered surgical complications; 6 hernioplasties experienced more than 1 postoperative complication, for a total 18 episodes of morbidity. Surgical complications are depicted in Table 3. There was no dialysis fluid leakage in any hernia repair. Five patients underwent reoperation (3 for PD catheter dysfunction, 1 for postoperative bleeding/PD catheter dysfunction, and 1 for wound infection debridement). There were three hernia recurrences, all in patients that did not undergo mesh hernioplasty. Recurrences were noted 12, 17, and 21 months after surgery. Recurrence rate in patients without the use of mesh was 12%. No patients that underwent mesh hernioplasty have evidenced recurrence.
Selected Published Studies of Abdominal Wall Hernia Repair in Peritoneal Dialysis Patients
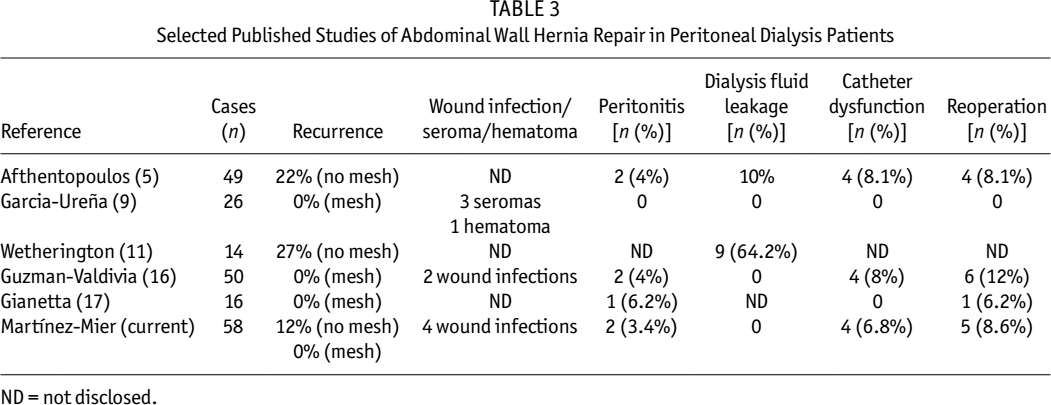
ND = not disclosed.
Three of 50 (6%) patients were lost to follow-up. The rest have been followed up from 2 to 45 months: 40 patients (80%) remain on PD, 4 (8%) patients were transferred to hemodialysis, 2 patients (4%) died from underlying disease, and 1 (2%) patient underwent kidney transplantation. Hernia recurrence has been diagnosed only in patients still on PD.
In the bivariate analysis, only the following risk factors for surgical complications were statistically significant: diabetes mellitus (p < 0.02), low height (p < 0.003), low weight (p < 0.03), low body mass index (p < 0.03), and low creatinine level (p < 0.03). In multivariate regression analysis, diabetes mellitus (p < 0.02) and low body mass index (p < 0.04) remained statistically significant for surgical complications in a model in which all the previous variables were included.
Discussion
The present study demonstrated that hernioplasty in PD patients has low morbidity and no recurrence rate when a tension-free mesh hernioplasty is performed, although there are certain risk factors for surgical complications, such as prior history of diabetes mellitus, low height, low weight, low body mass index, and low serum creatinine. Furthermore, this study supports the idea that early restoration of PD with low exchange volume after hernioplasty is feasible, avoiding temporary hemodialysis.
Recurrence rate after hernioplasty in PD patients is variable and depends on the hernia repair technique. Initial studies by Afthentopoulos et al. (5) and Wetherington et al. (11) without the use of mesh showed a recurrence rate of 22% and 27% respectively. The use of tension-free techniques is one of the most important breakthroughs in the treatment of abdominal wall hernias and has been used in patients on PD (9,13,16-18). Lewis et al. (15) first advocated the use of polypropylene mesh in this particular population. Garcia-Ureña et al. (9) observed no recurrence in a prospective series of 26 hernias. Recently, Crabtree (24) used a low-tension buttressed hernioplasty with onlay mesh to repair umbilical hernias in 34 PD patients; 13 of those repairs were performed after commencing dialysis therapy (24). Most of these studies did not diagnose hernia recurrence during follow-up, which suggests that all hernia repairs in PD patients should be performed using mesh hernioplasty.
Our study is probably one of the largest series published (58 hernias in 50 patients). We found that umbilical hernia was the most common type of hernia, similarly to others (5,9,11). Likewise, time on PD prior to hernioplasty was close to 12 months, as previously published (5,9,10,13). Mesh was used to repair 50% of hernias. The choice of mesh use was based mostly on hernia orifice size (<2 cm). We did not experience hernia recurrence in patients that underwent mesh hernioplasty, regardless of hernia type or hernia orifice size. Although we had a 12% recurrence rate without mesh use, it was less than in similar previously published series (5,11). Given the differences in our recurrence rate when mesh hernioplasty was performed, we advocate mesh hernioplasty in order to decrease the recurrence rate, as others have suggested (9,13,15-18).
End-stage renal disease patients might have small anthropometric measurements (low height and weight and small body mass index), and even low creatinine levels secondary to muscle wasting and chronic malnutrition (25). In addition, some of them are diagnosed with diabetes mellitus. These comorbid conditions contribute to a higher incidence of surgical complications in this population (2,3,8,20,26,27). Our results are in accordance with these previous studies since we identified low height and weight, small body mass index, diabetes mellitus, and low creatinine levels as risk factors for surgical complications. Of note, the use of mesh did not correlate with surgical complications such as wound infections or peritonitis, in the same way as Afthentopoulos et al. (5) and Garcia-Ureña et al. (9) described. In our center, we administered antibiotic prophylaxis (cefotaxime 1 g intravenous, preoperative, single dose) per routine in all our PD patients in order to decrease the incidence of infections.
To guarantee proper healing and to avoid postoperative dialysate leakage or early hernia recurrence, PD treatment is commonly withheld for several days or even weeks, often prolonging hospital stay and becoming a serious threat of infection to the patients. Cherney et al. (10) reported a 45.4% incidence of temporary hemodialysis in PD patients with incarcerated abdominal wall hernias. Tension-free hernioplasty with polypropylene mesh seems to allow continuation of PD early after surgery, with no dialysate leak or other complications (13,14-18). Mettang et al. (13) utilized low-volume high-frequency exchanges within 1 – 3 days after surgery. No complications were noted in their study. Lewis et al. (15) restarted PD within 24 hours in 100% of postoperative recoveries, as did Guzman-Valdivia et al. (16). Shah et al. (27) recommended continuation on standard PD therapy until the morning of the surgery, followed by no dialysis for the first 48 hours and intermittent PD 3 times per week (1-L exchange for 10 hours) for 2 weeks for CAPD patients, low volume CAPD for another 2 weeks, and resumption of the preoperative PD prescription after 4 – 5 weeks, with excellent results (27). Another PD management protocol has been suggested by Crabtree (24) in which low-volume automated PD exchanges are used, with an initial fill volume of 1 L, which is gradually increased to 1.5 L the second week, and with resumption of usual dialysis regimen thereafter. Our results agree with the previously reported results in the literature. We found that PD was successfully initiated within 72 hours after surgery in 96.5% of the surgical procedures, prescribing a low-volume high-frequency exchange program over 2 weeks, regardless of the type of hernia repair (conventional and/or tension free). Finally, automated PD might be utilized as an alternative in the postoperative period, since low volume and short time of inflow and outflow could be regulated in the cyclers (1,24); however, automated PD is not always available in all centers, such as our institution (approximately 20% of all of our PD population).
In conclusion, we advocate the use of tension-free mesh hernioplasty in patients on PD in order to decrease the incidence of hernia recurrence. Continuation of PD with initially low, stepwise increased volume and frequent exchanges is a feasible possibility in patients undergoing hernioplasty. There are possible perioperative risk factors for surgical complications in PD patients undergoing hernia repair. Further prospective studies will elucidate and corroborate these findings.