
Abstract
Background
An early and reliable diagnostic procedure for acute peritonitis in patients on peritoneal dialysis (PD) without typical clinical symptoms remains an important challenge in modern nephrology. During the first days of peritonitis, establishing the diagnosis based on peritoneal effluent pleocytosis and inflammatory markers [C-reactive protein (CRP) or interleukin-6] is not efficient in all cases. Increased peritoneal membrane permeability is a well-known consequence of peritonitis. Therefore, we evaluated the concentrations of selected circulating adipose tissue-derived proteins in the peritoneal effluent of PD patients with episodes of acute peritonitis.
Material and Methods
Concentrations of adiponectin and leptin, in both plasma and peritoneal effluent, were assessed in 24 adult PD patients with peritonitis episodes confirmed by clinical symptoms and/or microbiological tests, and in 23 PD patients without signs and symptoms of inflammation (control group).
Results
In peritoneal effluent collected from patients with acute peritonitis (also without pleocytosis or increased CRP), both adiponectin and leptin concentrations were markedly elevated: adiponectin 744.1 (344.2 – 1144.1) ng/mL vs 4.8 (3.1 – 6.5) ng/mL; leptin 16.3 (9.4 – 23.1) ng/mL vs 5.1 (0.5 – 9.6) ng/mL. Receiver operating characteristic analyses revealed that peritoneal effluent adiponectin concentration >180 ng/mL has 100% sensitivity and 100% specificity, while peritoneal effluent leptin concentration >11.0 ng/mL has 58.3% sensitivity and 95.5% specificity for the diagnosis of acute peritonitis. The increases in adiponectin and leptin concentrations in peritoneal effluent were not consequences of changes in their plasma levels. A positive correlation between peritoneal effluent and plasma concentrations of adiponectin and leptin in patients with peritonitis was found.
Conclusion
Increased concentration of leptin and especially adiponectin in peritoneal effluent seems to be a valuable and new early marker of high peritoneal membrane permeability due to acute peritonitis.
The aim of the present study was to assess concentrations of adipokines (adiponectin and leptin) produced by adipose tissue in peritoneal effluent of patients suspected of having acute peritonitis during PD therapy.
Patients and Methods
This study was performed in 24 patients with chronic kidney disease treated with PD (mean age 62 ± 13 years, mean time on PD 21 ± 15 months) and with acute peritonitis confirmed by clinical symptoms and microbiological tests. The control group consisted of 23 PD patients (mean age 54 ± 16 years, mean time on PD 16 ± 13 months) without signs and symptoms of inflammation. Cause of chronic renal disease was as follows: diabetes mellitus (22 patients), chronic pyelonephritis (6 patients), glomerular disease (6 patients), hypertensive nephropathy (3 patients), polycystic kidney disease (3 patients), amyloidosis (3 patients), and unknown (4 patients).
Based on the results of routine peritoneal equilibration tests performed in these patients, their transport status was as follows: high transporters 14.3%, high average 42.9%, low average 42.9%, low transporters zero. Mean dialysate-to-plasma ratio (D/P) of urea was 0.93 (0.9 – 0.95), mean D/P creatinine was 0.68 (0.62 – 0.75), mean Kt/V was 2.36 (2.0 – 2.71). All patients used glucose-based dialysate fluid and the Baxter twin-bag system (Baxter Healthcare, Deerfield, Illinois, USA) or the Fresenius stay · safe system (Fresenius Medical Care, Bad Homburg, Germany). Dwell times were generally 4 – 5 hours during the day and 8 – 9 hours overnight. All diabetic patients were treated with subcutaneous insulin. Clinical and biochemical data of both groups are shown in Table 1.
Clinical and Biochemical Characteristics of Peritoneal Dialysis (PD) Patients with Acute Peritonitis and in PD Patients Without Signs and Symptoms of Peritonitis (Control Group)
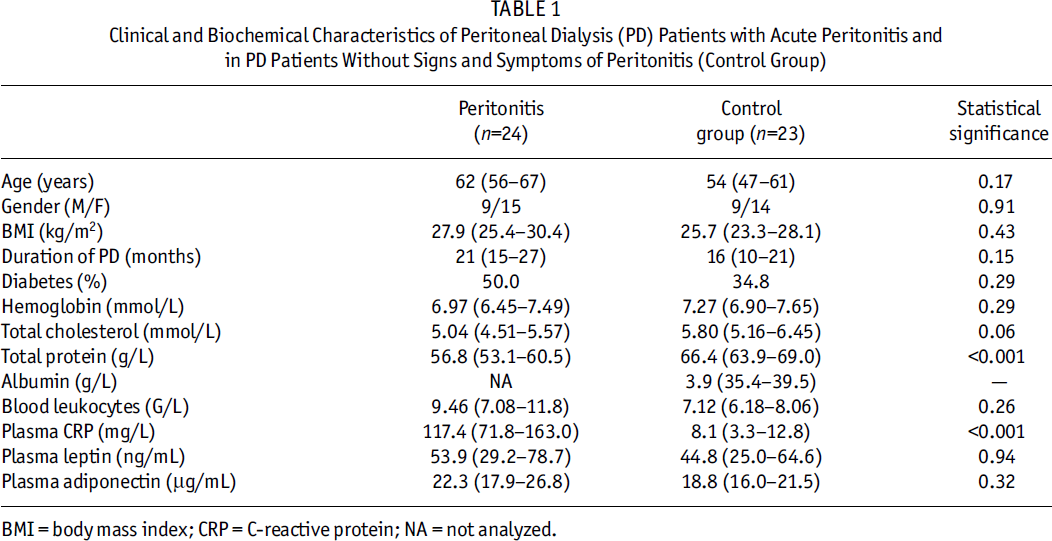
BMI = body mass index; CRP = C-reactive protein; NA = not analyzed.
In all patients with suspected peritonitis, concentrations of adiponectin, leptin, and CRP in plasma and in peritoneal effluent were assessed twice: the first at admission to the hospital due to the suspicion of acute peritonitis, and the second after recovery, 1 day before the patient was discharged from the hospital [mean time from the diagnosis to recovery was 14 days (12 – 16 days)]. In patients, the diagnosis of peritonitis was not yet established at the moment of admission; however, it was confirmed during the consecutive days. In the control group, all parameters were examined once. Plasma adiponectin concentration was measured by enzyme-linked immunosorbent assay (ELISA; B-Bridge, St. Jose, California, USA). Concentration of adiponectin in peritoneal effluent was measured with a 1000-fold lower dilution than standard plasma samples. Plasma leptin concentration was measured using radioimmunometric assay (Linco Research, St. Louis, Missouri, USA) and CRP was measured by turbidimetric method using a Beckman automated nephelometer (Beckman, Fullerton, California, USA).
Peritoneal clearances for both leptin and adiponectin were calculated based on plasma (P) and peritoneal effluent (D) concentrations, drained volume (V), and dwell time (t) according to the equation [D (/mL) x V (mL)] / [t (min) x P (/mL)].
Statistical analyses were performed using Statistica 6.0 (StatSoft Polska, Cracow, Poland) for Windows operating system (Microsoft Corp., Redmond, Washington, USA). Values are presented as mean and 95% confidence interval. Results were considered significant only with a p value less than 0.05. Statistical significance between compared groups was estimated using nonparametric tests (chi-square and Mann–Whitney U test). For analysis of changes in time, the Wilcoxon test was applied. To discriminate a cutoff value for the concentration of adipokines in peritoneal effluent characteristic for peritonitis, receiver operating characteristic curve analysis was performed.
Results
In patients admitted to our Peritoneal Dialysis Outpatient Department with the suspicion of peritonitis, peritoneal effluent pleocytosis examination was performed using the first and second effluent bags; however, in 25% of patients we were not able to confirm peritonitis based on pleocytosis alone.
Analysis of microbiological tests of peritoneal effluent in patients with peritonitis revealed that the most common pathogen was Staphylococcus epidermidis (in 7 patients). Serratia marcescens, Klebsiella pneumoniae, Staphylococcus hominis, and Escherichia coli were each identified in 2 patients, and there was 1 peritonitis episode each for Corynebacterium sp, Candida kefyr, Staphylococcus haemolyticus, Edwardsiella ictaluri, Ewingella americana, Acinetobacter lwoffii, and Candida glabrata involved. In 2 other cases, microbiological tests were negative.
At the time of diagnosis of a peritonitis episode, mean serum CRP level was markedly elevated (Table 1). In only 1 patient the CRP value was within the normal range (<5.0 mg/L); however, in 3 others, CRP level was only slightly elevated (range 5 – 10 mg/L). At discharge from the hospital, serum CRP concentration was significantly lower but still markedly above the normal range [50.0 (12.9 – 87.1) mg/L]. Also, peritoneal effluent concentration of CRP decreased significantly during the clinical course of peritonitis [2.29 (0.92 – 3.66) mg/L vs 0.78 (0.18 – 1.37) mg/L,p < 0.002]. In patients from the control group, mean concentration of CRP in peritoneal effluent was 0.2 (0.1 – 0.29) mg/L.
In peritoneal effluent collected from patients with peritonitis, both adiponectin and leptin levels were markedly elevated compared to the control group: adiponectin 744.1 (344.2 – 1144.1) ng/mL vs 4.8 (3.1 – 6.5) ng/mL, p < 0.001; leptin 16.3 (9.4 – 23.1) ng/mL vs 5.1 (0.5 – 9.6) ng/mL, p < 0.001 (Figure 1). The total amounts of adiponectin [1298 (586 – 2010) ng vs 11.6 (7.3 – 15.8) ng,p < 0.001] and leptin [28.6 (16.3 – 40.8) ng vs 12.1 (1.2 – 22.9) ng,p = 0.002] in peritoneal effluent were also significantly higher in patients with peritonitis, irrespectively of lower effluent volumes [1741 (1661 – 1823) mL vs 2386 (2344 – 2428) mL,p < 0.001]. At the time of discharge of the patient from the hospital after a peritonitis episode, these adipokine concentrations in peritoneal effluent decreased significantly (for adiponectin p = 0.005, for leptin p = 0.034); however, they remained much higher than in PD patients without peritonitis: adiponectin 291 (119 – 463) ng/mL, p < 0.001; leptin 13.2 (5.9 – 25.5) ng/mL, p = 0.008. Receiver operating characteristic curve analyses revealed that an adiponectin concentration >180 ng/mL in peritoneal effluent had 100% sensitivity and 100% specificity, while leptin concentration >11.0 ng/mL in peritoneal effluent had 58.3% sensitivity and 95.5% specificity for the diagnosis of peritonitis (Figure 1). In patients with confirmed peritonitis, plasma concentrations of adiponectin and leptin did not differ significantly from values found in PD patients without signs and symptoms of peritonitis (Table 1). The differences in adiponectin and leptin concentrations in peritoneal effluent were not the consequence of the differences of their plasma levels.
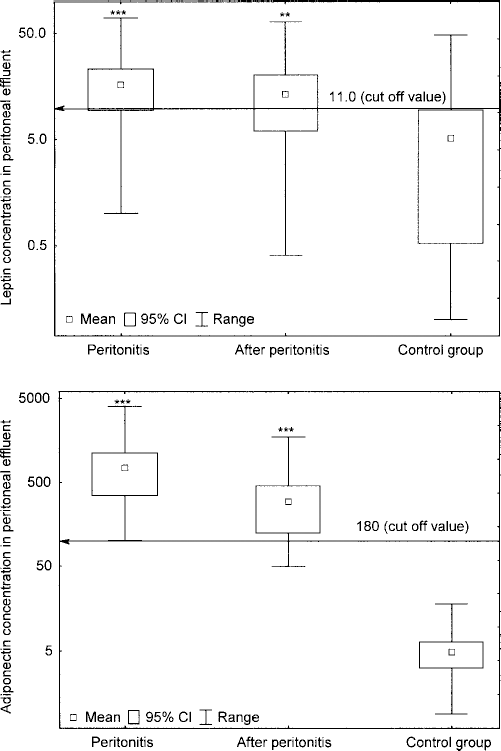
Concentrations (ng/mL) of leptin and adiponectin in peritoneal effluent (logarithmic scale) at the onset of a peritonitis episode and after recovery (1 day before discharge of the patient from the hospital) in comparison with peritoneal dialysis patients without peritonitis (control group).
Additionally, we calculated D/P ratios for adiponectin and leptin in both groups of patients. In the peritonitis group, calculated D/P adiponectin was 0.0364; in the control group, D/P adiponectin was 0.0003 (p < 0.001). A smaller although significant difference was also found for D/P leptin: 0.491 and 0.097 respectively (p < 0.001).
There was significant correlation between concentrations in peritoneal effluent and plasma for both adiponectin and leptin in patients with peritonitis (R = 0.45, p = 0.03 and R = 0.44, p = 0.03, respectively). In contrast, in the control group, similar correlation was significant only for leptin (R = 0.76, p < 0.001).
During peritonitis episodes, peritoneal clearance of leptin was significantly (p < 0.001) higher than in the control group [14.3 (8.0 – 20.5) mL/min vs 0.95 (0.47 – 1.43) mL/min respectively]. Similarly, peritoneal clearance of adiponectin during peritonitis was also markedly higher [1.056 (0.426 – 1.685) mL/min vs 0.003 (0.002 – 0.004) mL/min respectively (p < 0.001)]. At the time of discharge from the hospital, peritoneal clearance of leptin was almost normal [1.06 (0.43 – 1.68) mL/min], while adiponectin was still elevated [0.416 (0.159 – 0.673) mL/min].
Finally, in PD patients with peritonitis, the above-mentioned parameters were analyzed in subgroups of patients with and without diabetes. We found no statistically significant difference in either adiponectin [500 (206 – 793) ng/mL vs 1011 (189 – 1833) ng/mL (p = 0.38)] or leptin [5.4 (0.5 – 10.3) ng/mL vs 4.5 (3.0 – 5.9) ng/mL (p = 0.76)] concentrations measured in plasma and peritoneal effluent. The only parameter that reached statistical significance (p < 0.04) was serum CRP concentration, which was higher in diabetic patients [155.6 (84.8 – 226.4) mg/L vs 75.7 (18.9 – 132.5) mg/L].
Discussion
In the present study, we demonstrated for the first time that concentrations of both adiponectin and leptin in the peritoneal effluent were markedly elevated in PD patients with acute peritonitis already at the moment when such a suspicion arose, compared with PD patients without peritonitis. Moreover, for adiponectin, both the specificity and the sensitivity of effluent concentrations higher than 180 ng/mL at the onset of peritonitis reached 100%, with no overlap in any patient. It is worth noticing that pleocytosis assessed at the start of diagnostics was not sufficient to confirm peritonitis in 25% of patients. Also, simultaneously measured CRP levels in 4 of 24 patients (16.7%) did not allow us to clearly distinguish the patients with and without peritonitis. Thus, we assumed that this new parameter, peritoneal effluent adiponectin concentration, may be particularly useful for verifying the diagnosis of acute peritonitis in patients without a typical clinical picture. At the same time point, the specificity of peritoneal effluent concentration of leptin higher than 11.0 ng/mL reached 95.5% but had lower sensitivity (58.3%).
Both adiponectin and leptin are adipose tissue-derived proteins circulating in the blood. Adiponectin is a 244-amino acid protein with a molecular mass of 30 kDa; leptin is a 167-amino acid protein with a molecular mass of 16 kDa (7,8). The kidney is the main organ responsible for elimination/biodegradation of these proteins from the circulation (9,10); thus, in chronic kidney disease, elevated plasma concentrations of adiponectin and leptin have been found (9,11,12). Both adipokines were detected in the peritoneal effluent of PD patients in very low concentrations compared with plasma levels (11,13). Poor removal of these proteins with peritoneal effluent may be confirmed by their plasma concentrations, which were not lower in PD patients compared to hemodialyzed patients (11,13). Moreover, Heimbürger et al. (14) demonstrated that a small amount of leptin is locally produced by intraperitoneal adipocytes, which may be enhanced by intraperitoneal insulin administration given as the treatment of diabetes. There was no significant difference in peritoneal leptin clearance between diabetics and nondiabetics (14).
On the other hand, in PD patients undergoing an acute peritonitis episode, the peritoneal membrane transport of both low and high molecular weight substances increases significantly, probably due to an increased permeability and, to a lesser degree, as a consequence of an increased effective peritoneal surface area (6,15). However, our data do not exclude the increased intra-peritoneal production of adipokines in the course of a peritonitis episode; the positive correlation between their plasma and effluent concentrations possibly suggests its circulatory origin. This hypothesis could be verified and confirmed by experimental studies applying isotope-labeled adipokines.
We also monitored concentrations of adipokines in peritoneal effluent during recovery from an acute peritonitis episode, 1 day before discharge of the patient from the hospital. Mean time from diagnosis to recovery was 14 (12 – 16) days, and both adiponectin and leptin concentrations were significantly lower at that time point than at the onset of peritonitis, but were still much higher than in the control group.
In addition to clinical and laboratory parameters routinely used in the diagnosis of acute peritonitis, some new diagnostic modalities have been proposed in recent years. Several authors confirmed the diagnostic accuracy of different cytokines and growth factors, such as tumor necrosis factor-alpha, IL-6, IL-8 (16-18), IL-18 (19), IL-1 (20), and transforming growth factor-beta (20,21). Donovan et al. measured free elastase (a product of neutrophils recruited into the peritoneum) in peritoneal effluent from PD patients with acute bacterial peritonitis and found significantly higher quantities of uninhibited elastase compared to a control group of patients (22). Ruiz Solis et al. used abdominal scintigraphy with 99mTc-HMPAO-labeled leukocytes for early diagnosis of both peritonitis and exit-site infection (23). Recently, quantitative polymerase chain reaction for bacterial DNA was shown to correlate with regular microbiological tests and might be clinically useful in cases of “no growth” peritonitis (when the lack of bacterial growth is caused at least in part by growth inhibition due to antibiotic therapy) (24). However, we suggest that measurements of leptin and especially adiponectin concentrations in peritoneal effluent could be considered a convenient and effective method in the diagnostics of acute peritonitis in patients treated by continuous PD, at least in doubtful cases.
In summary, we have found that the increased concentration of leptin and especially adiponectin in peritoneal effluent seems to be a new and valuable marker of higher peritoneal membrane permeability during acute peritonitis. It is worth noticing that measurement of adiponectin effluent concentration is characterized by 100% sensitivity and 100% specificity for the diagnosis of this complication in PD patients.