
Abstract
Peritoneal dialysis (PD) is the preferred dialysis modality in children, but it relies on the patient or caregiver to perform dialysis daily at home. We describe the utilization of a modem transmission system in 2 pediatric PD patients to improve communication with the dialysis team, monitor compliance via frequent remote data collection, and decrease dialysis-related complications. A home dialysis modem was provided for each patient and connected to the home telephone line by the dialysis nurse. PD treatment data were transmitted daily to the dialysis unit, records entered into the patient's electronic medical record, and reviewed by the patient's PD nurse and/or pediatric nephrologist and adjustments made accordingly. This resulted in improved medical outcomes specifically related to fluid balance and cardiovascular health, ultimately facilitating renal transplantation in each case.
In summary, the use of the ProCard (Baxter Healthcare, Deerfield, Illinois, USA) has improved the ability to monitor home PD patients effectively. However, the additional use of the modem to transmit data on a more frequent basis can further enhance the care of chronic continuous cycling PD patients and should be considered in more challenging medical situations.
Keywords
We describe the utilization of a home modem transmission system in 2 pediatric PD patients to improve communication with the dialysis team, improve compliance with frequent remote data collection, and decrease dialysis-related or technical complications.
Methods
A dialysis nurse visited each patient's home and connected a modem to the dialysis machine and preexisting telephone landline. The modem was connected into a telephone jack and an electrical outlet; the telephone was then connected into the modem and the modem connected to the dialysis machine. The only additional cost associated with this system was a modem, which in this case was provided by Baxter. Initially, a test transfer was done through the system to the dialysis unit. If the modem connected to the Baxter program in the dialysis unit without problems, the dialysis staff would retrieve data from the dialysis machine from the ProCard. Of note, the HomeChoice Pro must be set to “Modem Connect Mode” to transmit.
To transmit data, a call was made by the dialysis unit to the telephone number linked to the modem. The patient turned on the dialysis machine, scrolled to “Patient Connect,” and clicked “Enter.” Once the connection was made, all treatments not previously downloaded from the ProCard were transmitted automatically to the dialysis unit. The ProCard self-erases; it will not contain any information if an attempt is made to download on site. Treatments were downloaded into the Baxter PD Link system and directly into the patient's electronic medical record. The time required each day to transmit the data was approximately 5 – 10 minutes.
Institutional Review Board approval and consent from each patient/parent were obtained.
Case 1
A 6-year-old white male with focal segmental glomerulosclerosis progressed to end-stage renal disease and began continuous cycling peritoneal dialysis (CCPD) in June 2004 after undergoing bilateral nephrectomies. Due to complaints of abdominal pain with fills, fill volumes were very slowly increased from 845 mL/m2/cycle initially to 1125 mL/m2/cycle over a period of 4 – 6 weeks. Blood pressures were normal based on 95% for height, age, and gender. In July 2004, he underwent an echocardiogram, which showed dilated left atrium and left ventricle (LV) with severe systolic dysfunction and concentric LV hypertrophy. The ejection fraction (EF) was 44%, with shortening fraction (SF) of 20%. A prior echocardiogram in May 2004 showed EF was 75% and SF 34%. The patient underwent vigorous CCPD with an optimized prescription (fill volumes 1265 mL/m2/cycle).
In August 2004, he was started on daily downloads. Data downloaded from the modem were transmitted directly into the hospital's electronic medical record and became part of the patient's medical record under a “flow sheet” section. In this section, data were organized into a running table, which then could be graphed. An example of the imported data is depicted in Figure 1(a) (table format) and Figure 1(b) (graph format). Records were reviewed daily by his dialysis nurse and nephrologist and his prescription was adjusted accordingly. Echocardiogram in October 2004 showed improvement in EF (52%) and SF (22%), with low normal contractility of the LV with mild dyskinesia; LV function and size were significantly improved. The patient continued on CCPD with results downloaded daily through December 2004. Echocardiogram in January 2005 showed normal LV size and systolic function with SF 39% and EF 78%. Blood pressures were in the normal range and patient's growth and development were normal. Medications were modified as necessary and electrolytes remained stable throughout the study. Subsequently, the patient underwent renal transplantation and to date is doing well with normal echocardiogram.
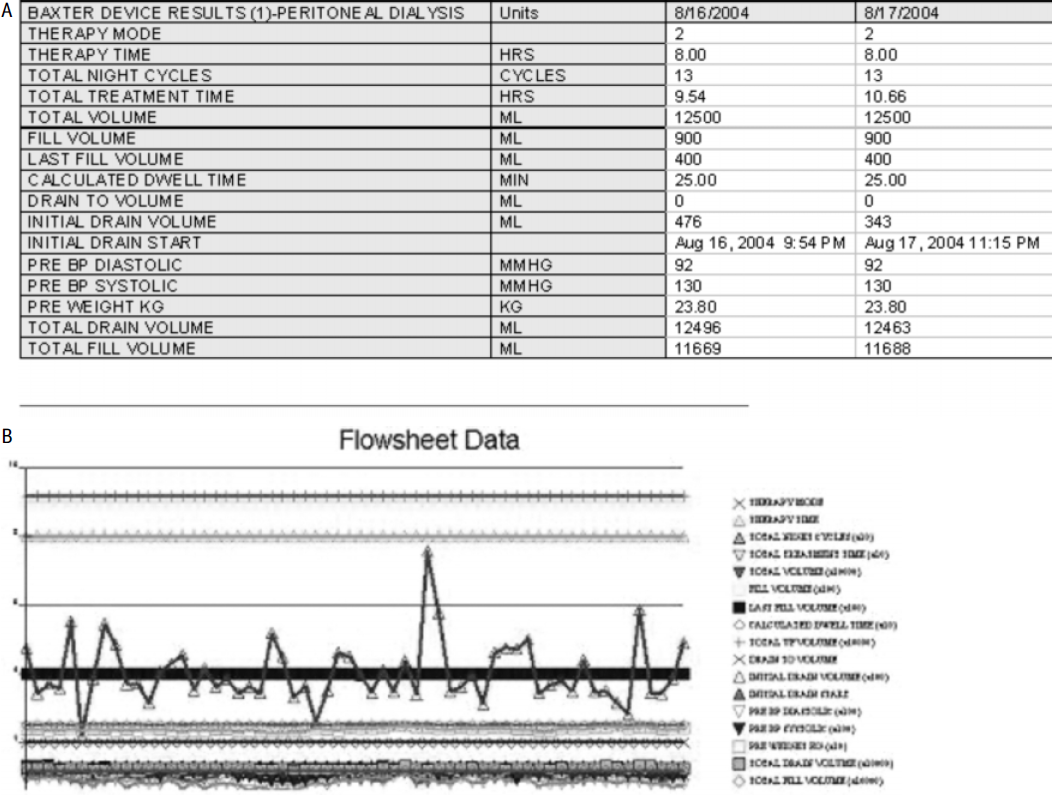
Example of data downloaded from the modem into the patient's electronic medical record as a “flow sheet,” in table format (A) and graphically (B).
Case 2
An 18-year-old girl with polycystic kidney disease began hemodialysis at the age of 13 years and switched to PD due to preference. She underwent renal transplantation in December 1999 but returned to PD in August 2000 after allograft failure. She was admitted in March 2003 with severe cardiac dysfunction. Echocardiogram demonstrated dilated LV, severe LV systolic dysfunction, left to right atrial septum bowing, mild to moderate mitral re-gurgitation, and trivial tricuspid regurgitation. The SF was 7% with EF of 25%. She was placed on milrinone and was eventually found to be very hypertensive after cardiac function improved. Her medications were adjusted and she was discharged. Repeat echocardiogram in March 2004 showed dilated LV with moderate LV dysfunction (SF was 19%) and normal right ventricular size and function.
Dialysis care was transferred to our facility in April 2005, at which time she was started on the ProCard for monitoring but lost her ProCard 2 months later. She was instructed to keep manual records and communicate with the dialysis team via telephone but did not adhere. Review of her ProCard in August 2005 showed she had performed only 7 dialyses during the month. In December 2005, she again returned to the clinic without her ProCard and was found to be hypertensive: 159/101 mmHg. She missed her visit in January 2006 due to lack of transportation and did not return calls in a timely manner. At this point, consent was obtained and the modem was set up at home. Over the next 4 – 5 months, her electrolytes improved and antihypertensive medication need decreased. She previously required three antihypertensive agents and needed only one agent by May 2006. She underwent successful renal transplant in July 2006. Repeat echocardiogram in January 2007 showed normalization of LV hypertrophy with SF 45% and EF 83%.
Discussion
Management of daily home dialysis can be difficult and stressful for the patient and family. A recent survey conducted in Great Britain identified variables impacting quality of health in technology-dependent patients, including patient education, improved communication, and teamwork (10). Although there are many benefits to home dialysis, it can also be a stressor. The patient or family member must be educated to provide treatments at home, whether the modality consists of continuous ambulatory peritoneal dialysis (CAPD) or CCPD. Although these modalities are preferred over hemodialysis in children, they must be performed daily at home by the patient/caregiver. The setup of dialysis involves numerous tasks requiring dexterity and the ability to maintain sterility (11). The child's room has to be modified and can often resemble a “hospital setting,” creating a source of anxiety for the family. In addition, parent and patient are responsible for other medical duties such as oral medication administration, home injection therapies, etc. Travel can be challenging and requires significant advance planning. This can be burdensome for a family. Further, when problems arise, troubleshooting may be difficult, requiring multiple telephone calls to the dialysis unit and/or technical company. In the case of CAPD, the patient must maintain sterility and accommodate their lifestyle in order to perform multiple manual exchanges daily. This can make it difficult to maintain a “normal childhood lifestyle.” Due to these and other variables, many PD patients find it difficult to maintain compliance.
Measurement of compliance remains difficult and, so far, no single reliable method to assess patient adherence to prescriptions has been validated, in pediatric or adult dialysis patients. Prior to an electronic system, patients were asked to manually keep home records of vital signs, dialysis fill volumes, ultrafiltration volumes, duration of dialysis, etc. The accuracy of records could be questionable, especially in adolescents. It has been our experience that many patients omit information, forget to bring records to the visits, or fabricate information.
Bernardini et al. performed serial home visits to assess for safety and independence with dialysis, and inventories of dialysis supplies were taken (5). This study concluded home visits to be a reliable way to measure compliance. However, this may not be practical as most treatments are performed overnight and visits are made during the day. Frequent visits may be required, which is neither time- nor cost-effective. Alternatively, Figueiredo et al. (6) described measurement of compliance in adult PD patients by evaluating supply inventories. In 30 home PD patients in Brazil, the investigators performed initial telephone interviews to determine home dialysis supply inventories and patient well-being. A follow-up telephone call was made 1 – 2 months later to assess actual number of exchanges performed based on consumption of dialysate bags. Compliance, defined as patients performing at least 90% of prescribed exchanges, was shown in only 70% of patients. Adequacy (Kt/V) was found to be suboptimal as well. Shapiro et al. (12) described a compliance rate of approximately 80% in home dialysis patients. Amici et al. correlated actual adequacy measurements with those predicted by the Baxter PD Adequest program to determine adherence. Approximately 22% of patients were considered non-adherent (7); however, the computer program is a model that simulates PD adequacy and is not validated to measure adherence.
The ProCard was introduced by Baxter Healthcare in 2000. In 2002, Juergensen et al. (8) and Neri et al. (9) first described the use of the ProCard to enhance compliance in home CCPD patients. The investigators followed 42 adult CCPD patients that received education about the ProCard to determine if extended education encouraged better adherence. Compared to historical rates, this group reported 83% of patients had achieved compliance rates of 95% or greater compared to 43% prior to the ProCard. The number of patients with <90% compliance decreased from 17% to 10%. This study concluded that patient education with the ProCard significantly enhanced patient compliance.
Although the ProCard alone can improve patient compliance, many PD patients, especially pediatric patients, require closer monitoring and adjustment of dialysis prescription to accommodate for growth and development. Fine control of volume status is essential to prevent end organ damage but can be difficult to achieve. Tele-medicine has been used to improve monitoring of home dialysis patients. Mitchell et al. (13) followed 1 hemodialysis patient remotely (approximately 300 km away) in Australia over 3 months; Stroetman et al. (14) followed 5 CAPD patients remotely and showed improved compliance in dialysis regimens. Others have described their experiences in a limited number of adult PD patients. Ghio et al. (15), from Italy, described the effectiveness of a telemedicine system in 2 children to improve monitoring. This system included the use of a home modem through which daily records were downloaded, and a home video system, which allowed for remote patient examination. Cargill and Watson tried to improve communication between the patient and the facility by videophone, but found only 1 of 3 patients used the machine over a 3-month period (16). Overall, while many patients may find closer monitoring intrusive, others may find the enhanced monitoring beneficial as additional support may encourage honesty and better communication.
We know of no other published pediatric CCPD data in the United States describing remote home monitoring of pediatric PD patients via modem and ProCard. Our reports describe the use of a modem system to provide monitoring to enhance compliance, potentially improving patient care. In Case 1, the patient was chronically volume overloaded, resulting in cardiac dysfunction. After the implementation of modem monitoring, the patient's fluid status became easier to manage. By altering the dialysis prescription daily, his volume status improved, decreasing preload to the heart, and ultimately his cardiac function normalized, allowing him to be transplanted. He continues with normal cardiac function and normal growth and development, and is thriving. In Case 2, the dialysis team was able to monitor compliance to help decrease the stress associated with home CCPD, thereby improving hypertension and cardiac function. This enhanced the patient's compliance and ultimately resulted in greater improvement in health, contributing to successful transplant. One limitation of the ProCard is that it cannot be altered remotely, making patient cooperation mandatory. It is important to download the ProCard at each visit to verify prescription and existing data.
In summary, the ProCard has improved the ability to monitor home PD patients. The use of the modem to transmit data on a more frequent basis can further enhance the care of chronic CCPD patients and should be considered to optimize home dialysis delivery.