
Abstract
Objective
The prevalence of left ventricular hypertrophy (LVH) reaches 75% in patients with end-stage renal disease. In patients on peritoneal dialysis (PD), some factors, such as hypertension, volume overload, serum albumin, and residual renal function, have been reported to be related to LVH. Dyslipidemia often occurs in PD but it remains unclear whether dyslipidemia is related to LVH. We investigated the relationship between clinical parameters, including lipid profile, and left ventricular mass index (LVMI).
Methods
In this cross-sectional study, 34 patients undergoing PD for more than 1 year without combined therapy with hemodialysis were included. We recorded the patients’ clinical data and related those parameters with LVMI as evaluated by echocardiography.
Results
The patients included 23 males and 11 females (age 62.2 ± 12.1 years, duration on PD 31.6 ± 15.6 months). Mean LVMI was 142 ± 37 g/m2. In univariate analysis, urine volume (r = -0.493, p = 0.003), total cholesterol (r = -0.418, p = 0.01), high-density lipoprotein cholesterol (HDL-C; r = -0.374, p = 0.02), and human atrial natriuretic peptide (hANP; r = 0.600, p < 0.001) significantly correlated with LVMI. Stepwise multiple regression analysis showed that hANP (β= 0.524, p = 0.001) and HDL-C (β= -0.422, p = 0.007) were independently associated with LVMI (r2 = 0.32).
Conclusion
Strict volume control and salt restriction is essential for prevention of LVH. The role of HDL-C in the development of LVH in PD patients remains to be determined.
Keywords
Methods
Patients
Thirty-four patients undergoing PD in our department were included in this study. To meet the inclusion criteria, the patient had to be undergoing PD for more than 1 year and not undergoing combined therapy with HD. We recorded patients’ sex, age, duration on PD, peritoneal ultrafiltration, urine volume, dialysate-to-plasma creatinine ratio (D/P Cr) after 4-hour dwell during their peritoneal equilibration test, systolic and diastolic blood pressure, pulse pressure, presence of diabetes mellitus, hemoglobin, serum albumin, uric acid, calcium, phosphorus, calcium–phosphorus product (CaxP), intact parathyroid hormone (iPTH), total cholesterol, triglyceride, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C); the ratio of apolipoprotein A1 to apolipoprotein B (ApoA-1/ApoB), lipoprotein(a) [Lp(a)], total homocysteine (tHcy), C-reactive protein (CRP), human atrial natriuretic pep-tide (hANP); and administration of angiotensin-converting enzyme-inhibitor (ACEI), angiotensin II receptor blocker (ARB), and statin. Blood pressure was measured at the patient's home. The values for D/P Cr, ApoA-1/ ApoB, Lp(a), and tHcy were obtained in 26 patients. In addition, we measured brachial–ankle pulse wave velocity (baPWV) using the oscillometric method as an index of aortic stiffness. baPWV was automatically calculated using a Colin Waveform Analyzer (PWV/ABI; Colin Medical Technology, Komaki, Japan). The validity, reproducibility, and clinical significance of noninvasive baPWV have been reported elsewhere (14).
We examined whether these parameters correlated with LVMI. The ethics committee of our hospital approved the study and all patients gave their informed consent.
Echocardiography
Two-dimensional and M-mode echocardiographic examinations were performed in all patients by a single operator. Left ventricular (LV) mass was calculated according to the Penn convention (15): LV mass (g) = 1.04 x [(LVDd + IVSth + PWth)3 – (LVDd)3] – 13.6, where LVDd is LV end-diastolic diameter, IVSth is interventricular septal thickness, and PWth is LV posterior wall thickness. LVMI was calculated by dividing LV mass by body surface area (in meters squared). The cutoff value of LVMI for LVH varies extensively; the definitive criterion is absent (16). Therefore, we recorded a continuous variable of LVMI and related LVMI with clinical parameters.
Statistical Analysis
Data are shown as mean ± SD. Comparisons between two groups were performed using Mann–Whitney U test. Correlations were tested by Spearman's correlation rank test. Stepwise multiple regression analysis was used to select independent risk factors among parameters selected by univariate analyses. A p value less than 0.05 was considered statistically significant. All statistical analyses were performed using SPSS 10.0 software (SPSS Inc., Chicago, Illinois, USA).
Results
Clinical characteristics of the 34 patients are shown in Table 1. The patients included 23 males and 11 females; their mean age was 62.2 years. They had been treated with PD for 31.6 months (range 12 – 70 months). Mean peritoneal ultrafiltration was 879 mL/day; urine volume was 736 mL/day. Mean systolic and diastolic pressures were 148 mmHg and 80 mmHg respectively. Eleven patients (32.4%) had diabetes mellitus. ACEI/ ARB and statin were administered in 23 (67.6%) and 14 patients (41.2%) respectively. Mean LVMI was 142 ± 37 g/m2.
Patients’ (n = 34) Clinical Characteristics
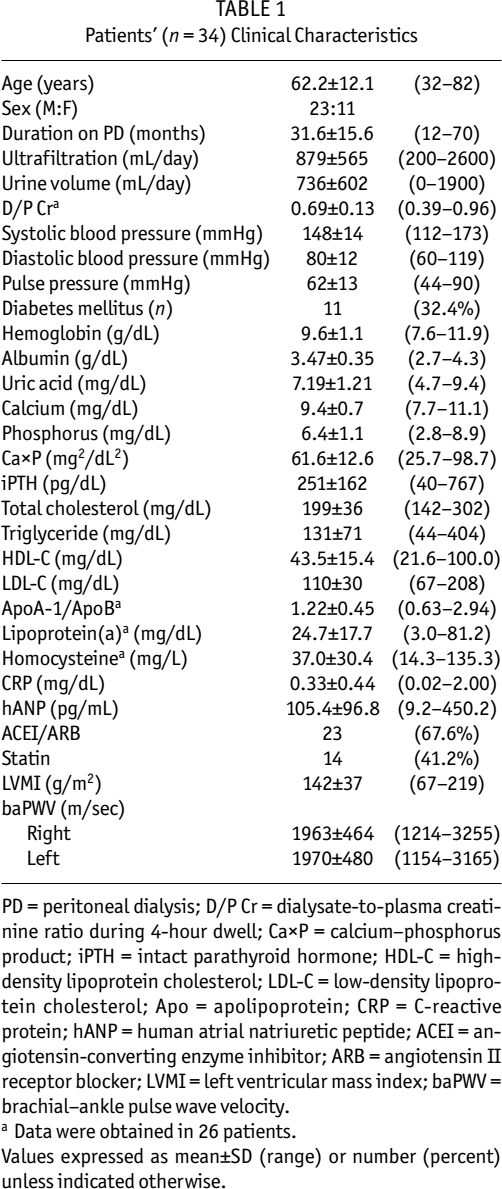
PD = peritoneal dialysis; D/P Cr = dialysate-to-plasma creatinine ratio during 4-hour dwell; CaxP = calcium–phosphorus product; iPTH = intact parathyroid hormone; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol; Apo = apolipoprotein; CRP = C-reactive protein; hANP = human atrial natriuretic peptide; ACEI = angiotensin-converting enzyme inhibitor; ARB = angiotensin II receptor blocker; LVMI = left ventricular mass index; baPWV = brachial–ankle pulse wave velocity.
Data were obtained in 26 patients.
Values expressed as mean±SD (range) or number (percent) unless indicated otherwise.
Table 2 shows comparisons of LVMI based on categorical parameters. Male patients showed higher LVMI than female patients, with marginal significance (149 ± 32 vs 127 ± 45 g/m2, p = 0.08). In addition, diabetic patients showed higher LVMI than nondiabetic patients (156 ± 31 vs 135 ± 39 g/m2) but the difference did not reach statistical significance (p = 0.07).
Comparisons of Left Ventricular Mass Index (LVMI) Based on Categorical Parameters
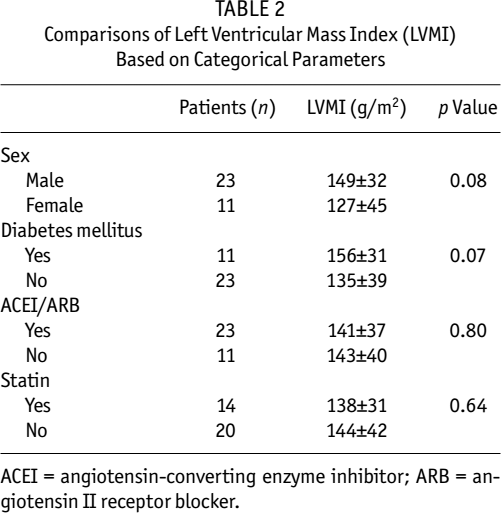
ACEI = angiotensin-converting enzyme inhibitor; ARB = angiotensin II receptor blocker.
Table 3 shows correlation coefficients between LVMI and continuous parameters. Duration on PD and D/P Cr did not correlate with LVMI. Urine volume showed significant negative correlation with LVMI (r = –0.493, p = 0.003), but peritoneal ultrafiltration did not. The correlation between systolic blood pressure and LVMI was not statistically significant (r = 0.297, p = 0.08). Hemoglobin also did not correlate with LVMI. Total cholesterol (r = –0.418, p = 0.01) and HDL-C (r = –0.374, p = 0.02) showed significant negative correlation with LVMI. LDL-C and ApoA-1/ApoB showed negative correlation with LVMI, with marginal significance. hANP showed the strongest correlation (r = 0.600, p < 0.001). baPWV did not correlate with LVMI.
Correlation Coefficients Between Left Ventricular Mass Index and Clinical Parameters

PD = peritoneal dialysis; D/P Cr = dialysate-to-plasma creatinine ratio during 4-hour dwell; CaxP = calcium–phosphorus product; iPTH = intact parathyroid hormone; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol; Apo = apolipoprotein; CRP = C-reactive protein; hANP = human atrial natriuretic peptide; baPWV = brachial–ankle pulse wave velocity.
Data were obtained in 26 patients.
Stepwise multiple regression analysis showed that, among the parameters selected by univariate analysis, hANP (r = 0.524, p < 0.001) and HDL-C (r = –0.422, p = 0.007) independently correlated with LVMI (Table 4).
Stepwise Multiple Regression Analysis for Left Ventricular Mass Index
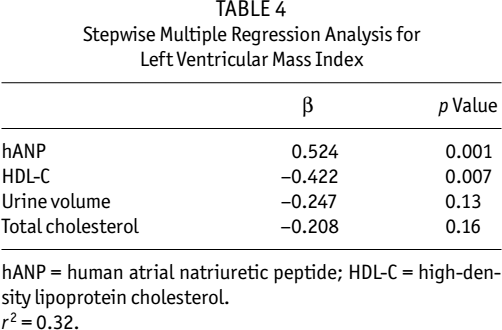
hANP = human atrial natriuretic peptide; HDL-C = high-density lipoprotein cholesterol. r2 = 0.32.
Discussion
In previous studies in PD, indices reflecting hypervolemia, such as increased hANP (8) and hypertension (8-10), were related to LVH. Many studies have indicated hypervolemia in PD patients. In a multicenter survey, Nakayama et al. reported that, of 203 Japanese patients on PD for 53.6 ± 35.0 months, 60 had clinical symptoms of hypervolemia (17). Other authors have reported that, compared with HD patients, PD patients have a higher incidence of LVMI caused by hypervolemia (8,18). However, strict volume control and salt restriction led to normal LVMI in PD (19,20). Thus, volume control is apparently essential for prevention of LVH, as ascertained also in our study. hANP was most significantly associated with LVMI. Urine volume is related not only to volume control but also to residual renal function. We obtained a notable finding in that urine volume showed significant negative correlation with LVMI, but peritoneal ultrafiltration did not. This result suggests that unknown uremic toxins removed by urine but not removed by PD may be related to LVH. In fact, it has been reported that residual renal creatinine clearance negatively correlates with LVMI (10). The importance of residual renal function is increasingly stressed in PD. Residual renal function plays an important role in maintaining body fluid balance, phosphorus control, removal of middle molecular uremic toxins, and prevention of heart valve calcification and cardiac hypertrophy (21). However, residual renal function may depend on hypervolemia, as suggested by Gunal et al. (22). Can residual renal function be preserved under strict volume control? Although icodextrin solution may be a clue, the problem of residual renal function and volume control is controversial (23).
To our knowledge, this is the first study reporting that decreased HDL-C is independently associated with LVH in PD patients. Compared with HD patients, PD patients show a more atherogenic lipid profile: increases in total cholesterol, triglyceride, LDL-C, and ApoB and a decrease in HDL-C (11,12). HDL-C has antiatherogenic effects, such as removal of cholesterol from atherosclerotic plaques and cells, antioxidant effects, and preservation of blood viscosity by promotion of erythrocyte membrane deformability (12). Decreased HDL-C is an independent determinant for LVH in patients with essential hypertension (24,25). However, this relationship has not been reported in PD patients. In our study, univariate analysis showed that LVMI negatively correlated not only with HDL-C but also with atherogenic lipids, including total cholesterol and LDL-C. The results of our univariate analysis may reflect the relationship between malnutrition and LVH. However, the fact that only decreased HDL-C was independently associated with LVH by multivariate analysis suggests harmful mechanisms of decreased HDL-C other than malnutrition. Both low HDL-C and LVH are known to be related to endothelial dysfunction (26,27). Impairment of endothelium-dependent vasodilatation has been reported in PD patients (28). Although we speculate that decreased HDL-C is related to LVH via endothelial dysfunction, we could not evaluate flow-mediated dilatation, which reflects endothelium-dependent vasodilatation. Since baPWV has been reported to correlate with flow-mediated dilatation (29), we tested the correlation between baPWV and LVMI. To date, the correlation between PWV and LVMI has been reported in HD patients (30) but not in PD patients. In this study, we could not show the correlation.
In our study, there was no difference in LVMI between patients administered and patients not administered ARB, ACEI, or statin. Patients showing higher blood pressure or severe dyslipidemia tended to be administered these drugs. All these drugs have beneficial effects on vascular endothelial function (31,32) and LVH (33,34). In addition, it is of interest that administration of HDL-C improved endothelial function in patients with hypercholesterolemia in Spieker et al.‘s study (35). Some trials failed to show the effects of an increase in HDL-C on the progression of atherosclerosis or mortality in the general population or in patients on HD (36,37). Recently, a retrospective cohort study showed that lipidmodifying medication therapy might be associated with improved clinical outcomes in PD patients (38). The clinical importance of dyslipidemia in the PD population might be different from that in the general or the HD population.
There are some limitations in our study: the cross-sectional study design, small sample size, and the single-center study design make it difficult to draw general conclusions and causal relationships. Studies resolving these limitations are required.
In conclusion, we report that increased hANP and decreased HDL-C were independently associated with LVH in PD patients. Strict volume control is essential for the prevention of LVH. In addition, we showed a potential association between dyslipidemia and LVH in this study. The role of HDL-C in the development of LVH in PD patients remains to be determined in an interventional study.