
Abstract
Background
Laparoscopic techniques for placement of peritoneal dialysis catheters are becoming increasingly popular. In this paper, we report the results of one-port laparoscopic placement of Tenckhoff catheters in 79 patients in our center.
Method
Videoscopic monitoring was performed via a port inserted in the left upper quadrant and the catheter was placed via a pull-apart sheath through an incision near the umbilicus. The tip and the deep cuff of the catheter were placed into the true pelvis (on the urinary bladder) and into the rectus sheath respectively. A subcutaneous tunnel was created and a point midway on the umbilico-crestal line was selected as the exit site of the catheter. Catheters were capped for 2 weeks before initiation of peritoneal dialysis. Mean duration of the operation was 25 minutes.
Results
Four patients died during the follow-up period, all due to other medical problems, and 4 patients underwent renal transplantation. During a 48-month follow-up, catheter-related complications were catheter migration (1.3%; month 1), dialysate leakage (1.3%; month 1), port-site hernia (3.8%; after 6 months), exit-site infection (2.5%; months 1 and 9), and bacterial peritonitis (2.5%; after 6 months). Catheter survival was 97.2% in our series.
Conclusion
We obtained a low complication rate and a high catheter survival rate with this one-port laparoscopic technique.
Keywords
Most techniques use two to four ports (1,6-11); however, each port entry creates a weak abdominal site where a hernia or leak could later occur (12). A one-port technique has been recently introduced (13) and used for the management of obstructed catheters and placement of catheters into complicated abdomens (14-17). In the present paper, we report and evaluate the results of the one-port laparoscopic technique in placing PD catheters in 79 chronic renal failure patients treated in our center. To our knowledge, this study represents the largest study to date on this technique.
Patients and Methods
Between January 2002 and August 2006, 79 consecutive chronic renal failure patients (46 men, 33 women; mean age 50 years, range 19 – 83 years) underwent laparoscopic placement of Tenckhoff Toronto–Western Hospital catheters performed by 1 experienced surgeon in our center. All patients were eligible to receive general anesthesia and none had had a previous peritoneal catheter placed. The contraindications for the technique were those regarding general anesthesia and pneumoperitoneum. Prophylactic antibiotics, usually a cephalosporin, were administered prior to the procedure. All patients gave their informed consent and the ethics committee in our university approved the study protocol.
Patients were placed in a supine position. A 5-mm port was inserted for videoscopic monitoring through a left upper quadrant incision at a point just lateral to the margin of left rectus muscle and inferior to the costal margin on the midclavicular line. This port also served for pneumoperitoneum installation with carbon dioxide, with intra-abdominal pressure kept below 12 mmHg during the operation. A thorough inspection of the abdominal cavity was performed, with special attention to the presence of adhesions and herniations that could potentially cause catheter malfunction after the induction of PD.
In order to prevent omentum wrapping and subsequent catheter obstruction, omentopexy was performed in case of a large or bulky omentum (18). Omentectomy was not necessary in any of the patients. In a few cases with previous abdominal surgery, adhesiolysis was required prior to PD catheter placement. Adhesiolysis was performed laparoscopically using two extra ports: one inserted 5 cm to the left and the other 5 cm to the right of the umbilicus.
The Peritoneal Catheter Kit (Quinton Instrument Company, Seattle, Washington, USA) was used for catheter placement. A 5-mm incision was made 2 cm left of and 2 cm inferior to the umbilicus. Under direct visualization through the camera, a pull-apart sheath was then inserted in a caudal direction (at a 45 degree angle) toward the bladder and rectum. We used a 5 mm, 0 degree telescope (Karl Storz, Tuttlingen, Germany). The Tenckhoff catheter (curled type) was passed through the pull-apart sheath over a 90-cm stylet into the peritoneal cavity. The tip of the catheter was placed in the true pelvis (on the urinary bladder), with the deep cuff in the rectus sheath. The stylet was then removed.
The pull-apart sheath was removed, leaving the Tenckhoff catheter in the peritoneal cavity. A subcutaneous tunnel was then created for the catheter. A point midway on the umbilico-crestal line was selected as the output site of the catheter. With the aid of the tunneling stylet of the catheter kit, a subcutaneous tunnel was fashioned in a lateral caudal direction. The end of the catheter attached to the stylet was advanced into the tunnel and pulled out from the above-mentioned point (Figure 1).

Cephalocaudal direction of the port used for catheter placement (upper panel). Result after subcutaneous tunneling and catheter exit (lower panel).
To ensure satisfactory function of the catheter, we made sure there was no kinking; patency was checked by small amounts of peritoneal fluid flushed through the catheter's lumen (in–out test). The abdomen was gradually deflated while the position of the catheter tip was checked and all incisions were then sutured. The catheter was heparinized and kept capped for 2 weeks. Following catheter placement, all patients were trained by expert nurses on catheter handling and avoidance of constipation. Low-volume exchange of dialysate fluid (a maximum of 250 cc) was practiced during the 2 weeks prior to the initiation of dialysis.
Catheter-related complications were classified as early (<6 months) versus late (≥ 6 months), and mechanical (hemorrhage, obstruction, catheter migration, leakage, hernia) versus infectious (exit-site infection, tunnel infection, peritonitis).
Results
Table 1 shows a summary of patients’ characteristics and the results. There was no history of previous PD cycles in our series. Six patients had a history of previous abdominal surgery, 4 of whom required adhesiolysis prior to placement of the peritoneal catheter. Omentopexy was performed in 11 patients. All procedures were completed laparoscopically and the dialysis catheter was successfully placed in the desired position. General anesthesia was tolerated well by all patients. Mean duration of the operation was 25 minutes (range 15 – 35 minutes). Duration of hospitalization was 1 day for 60 patients, 2 days for 12 patients, 3 days for 5 patients, and 4 days for 2 patients. There was no intraoperative complication or surgical mortality.
Characteristics of Seventy-Nine Patients and the Results
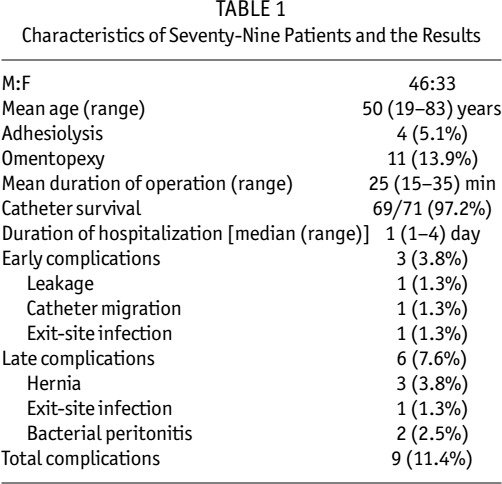
We had three cases of early complications and six cases of late complications. We did not have any cases of hemorrhage, flow obstruction, or tunnel infection. There was one (1.3%) incidence of catheter migration and one (1.3%) incidence of early leakage, both during the first month. Both patients were treated successfully with low-volume exchange and interruption of PD for 15 days while catheter repositioning was achieved by radioscopic wire manipulation. There were 3 (3.8%) hernias, 2 in the site of port entry and 1 in the site of catheter entry, all of which occurred after 6 months. Two (2.5%) patients developed exit-site infection, 1 during the first month and the other during month 9; both were treated successfully with appropriate antibiotics. Two (2.5%) patients required catheter removal due to bacterial peritonitis that occurred after 6 months.
Patients were followed for an average of 48 months (range 4 – 60 months). Duration of PD was the same, that is, 48 months on average (range 4 – 60 months). Two patients died prior to initiation of PD (a man due to cardiac arrest during hemodialysis and a woman due to cardiac tamponade). Four patients died during the follow-up period, all due to other medical problems (2 cases of heart failure, 2 cases of liver cirrhosis), and 4 (5.1%) patients underwent renal transplantation. The duration of PD in the latter group was 12, 12, 16, and 24 months. The PD catheter was removed following successful transplantation. To date, 69 patients remain on PD and all catheters are functioning properly.
Discussion
The laparoscopic approach to placement of Tenckhoff PD catheters, introduced in the 1980s (19), has advantages over open and percutaneous surgical techniques, such as a lower incidences of flow obstruction and visceral injury (20) and the ability to perform concomitant procedures (21). The one-port approach (13) was developed later for the management of obstructed catheters and placement of catheters into complicated abdomens.
Although the same single-port method has been used in previous studies, on both adults and children (15,17,22), and one of the ports in some two-port studies has actually been used in the same manner as the pull-apart introducer (23,24), our study is the largest to date. This advantage makes it possible to evaluate complication rates and catheter survival more accurately. While obstruction of dialysate flow (incidence 12.5% – 17.5%), port-site hernia (25), and leakage (incidence 5% – 30%) are three major causes of PD catheter failure (12,26,27), complications were rare in our study and long-term catheter survival was 97.2%.
Our complication rates over long-term follow-up (leakage 1.3%, catheter migration 1.3%, exit-site infection 2.5%, peritonitis 2.5%, hernia 3%) stand comparably low among other studies (12). A recent large prospective study (27) compared the incidence of flow obstruction among three methods: 63 catheters implanted by open surgery, 78 catheters implanted by basic laparoscopy without associated interventions, and 200 catheters implanted by advanced laparoscopic techniques, including rectus sheath tunneling, selective prophylactic omentopexy, and selective adhesiolysis. Flow obstruction followed in 0.5% of the implantation procedures in the advanced group, 17.5% in the open dissection group, and 12.5% in the basic laparoscopy group (p < 0.0001).
Tunneling lessens the risk of catheter migration that would otherwise occur in about 20% of cases and result in poor return of the dialysate (16,22,28). Fixing the catheter tip into the pelvis by nonabsorbable sutures can also prevent catheter migration (28), but we preferred to avoid the potential risk of mechanical intestinal obstruction that exists with the latter technique. By using the tunneling technique, we also eliminated the need for repeat surgery in case of catheter dysfunction. It has been shown that herniation occurs most commonly through port sites larger than 10 mm, and using 5-mm ports reduces the chance of port-site hernia. Also, longer procedures carry a higher risk (25). The low incidence of hernia (3%) in our series and a mean operating time of 25 minutes support this idea. Finally, we attribute the particularly low rate of infectious complications in our series to the implantation technique used, the 2-week interval before the initiation of PD, patient training, and post-insertion catheter handling.
General anesthesia provides patient comfort during laparoscopy, especially when carbon dioxide (which is irritating to the peritoneum) is used for insufflation of the abdomen. As a result, general anesthesia has become a routine procedure in laparoscopic techniques. The use of general anesthesia, however, necessitates careful patient selection, taking into account contraindications and potential complications. It is, however, worth noting that local anesthesia has also been used in laparoscopic approaches for PD access (21,29,30); in particular, minimally invasive needlescopic techniques often use local anesthesia for placement of Tenckhoff catheters (31).
In summary, we reported the results of our experience with one-port laparoscopic placement of Tenckhoff catheters in 79 patients. Catheter survival was high and both early and late complication rates were low over an average of 48 months of follow-up.