
Abstract

[PP-228] Successful Treatment with Lamivudine of Type B Acute Hepatitis in a PD Patient
Chronic hepatitis is uncommon in peritoneal dialysis (PD) patients because of less exposure to blood and blood products; acute hepatitis is highly unusual. Here, we report the case of a 79-year-old woman on continuous ambulatory PD (CAPD) for 2 years for end-stage renal disease resulting from multiple myeloma.
The patient was receiving melphalan and prednisone at home for myeloma. She had been admitted several times for pancytopenia because of confusing melphalan and prednisone, and had received repeated blood transfusions. The patient was admitted again with pancytopenia (hemoglobin 5.1 g/dL; white blood cell count 1200/mL; Tr 4000/mL) and jaundice. Acute hepatitis B was diagnosed (HBsAg became positive in a previously negative patient). The evolution indicated a subacute hepatic failure, with initially very high transaminases, decreasing thereafter (ASAT 2500–60 IU/L, ALAT 2800–51 IU/L), intrahepatic cholestasis (bilirubin up to 11.8 mg/dL total and 10.5 mg/dL direct, alkaline phosphatase up to 270 IU/L) and a sonographically shrinking liver.
We started her on lamivudine therapy (together with classical supportive therapy), with a slow positive evolution: liver enzymes and bilirubin returned to near-normal values (ASAT 52 IU/L, ALAT 45 IU/L, total bilirubin 1.4 mg/dL), and jaundice disappeared. Unfortunately, pancytopenia persisted; the patient developed fatal upper gastrointestinal hemorrhage and died. We speculate on the value of lamivudine therapy in patients with acute hepatitis B on dialysis.
Interestingly, despite advanced age and acute disease, the patient had a quite unaffected state of consciousness, rather unusual in such patients. We hypothesize that PD may have a positive effect in patients with chronic or acute liver injury, possibly through elimination of bilirubin and other toxins (although we were not able to quantify them). We emphasize that, despite rigorous testing of blood, repeated transfusions are still a risk factor for hepatitis.
Zugravu A., Stancu S., Mircescu G., “Carol Davila” Univer. of Medicine and Pharmacy and “Carol Davila” Clinical Hosp. of Nephrology, Bucharest, Romania.
[PP-229] Effect of N-Acetylcysteine Supplementation on Inflammatory and Oxidative Stress Markers in PD Patients: A Randomized Placebo-Controlled Study
Background: Inflammation (IF) and oxidative stress (OS) are cardiovascular risk factors in patients (pts) with renal disease. The antioxidant N-acetylcysteine (NAC) has been shown to reduce cardiovascular events in hemodialysis pts.
Objectives: To determine the effect of oral NAC (1200 mg daily), a thiolcontaining antioxidant that inhibits nuclear factor κB activation in vitro, on plasma levels of IF and OS markers in peritoneal dialysis (PD) pts.
Methods: We performed a randomized placebo-controlled study over 8 weeks in 30 pts (40% men; age: 52±13 years) on regular PD (2 groups of 15 pts in each arm, matched for age and sex).
Results: Of 30 pts, 22 completed the study (n=12 NAC, n=10 placebo). IF was assessed pre- and post-treatment in both groups through measurements of plasma high-sensitivity C-reactive protein, interleukin-6 [IL-6 (pg/mL)], tumor necrosis factor α, and pentraxin. The OS markers analyzed were pentosidine, homocysteine, serum L glutathione, serum glutathione, asymmetric dimethylarginine, total antioxidant status, and sulfhydryls. In the treated group, baseline NAC was 2.6 μmol/L on average; its concentration increased to 24.8 μmol/L (p=0.007). After 8 weeks of follow-up, a significant reduction in median level of IL-6 [9.4 pg/mL (range: 4.5–31 pg/mL) vs. 7.6 pg/mL (4.9–13.5 pg/mL),p=0.006] was observed in the NAC group.
Changes in other IF and OS markers from baseline to post-treatment were nonsignificant.
Conclusions: In this small cohort of PD pts, short-term oral supplementation with NAC had no effect on OS markers. However, it resulted in a significant reduction in IL-6 levels, suggesting that antioxidant therapy with NAC may be useful in blunting IF response.
Nascimento M.M.1, Suliman M.2, Anderstam B.2, Martins C.2, Hayashi S.2, Marchioro J.1, Chinaglia T.1, Silva M.1, Riella M.2, Lindholm B.1, Dept. of Nephrol.,1 Evangelic Med School, Curitiba, Brazil, and Divs. of Baxter Novum and Renal Med.,2 Karolinska Inst. Stockholm, Sweden.
[PP-230] Peritonectomy is a Successful Treatment for Patients with Encapsulating Peritoneal Sclerosis following Renal Transplantation
Encapsulating peritoneal sclerosis (EPS) is an increasingly recognized complication of long-term peritoneal dialysis (PD), associated with deposition of fibrous sheets that constrict and restrict the bowel. In the past, surgical intervention has been associated with high mortality. EPS following renal transplantation is a new phenomenon, occurring relatively soon post-transplant despite immunosuppression. Peritonectomy has been used to treat PD patients with EPS.
We collected outcome data on renal allograft recipients who developed EPS following transplantation in a single center over 3 years (2004– 2006). Diagnosis was based on both clinical and radiologic findings, with surgical confirmation. Patients with a clinical picture including ascites, deteriorating nutrition status, raised inflammatory markers, and bowel obstruction underwent adhesiolysis and complete peritonectomy.
During the study period, 11 patients developed EPS following renal transplantation. Clinical findings included ascites and symptoms of bowel obstruction. Computed tomography findings included ascites, peritoneal thickening and calcification, abdominal cocoon, bowel thickening, and dilatation. Ten patients underwent surgery, and 1 patient was treated conservatively and achieved a normal nutritional state. In 9 patients who underwent peritonectomy and adhesiolysis, 7 are now eating a normal diet. In 5 of the 7, residual symptoms persist, including nausea, abdominal pain, and constipation. One patient underwent a repeat peritonectomy and is now almost symptom-free. In this cohort, 1 death occurred.
This is the first report of peritonectomy in the management of EPS following renal transplantation; normal diet was achieved in most patients. Unlike the high surgical mortality (up to 33%) seen in previous reports, only 10% mortality has occurred in this group. EPS should be considered in patients with post-transplant chronic abdominal symptoms and ascites. The key to successful surgery is early semi-elective peritonectomy after adequate preparation.
Summers A.M., De Freitas D.G., Hurst H., Taylor P., Hutchison A.J., Dunn L., Brenchley P.E., Augustine T., Manchester Inst. of Nephrology and Transplantation, U.K.
[PP-231] Role of PD in the Treatment of Refractory Ascites and Renal Failure in Non Hodgkin Lymphoma
We present a case of a 57-year-old Caucasian man with low-grade centrocytic centroblastic non Hodgkin lymphoma. He had received various types of chemotherapy but had substantially resistant disease with widespread lymph node involvement and recurrent lymphatic pleural effusion and ascites. He had already undergone pleurodesis and had an indwelling Tenckhoff catheter for simple peritoneal drainage. However, he had no proper aseptic care.
He developed methicillin-susceptible Staphylococcus aureus sepsis from purulent peritonitis, complicated with fluid overload and acute renal failure. A catheter extension was adapted, and he was started on manual exchanges and intraperitoneal antibiotics. Infection and fluid overload resolved, but he recovered renal function only slowly. He was educated to aseptically perform manual peritoneal dialysis.
He has now recovered renal function, and his ascites is controlled with instillation and immediate drainage of peritoneal dialysis fluid with no dwells. The ascitic fluid is now clear and has lost its “milky” look. Nutrition status and anemia are also improved.
In this case, the use of a closed circuit and peritoneal dialysate for ascites drainage was shown to be a successful option and should be considered in similar situations.
Aires I., Lobos A.V., Rodrigues V., Ferreira C., Picado B., Santos J.R., Hosp. Curry Cabral, Lisbon, Portugal.
[PP-232] Assisted Automated Peritoneal Dialysis
We have introduced a novel assisted automated peritoneal dialysis (aAPD) program to our unit. The objective is to maintain patients on their preferred modality—automated peritoneal dialysis (APD)—for as long as possible in their own home even if they are unable to be independent or perform self-care dialysis, thus enhancing the patient's quality of life and possibly increasing peritoneal dialysis numbers. These unaided patients would otherwise be transferred to hemodialysis. A secondary effect may be a decrease in hemodialysis congestion.
Discussions took place with our dialysis suppliers and an external nursing agency to provide help and support to these patients on a daily basis. The nurse visits, strips the cycler from the night before, documents machine readings, checks the clarity of the peritoneal dialysis effluent, and sets the machine again after checking the patient's weight and blood pressure. If necessary, the nurse can alter the machine program after relaying information back to the unit. In addition, the nurse can re-dress the catheter exit site, reporting any abnormalities immediately. The agency nurses are trained by our dialysis training nurses and are assessed by them annually.
We drew up a patient criteria list considering hemodialysis patients, pre-dialysis, peritoneal dialysis, and the acute setting. The first patients commenced aAPD in August 2007. Our short term experience was audited at the end of December 2007, and 7 patients are on the new modality: 1 patient directly from pre-dialysis, 1 patient from hemodialysis, and 5 patients who were already on peritoneal dialysis. The aAPD modality is already proving its worth; all 7 patients would otherwise have transferred to hemodialysis.
The next steps are to promote this modality at our main hemodialysis and satellite units, and as an option for acute or chronic scenarios and for a dip-in and -out service for carers needing respite care, and to audit the effects.
Denning J., Woodrow G., The Leeds Teaching Hospitals NHS Trust, U.K.
[PP-233] Peritoneal Dialysis: Senegalese Pilot Experience in West Africa
Peritoneal dialysis (PD) is a complementary technique to hemodialysis in renal replacement therapy for end-stage renal disease (ESRD). It was not used yet for that indication in west Africa because of the technical difficulties and concerns about the peritonitis.
Results: Our pilot experience from March 2004 to March 2007 includes all ESRD patients treated with PD [n=26; 14 men, 12 women; mean age: 48 years (range: 16–79 years)]. Initial nephropathy was nephroangiosclerosis in 8 cases, diabetic nephropathy in 6 cases, chronic glomerulonephritis in 4 cases, postpartum acute renal failure in 1 case, polycystic kidney in 1 case, and undetermined cause in 6 cases. Patients were autonomous in 77% of cases at the beginning of PD.
Over the last 12 months, continuous ambulatory PD (CAPD) was prescribed in 74% of cases and automated PD (APD) in 26% of cases. We have observed 25 cases of peritonitis since program start. The rate of peritonitis is 23 months x patients / peritonitis since the beginning of the experience, and 31 months x patients / peritonitis during the last 12 months. Outcome of peritonitis was favorable in all cases, except 1 episode resulting from Pseudomonas aeruginosa which involved fatal septic shock and 1 episode resulting from Candida albicans which justified catheter ablation and transfer to hemodialysis. We recorded 6 deaths (23%), 2 related to PD peritonitis.
Conclusions: PD is a perfectly realizable technique of renal replacement therapy in West Africa, however it requires support from the authorities for its development.
Abdou N., Moustapha C.M., El Hadji K.F., Marème D.K., Boucar D., Service de Néphrologie, CHU A. Le Dantec, Dakar, Sénégal.
[PP-234] Encapsulating Peritoneal Sclerosis: Tamoxifen Efficacy in Three Severe Cases
Encapsulating peritoneal sclerosis (EPS) is a rare but extremely serious complication of peritoneal dialysis (PD). There is no established medical treatment, and surgery has been reported with variable success. Since the first case reported in 1999, a benefit for tamoxifen in the treatment of EPS has been suggested, and other cases of successful treatment have been described.
Among 110 patients treated in our PD unit since 1993, we identified 4 cases of EPS.
A 50-year-old woman on continuous ambulatory PD (CAPD) for 7 years developed partial small-bowel obstruction (SBO) and a diagnosis of EPS was made at surgery. She had recurrent partial SBO, which became complete 10 months later. Surgery was performed, but she died from ongoing sepsis.
An African woman 20 years of age developed SBO after 5 years on PD. She underwent laparotomy, and adhesions were lysed. This patient was switched to hemodialysis and received steroids and tamoxifen (discontinued for hepatic toxicity). In January 2003, she had recurrent SBO. Tamoxifen was recommenced, and steady improvement with no further bowel obstruction was seen.
A 41-year-old man on PD for 5 years presented in November 2004 with impaired peritoneal ultrafiltration (UF). A computed tomography (CT) scan demonstrated adhesions and loculated collection. A renal transplant was performed in December 2004. In October 2006, he presented with SBO. Laparotomy revealed thick opaque visceral peritoneum. He developed sepsis related to bowel perforation. This patient started treatment with tamoxifen and currently remains free of symptoms. He developed femoral thrombosis during tamoxifen treatment.
A 40-year-old woman on PD for 8 years presented with UF failure and was switched to hemodialysis. She later presented with fever, refractory hemorrhagic ascites, complete intolerance to oral intake, and cachexia. A CT scan revealed sclerosing peritonitis. Treatment with prednisone and tamoxifen was commenced. Her gastrointestinal symptoms, and nutrition improved markedly.
In our experience, tamoxifen has been effective in EPS, even in severe and advanced cases.
Santos L.1, Mateus A.2, Ramos A.2, Ponce P.2, Dept. of Nephrol.,1 Hosp. Rainha Sta Isabel, Torres Novas, and Dept. of Nephrol.,2 Hosp. Garcia de Orta, Portugal.
[PP-235] Comparison of Hemodialysis and Peritoneal Dialysis— Analysis and Interpretation of Cost Data
Background: Limited funds and a growing population with end-stage renal disease (ESRD) affect health care systems in many countries. Cost analysis of various dialysis modalities mostly lack hospitalization rates and an exact balance sheet analysis and are therefore not directly comparable.
Objectives: To compare and interpret the complete costs for hemodialysis (HD) and peritoneal dialysis (PD), including overhead costs for treatment of complications and for the hospital itself.
Methods: Files of 60 random ESRD patients who had been on dialysis for more than 18 months were retrospectively studied, and all consumption of health care resources was recorded. These resources include costs for medication [including, as a separate group, costs for erythropoietin-stimulating agents (ESAs)], transportation, materials, technical services, overhead costs, ancillary personal costs, costs for radiology and laboratory tests as recorded in an absorption costing for the dialysis department in a large hospital in Austria.
Results: Total costs per patient–year ranged between €94 100 and €48 100 for HD and between €26 900 and €65 800 for PD. The average annual cost per patient was €62 870 for HD and €41 460 for PD:
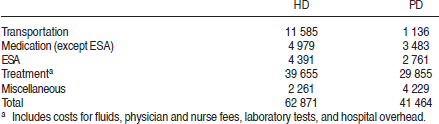
Includes costs for fluids, physician and nurse fees, laboratory tests, and hospital overhead.
Conclusions: Our study evaluated the total costs for two different treatment modalities for ESRD in Austria, including a detailed analysis of the absorption costing of a single dialysis center. This is—to our knowledge—the first study in which this accuracy of measurement has been achieved. As compared with HD, CAPD is associated with strikingly lower absolute costs (75:25 ratio for HD vs. PD for years 1–5). Costs for transportation, laboratory tests, ESAs, and overhead are much lower for PD treatment. The study shows a possible cost benefit for the healthcare system when enhancing the ratio HD versus PD towards PD.
Schuster K., Ärztliche Direktion, Landesklinikum St. Pölten, St. Pölten, Austria.
[PP-236] Can Prediction of Encapsulating Peritoneal Sclerosis be Improved by CT Scanning and Measurement of Dialysate Cytokines?
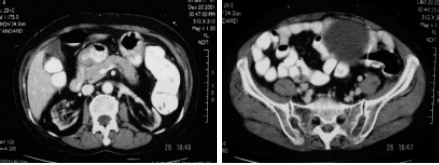
Objectives: Reliable screening tools for encapsulating peritoneal sclerosis (EPS) need to be developed so that patients (pts) can receive appropriate advice about risks and benefits of remaining on long-term peritoneal dialysis (PD). In a prospective study, we measured dialysate interleukin-6 (IL-6), and we developed a diagnostic (Dx) abdominal computed tomography (CT) score.
Methods: We matched 12 PD pts who had EPS with 12 control PD pts who underwent a CT scan for screening or other clinical reasons. Dialysate IL-6 had been measured in all pts; serial IL-6 levels over 3 years had been measured in 7 pts from each group.
Results: Mean time on PD was 7.5 years (range: 4.2–11.9 years) for the EPS group and 3.5 years (range: 0.4–7.3 years) for the control group. PD parameters were available for all pts:

Dialysate IL-6 was significantly higher in the EPS group (114.6±25.1 ng/4 h vs. 45±16.2 ng/ 4 h, p=0.02). Mean Dx CT score was 9.1 (range: 2–16). Mean control CT score was 1.1 (range: 0–4). Pre-Dx CT scans were available in 8 pts; 5 done 5–21 months before Dx scored in the 0–2 range; 3 done 0.5–27 months before Dx scored in the 7–9 range. No pt was symptomatic for EPS at pre-Dx scan:
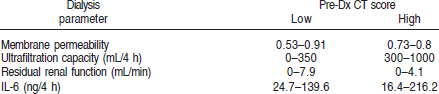
Conclusions: This preliminary study suggests that CT is not a useful tool for predicting development of EPS. As with other studies, many (but not all) pts who develop EPS have high dialysate-to-plasma (D/P) creatinine, low ultrafiltration, and loss of residual renal function. Measurement of dialysate cytokine production may enhance prediction from those parameters, but needs to be confirmed in a larger prospective study.
Ahmad S.1, Tarzi R.M.1, Lim A.2, Moser S.2, Gedroyc W.2, Tam F.W.1, Brown E.A.1, Imperial College Kidney and Transplant Inst.,1 and Dept. of Radiology,2 Imperial College Healthcare NHS Trust, Hammersmith Hosp., London, U.K.
[PP-237] Thyroid Hormone is Linked to Micro-inflammation, Obesity, Cardiovascular Disease in PD Patients
Objectives: Peritoneal dialysis (PD) patients frequently display low T3 levels as an effect of impaired extra-thyroidal T4-to-T3 conversion, or as a phenomenon secondary to peritoneal loss of thyroid-binding globulin. Low T3 syndrome is a strong predictor of death in cardiac patients and might be directly implicated in the poor prognosis of cardiac patients. The purpose of the present study was to evaluate the relationship between thyroid hormone and micro-inflammation, cardiovascular disease (CVD), and obesity in PD patients.
Methods: We allocated 30 PD patients without thyroid disease (15 men, 15 women; mean age: 54.0±10.7 years; PD duration: 32.1±32.3 months) to 1 of 2 groups according to obesity [non obese: body mass index (BMI)<25 kg/m2; obese; BMI≥25 kg/m2] and also to 2 groups according to presence of CVD. The thyroid function profile was determined by measuring T4, T3, FT4, FT3, and thyroid-stimulating hormone (TSH). Biochemical parameters were determined by measuring C-reactive protein (CRP), total CO2 (tCO2), lipid profile, albumin, and Kt/V.
Results: Causes of renal failure were hypertension (43.3%), diabetes (30%), glomerulonephritis (16.7%), unknown (10%). Mean Kt/V was 1.9±0.4, and BMI, 22.7±3.6 kg/m2. FT3 was significantly positively correlated with tCO2 and negatively correlated with CRP (p<0.05). Also, FT3 in the CVD group (2.5±0.4 pg/dL, n=14) was significantly lower than in the non CVD group (2.8±0.4 pg/dL, n=16, p<0.05). FT4 in the obese group (1.2±0.2 ng/dL, n=9) was significantly lower than in the non obese group (1.1±0.1 ng/dL, n=21, p<0.05).
Conclusions: We suggest that low FT3 may be associated with micro-inflammation and cardiovascular disease. Also, low FT4 may be associated with obesity. Further large studies are needed whether low FT3 and FT4 may be associated with cardiovascular disease, micro-inflammation, and nutrition, with the aim of preventing complications of peritoneal dialysis.
Kim H., Lee S., Son M., Kim J., Yang D., Dept. of Internal Medicine, Pochon CHA Univer., Sungnam, Korea.
[PP-238] the Development of a Model of Care for Patients with Advanced Chronic Kidney Disease
Background: Patient numbers in our pre-dialysis service have grown from 122 in 2002 to 505 in 2007, of which 45% have CKD stage 4 and 55% have CKD stage 5. The renal National Service Framework advocates the need for patient education, informed choice, timely preparation, and insertion of access for dialysis treatment.
Methods: We introduced new-patient referral clinics (6/month). Criteria for referral is based on an estimated glomerular filtration rate (eGFR) of 20 mL/min with progressive decline of renal function. At each clinic, 4 patients are seen by an associate specialist, a pre-dialysis nurse specialist, and a dietician. The purpose of the clinic is to initiate specific education concerning the patient's renal disease and treatment choices, to do medical assessment, to expedite referral for transplant work-up where appropriate, and to provide dietetic input. Patients are then routinely followed at pre-dialysis follow-up clinics (6/month), where ongoing education is provided regarding treatment choices, renal disease is monitored so as to stabilize or slow the decline in renal function, and continuing access to the dietician and other renal multidisciplinary team members is provided. For patients whose dialysis is pending referral, access is expedited in accordance with our dialysis access pathway. Patients opting for conservative management are referred into our renal palliative care clinic.
Results: This new model of care is continuously audited to record new referrals to the service. Audit is also ongoing in the 505 patients attending our follow-up clinics, examining and investigating timely decision-making, timely referral and organization of dialysis access, and choices of modes of therapy. These data will allow us to monitor progress with respect to national guidelines.
Conclusions: Clinical approaches for monitoring, supporting, educating, and coordinating patients in CKD stages 4 and 5 vary. We have developed a highly specialized and structured pathway that accommodates patient needs at specific times through their renal disease trajectory.
Heatley S.A., Hirst G., Alcock F., Williamson C., Odonnell J., Summers A., Central Manchester and Manchester Childrens Univer. Hospitals Trust, U.K.
[PP-239] Clinical Achievements in Patients Participating in the BRAZPD Study Using the Spanish Recommendations for PD
Background: The Sociedad Española de Nefrología (SENEFRO) has established clinical targets for patients (pts) on dialysis. Knowing the proportion of pts who reach targets proposed in the guidelines is important in evaluating the quality of treatment and difficulties in achieving goals.
Objectives: Evaluate the proportion of pts who satisfied SENEFRO guidelines in a cohort of pts on peritoneal dialysis [PD (BRAZPD)].
Methods: The BRAZPD is a multicenter prospective cohort study that started in December 2004. All incident and prevalent pts who spent more than 3 months on PD were followed until February 2007.
Results: The study included 3226 pts on automated PD (APD) and continuous ambulatory PD (CAPD), of whom 2094 were incident pts with an average follow-up was 13.6 months. Mean age was 54±19 years, 52% were women, and 64% were Caucasian. Diabetes mellitus (36%) was the most frequent cause of chronic kidney disease. Target blood pressure was reached in 70% of pts. The prevalence of peritonitis was 1 episode in 30 pt–months. Peritonitis with negative culture was observed in 40%, and the cure rate was 87%. The goal for hemoglobin (Hb) was achieved in 49%. Goals for Ca, P, and CaxP were achieved in 62%, 30%, 79% respectively. Albumin was on target in 66%. The goals were most difficult to accomplish in diabetic pts. The targeted Hb level was the most difficult to reach, mainly in those who did not received pre-dialytic care (p<0.005). Drop-out was 33%, mainly because of death (52%), and cardiovascular diseases were the most prevalent cause of death (40%). Incident and prevalent pts presented survivals of 72% and 75% respectively.
Conclusions: From these data, we conclude that the quality of PD in Brazil is in consonance with the parameters established internationally.
Fernandes N.M.1, Bastos M.G.1, Pereira L.C.2, Franco M.G.2, Haddad S.A.3, Pinheiro M.T.4, Faifer T.M.4, Visona A.P.5, Tavares E.F.6, Caramori J.7, Silva E.C.8, Carvallo R.B.9, Divino–Filho J.C.10, Pecoits–Filho R.11, Dept. Nephrol. and Imepen Foundation,1 Fed. Univer., Juiz de Fora; Gamen,2 Rio de Janeiro; Ourinhos,3 Bauru Hosp. Assoc.,4 and Votuporanga,5; Sao Paulo; Unirim– Recife,6 Pernambuco; Famesp,7; Sao Paulo; Renal Clin.,8 Pernambuco; Assis,9 Sao Paulo, Brazil; 10Baxter Healthcare; and 11BRAZPD Group.
[PP-240] Carcinoma of Ovary with Tenckhoff Catheter Tunnel Metastasis—A Case Report and Review of the Literature
The frequency of abdominal malignancy among end-stage renal disease (ESRD) patients treated with peritoneal dialysis (PD) is not well addressed. Chances are higher, especially for malignancies arising from the urinary and genital tract. Some of these cases present late with distant metastasis, but metastasis along the Tenckhoff catheter has not previously been reported.
A Chinese woman with ESRD treated with continuous ambulatory PD (CAPD) for 2 years presented to us with a rapidly enlarging tunnel swelling over the Tenckhoff catheter. Subsequent computerized tomogram of the abdomen confirmed the presence of an adnexal mass.
Fine-needle aspiration confirmed mucinous type of cystadenocarcinoma. Her PD was well performed, and the dialysis effluent remained clear. She refused intervention and finally died 2 years later. Literature review and discussion of the incidence of abdominal malignancy in ESRD patients on CAPD follows.
Chak W., Wong H., Choi K., Chan Y., Chau K., Li C., Dept. of Medicine, Renal Unit, Queen Elizabeth Hosp.
[PP-241] Enhancing Care in PD Using Telecare—The Singapore General Hospital Experience
Background: With recent advances in telecommunications technology in the health care sector, we recruited peritoneal dialysis (PD) patients (pts) for telecare monitoring (MyTelecare) as par t of an initiative to enhance health care.
Objectives: To enhance monitoring of PD treatment, and to identify problems early and institute prompt measures.
Methods: We recruited 19 pts (age: 20–75 years; 11 men, 8 women) to use the MyTelecare system. Study period was 18 months. Pts logged in to send information using the MyTelecare Internet portal or a mobile phone (SMS). Parameters monitored were temperature, blood pressure (BP), blood glucose, weight, ultrafiltration, flow time, exit site, and effluent status. Internet data entry was accompanied by a customized symptoms questionnaire. Monitored parameters were assigned ranges with preset auto-alarms tailored to the individual pt. For abnormalities requiring prompt response, an SMS alert message was sent to the physician for acknowledgment; appropriate action was returned using SMS. For less urgent problems, physicians logged in at the MyTelecare portal to view pt charts, symptom questionnaires, and answers to queries.
Results: A total of 563 entries were registered, of which 287 (51%) triggered an alert to physician: 14.6% of those alerts warranted a prompt SMS response (5.5% exit-site problems, 5.3% lower-limb swelling, 3.8% cloudy effluent). Another 14% required an early reply through the portal system. In 6 cases of uncontrolled hypertension, medications were titrated using MyTelecare. All exit-site infections were treated successfully as outpatient cases. Only 1 case of peritonitis required inpatient management. A pt survey revealed satisfaction with the system, finding it useful, easily accessible worldwide, and user friendly. Pts were more motivated; the system empowered them with regard to their treatment.
Conclusions: Telecare monitoring and prompt action, taken early, for problems encountered can potentially reduce hospital visits, thus reducing overall cost to pts. This enhancement in PD monitoring and treatment will in the long-term improve the technique and pt survival.
Tan R.1, Lim F.S.2, Wong K.S.1, Foo M.1, Dept. of Renal Medicine,1 Singapore General Hosp., and ITAG/Info Tech,2 SingHealth, Singapore.
[PP-242] Successful Conservative Management of Scrotal Edema Resulting from Uncomplicated Peritoneal Fluid Leak: Case Report
Peritoneal fluid leaks are frequent in continuous ambulatory peritoneal dialysis (CAPD) patients and may manifest as subcutaneous or genital edema or apparent ultrafiltration (UF) failure. If imaging studies exclude an associated hernia or patent processus vaginalis, a conservative approach to management may be adopted. Here we present a case of gross dialysate leak resulting both in bilateral scrotal edema and in apparent UF failure without an associated hernia or detectable peritoneal defect.
Case Report: An 80-year-old bedridden man with kidney failure, hypertension, and ischemic heart disease developed gross bilateral scrotal swelling with no cough impulse, associated with apparent UF failure shortly after initiation of CAPD. Computed tomography peritoneography (CTP) showed bilateral scrotal fluid collections without a hernia or patent processus vaginalis. An attempt to maintain the patient on CAPD by reduction in the dialysate volume, scrotal elevation, and adoption of a supine position was not successful; CAPD was substituted with temporary hemodialysis for 4 weeks. The subsequent reversal of scrotal swelling after 1 week of CAPD cessation was compatible with caudal fluid dissection through the soft tissues being the cause of this patient's problem.
After 4 weeks, CAPD was reinstituted with intermittent dry periods; the scrotal swelling did not recur, and satisfactory UF could be easily attained. The patient has been successfully maintained on CAPD for the last 16 months.
Conclusions: Fluid dissection through soft tissues can result in gross genital edema and apparent UF failure in CAPD patients. The severity of dialysate leak does not preclude a satisfactory response to conservative management, allowing for reinstitution of CAPD after a rest period. CAPD with intermittent dry periods may be a practical option for managing uncomplicated scrotal edema, such as this case, in the absence of automated dialysis facilities.
Mubarak A.I., Abu-Aisha H., Sudan National Peritoneal Dialysis Program.
[PP-243] Prevalence and Severity of Restless Legs Syndrome in Dialysis Patients
Objectives: Restless legs syndrome (RLS) is common in dialysis patients (pts). We investigated the frequency and severity of RLS, which has a negative effect on quality of life and is accompanied by increased mortality in dialysis.
Methods: A questionnaire including the minimum criteria of the International Restless Legs Syndrome Study Group (IRLSSG) was administered to 48 hemodialysis (HD) pts and 43 peritoneal dialysis (PD) pts. A neurologist evaluated all pts for a clinical diagnosis of RLS. The severity of RLS was determined by the IRLSSG Severity Scale.
Results: RLS was diagnosed in 28 (12 HD, 16 PD) of 91 dialysis pts (48 HD, 43 PD). The RLS rate was 25% in HD pts and 37.2% in PD pts. However, those percentages and the severity of RLS were not significantly different between the groups:
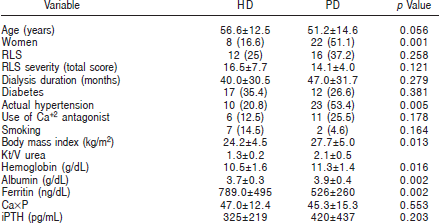
All data mean ± standard deviation, and unpaired t-test for comparisons; or number (percentage), and chi-square test for comparisons. iPTH = intact parathyroid hormone.
RLS was positively correlated with body mass index [BMI (r=0.260)] and actual hypertension (r=0.290). Both parameters were also found independent predictors of RLS. Severity of RLS was significantly associated with age and serum ferritin level, which were independent predictors of RLS severity.
Conclusions: Dialysis modality has no effects on prevalence and severity of RLS. In the presence of RLS, correctable factors associated with RLS, such as BMI, hypertension, and ferritin should be considered.
Yuksel S.1, Yilmaz M.2, Demir M.1, Erturk J.3, Koyuncuoglu H.R.2, Sezer M.T.1, Dept. Nephrology1 and Dept. Neurology,2 Suleyman Demirel Univer. Med. Faculty, and Dialysis Unit,3 Hosp. of Suleyman Demirel Univer., Turkey.
[PP-244] Assessment of Compliance and Retraining Needs in PD Patients
Objectives: To evaluate the theoretical knowledge that the patients retained from initial peritoneal dialysis (PD) training; to perform a PD retraining program; and to evaluate the efficacy of a PD re-training program on patient outcomes.
Methods: We evaluated 52 patients (26 men, 26 women; mean age: 54 years), who had been on PD for at least 6 months (mean: 37±14 months). The cognitive investigation used a questionnaire containing 30 queries assessing patient knowledge about PD, diet, drugs, infections (peritonitis, exit site), and physical activity. An 80% cut-off for correct answers was taken as a reference point for evaluating retraining needs.
In January 2008, retraining started. It consisted of brief sessions with the patient, aimed at reviewing parts of training that had been forgotten. We used educational materials provided by Baxter Healthcare. The third phase of this study, currently in progress, will evaluate the efficacy of the retraining program on patient outcomes, particularly in preventing episodes of peritonitis.
Results: In patient questionnaires 71% of answers were correct, 15% were incomplete, and 11% were incorrect (3% missing data). Data collected during the re-training program showed that 20% of patients were noncompliant with the exchange procedure, and 16% were noncompliant with the exit-site procedures. Regarding medications, 80% of patients were found totally compliant. Evaluation of the PD re-training program is in progress. All data will be available in June 2008.
Conclusions: Over time, because of the chronic nature of kidney failure and dialysis therapy, patients tend to forget or modify the information received at the beginning of their dialysis treatment. Based on our results, we recommend routine performance of an evaluation of re-training needs and activation of structured PD re-training programs.
Russo R.1, Corciulo R.1, Valicenti E.1, Paris V.2, Dept. of Nephrology,1 Univer. of Bari, and Baxter SpA,2 Roma, Italy.
[PP-245] Bridging the Gap: Pre-planned Education about Home Dialysis
Despite evidence in the literature that demonstrates that home dialysis is more convenient and improves quality of life, many patients in the province of Ontario are started and maintained on hospital-based dialysis therapies. Ontario's Ministry of Health and Long Term Care (MoHLTC) has set provincial targets for dialysis modality distribution that all dialysis programs are expected to achieve by 2010: 60% in-center hemodialysis (HD), 30% home peritoneal dialysis (PD), and 10% home HD.
Progressing toward meeting those targets, a patient education program was developed by Home Dialysis staff, followed by a Home Dialysis Liaison role to inform in-center HD patients about alternative treatment options, with the intention of encouraging clinically suitable patients to migrate from in-center HD to home PD. The study evaluated the effectiveness of the education program, and captured the patients’ perception of home dialysis which affected transfer to PD.
All clinically suitable patients (approximately 150) were included in the study sample. Subjects received education on PD by a home dialysis nurse. Baseline data were collected on demographics, living arrangements, pre-dialysis treatment, and awareness of alternative care options. Responsiveness to the education was measured and correlated with patient characteristics. Following initial contact, 37 in-center HD patients received the full education program, with 4 transferring to PD, and 3 to home HD. The Home Dialysis Liaison nurse saw gave modality education to 10 patients; 3 of those chose PD.
Kashani M., Home Dialysis Unit, St. Michael's Hosp., Ontario, Canada.
[PP-246] Strategies to Maximize PD Utilization in the “MINT” Countries
The Asian continent has been showing the highest numeric growth in peritoneal dialysis (PD), although PD penetration is still low in most countries in the region. Many countries have had significant economic growth and better health care affordability in the past decade. However, PD utilization rates have not improved as might have been expected, but hemodialysis has grown exponentially. That differential has been especially true of Malaysia, the Indian subcontinent, and Thailand (the “MINT” countries), which share certain issues and have a few unique ones, which are emerging as bottlenecks to a more sustained growth of PD as an option for renal replacement therapy. The PD community needs to address these issues, most of which are misplaced perceptions in the minds of the practicing nephrologists, health care providers, and the patient population at large.
Nayak K.1, Sirivongs D.2, Dept. of Nephrology,1 Global Hosp., Hyderabad, India, and Div. of Nephrology,2 Khon Kaen Medical School, Khon Kaen, Thailand.
[PP-247] the Effects of Previous Intraperitoneal Adhesions on the Outcome of Peritoneal Dialysis Catheters
Background: Peritoneal dialysis (PD) in patients with the history of previous abdominal surgery is doubtful because of the presence of intraperitoneal adhesions. The purpose of the present study was to compare outcome of PD catheters inserted using a laparoscopic technique in patients with and without intraperitoneal adhesions.
Methods: A data bank of patients who underwent laparoscopic implantation of a PD catheter from March 2004 to June 2007 was reviewed. Follow-up was 1–36 months (mean: 14.6 months). Overall and revision-free survival of catheters was estimated using the Kaplan–Meier method.
Results: In 169 patients, 180 consecutive laparoscopic procedures resulted in 179 successful catheter implantations. One patient with extensive adhesions could not be implanted. In 85 of the 179 procedures (47%), a history of previous abdominal surgery was present, but only 23 (27%) of the patients had intraperitoneal adhesions. Intraperitoneal adhesions were present in 4 patients without a history of previous abdominal surgery. The final comparison was done for two groups, 27 patients with and 152 patients without intraperitoneal adhesions. The two groups showed no significant difference in 1- and 2-year overall and revision-free survival of catheters, in rates of mechanical and infectious complications, and in the surgical revision rate.
Conclusions: There was no significant difference in the outcomes of PD catheters in patients with and without intraperitoneal adhesions. Laparoscopy is the only way to diagnose and treat intraperitoneal adhesions, and it is the best technique of implantation of PD catheters in patients with history of previous abdominal surgery.
Keshvari A.1, Najafi I.2, Nouritaromlu M.1, Dept. of Surgery1 and Dept. of Nephrology,2 Tehran University of Medical Sciences, Iran.
[PP-248] Nephrogenic Fibrosing Dermopathy–Nephrogenic Systemic Fibrosis: Literature Review Based on a Re-evaluation of a Case
Recently, the Spanish Medicine and Sanitary Products Agency sent an alert about the use of contrast containing gadolinium in patients with end-stage renal disease (ESRD) and the appearance of nephrogenic fibrosing dermopathy (NFD)/nephrogenic systemic fibrosis (NSF), a rare disease of excessive formation of connective tissue, leading to fibrosis and thickening of the skin either locally or systemically.
Case Report: Four months following a cholangiogram with gadolinium, a 75-year-old woman on peritoneal dialysis (PD) developed fibrosis and cutaneous thickening causing severe contracture of her limbs. She was initially diagnosed with Buschke scleroderma and was therefore treated with high doses of penicillin, which proved ineffective for her condition. The diagnosis of NFD/NSF was confirmed on skin biopsy. A literature review was undertaken, which described some possible contributing factors for NFD, such as exposure to some form of invasive vascular procedure or thrombosis (she had had an arteriogram and an arteriovenous fistula thrombosis). Clinically, she did not present with any systemic involvement, and her skin partly improved after administration of pentoxifylline, which has been reported as a possible treatment.
Conclusions: Potentially, there are patients with ESRD and skin disease diagnosed as another dermatologic entity. It is important to re-evaluate those cases to make a certain diagnosis, because NFD/ NSF can become a very incapacitating disease. It is also important to evaluate the benefits and risks of image studies using gadolinium contrast in patients with ESRD.
Sujan S., Montero L., Ros S., Torres A., Trujillo C., Hosp. Carlos Haya, Málaga, Spain.
[PP-249] Chylous Ascites: Is Secondary Amyloidosis a Possible Cause? Literature Review Based on a Case Presentation
Chylous ascites is milky discoloration of the peritoneal fluid because of elevated triglyceride content or the presence of chylomicrons. In the absence of peritonitis, this condition is the result of disruption of the abdominal lymphatic system in patients on peritoneal dialysis, the most common cause being trauma during Tenckhoff catheter insertion. Other possible causes are malignancy, cirrhosis, and inflammatory and infectious conditions, but a relationship with primary amyloidosis has also been described.
Case Report: A 21-year-old woman with chronic kidney disease secondary to AA amyloid from juvenile rheumatoid arthritis was indicated for renal replacement therapy because of the progressive decline of her renal function. She was admitted for peritoneal catheter placement. During the procedure, before the catheter insertion and without any trauma, she presented with chylous ascites. She was thoroughly investigated to exclude malignancy or other inflammatory or infectious diseases that cause chyloperitoneum, with no findings. We conclude that AA amyloidosis is another possible cause of chylous ascites not yet described in literature.
Sujan S., Ros S., Cobelo C., Trujillo C., Carlos Haya Hosp., Málaga, Spain.
[PP-250] Nurse-Prescribing Improving the Patient Experience
Objectives: To provide a seamless care pathway in managing the prescription needs of patients, to reduce waiting times for prescriptions, and hence to improve the experience of patients attending nurse-led clinics. I therefore enrolled in the nurse-prescribing course at the local university in September 2005. During that 6-month course, I sat written and oral exams and also produced a substantial portfolio demonstrating my competence and understanding as a prescriber. I was fortunate to have a renal SpR mentor who educated and supported me in my working field while I was training.
I completed the course, successfully passed the exams, and registered with the nursing council to practice. Having had numerous discussions about my scope of practice with my manager, lead clinician, and pharmacist (I was the first renal nurse in our Trust to prescribe), I was ready to start prescribing. I commenced in November 2006. I qualified as an independent nurse prescriber and a supplementary prescriber. Independent prescribing suited my practice, and therefore that method is the only one I use now. I audited my prescribing practice every 3 months, initially expanding the range of drugs I felt confident to prescribe as time went on:

The medications I now prescribe enable us, as a nurse-led team to deal with the prescription needs of patients without having to signal and wait for a doctor. The patients are informed that I will be prescribing and are happy for me to do so. They feel that this approach has had a great impact on their treatment satisfaction, and doctors look upon me as an equal in the prescribing field and appreciate how the teamwork lightens their workload.
Denning J., Leeds Teaching Hospitals NHS Trust, U.K.
[PP-251] Post-Hysteroscopy Polymicrobial Peritonitis in a Woman Receiving CAPD
We report the first case of post-hysteroscopy polymicrobial peritonitis in a female continuous ambulatory peritoneal dialysis (CAPD) patient 1 day after hysteroscopy for menorrhagia. Peritoneal fluid culture grew multiple organisms, including group B Streptococcus, methicillin-sensitive Staphylococcus aureus, and Escherichia coli. It is suspected that the vaginal flora were carried retrograde into the peritoneal cavity in the distension medium via a possible vaginoperitoneal communication. The patient developed septicemic shock, resulting in admission to the intensive care unit. Tenckhoff catheter removal was subsequently required despite appropriate administration of intraperitoneal and intravenous antibiotics. The use of prophylactic antibiotics in CAPD patients undergoing gynecologic procedures is recommended.
Yap D.Y., Tse K., Lam M., Chan D.T., Lai K., Dept. of Medicine, Queen Mary Hosp., The Univer. of Hong Kong, Hong Kong SAR, PR China.
[PP-252] Encapsulating Peritoneal Sclerosis following Renal Transplantation despite Tamoxifen and Immunosuppressive Therapy
Background: Encapsulating peritoneal sclerosis (EPS) is a rare and often fatal condition occurring in patients who have undergone peritoneal dialysis (PD). Recently there have been reports of EPS occurring post transplantation. Here we report a case of EPS in a renal transplant recipient despite prophylactic treatment with tamoxifen and immunosuppression.
Case Report: In a man receiving PD for end-stage renal failure of unknown cause, an initial diagnosis of EPS was made following the surgical and pathologic findings of adhesions and peritoneal fibrosis with inflammation at the time of cholecystectomy. Computed tomography (CT) imaging at that time and later, before renal transplantation, did not demonstrate evidence of EPS. This patient chose to remain on PD for lifestyle reasons and commenced on tamoxifen to prevent further deterioration of the peritoneal membrane. Treatment continued despite transplantation, but failed to prevent ensuing subacute bowel obstruction post transplant. A peritonectomy was performed, but symptoms persisted, and a repeat peritonectomy was performed 6 months later. At that time, the patient was still receiving tamoxifen and immunosuppression and not undergoing PD.
Conclusions: This report highlights some important clinical issues regarding diagnosis, treatment, and management of EPS. It questions the value of CT as a screening tool. Also, the EPS developed and reoccurred despite tamoxifen and immunosuppressive therapy. It is possible that tamoxifen afforded protection or slowed disease progression until a yet-unidentified trigger at the time of transplantation led to rapid EPS progression. The importance of a high index of clinical suspicion is highlighted by the diagnosis of irritable bowel syndrome (IBS) before transplant. The marked overlap in symptoms between IBS and EPS may cause diagnostic confusion. Familiarity with EPS and a high index of clinical suspicion are important determinants in making the diagnosis, which is an important lesson from this case.
Summers A.M., De Freitas D.G., Hurst H., Taylor P., Dunn L., Williams R., Hutchison A.J., Brenchley P.E., Augustine T., Manchester Inst. of Nephrology and Transplantation, U.K.
[PP-253] Comparative Study of Continuous Venovenous Hemodiafiltration and PD in Critically Ill Acute Renal Failure
Critically ill patients with renal failure were randomly allotted to receive either pump driven continuous venovenous hemodiafiltration [CVVHDF (group A; n=22; mean age: 44.81±14.52 years)] or continuous peritoneal dialysis [PD (group B; n=24; mean age: 46.63±16.67 years)]. The cause and severity of renal failure was assessed by noting the number of organs involved and the Acute Physiology and Chronic Health Evaluation (APACHE) II score. Renal function, electrolytes, and arterial blood gases were analyzed every 6 hours, and urea and creatinine clearances were estimated. The degree and time taken for correction of uremia, acidosis, hyperkalemia, fluid overload, sensorium and hemodynamic disturbance, and the cost and final outcome were studied. Statistical analysis used chi-square, Student t-, modified t-, and Fisher exact test.
Results: The two groups were comparable with regard to age, sex, and causes and severity of renal failure. Group A received 19.24±11.93 hours of dialysis, and group B, 66.33±72.7 hours (p=0.004). Uremic correction was inadequate in 9 in group A and 12 in group B with no significant difference in time to correct. The urea and creatinine clearances were 20.48±8.41 and 18.14±9.14 in group A (p=0.003) and 9.32±5.02 and 10.53±6.22 in group B (p=0.006). Acidosis correction appeared to be better in group B (p=0.028). Fluid correction was significantly faster in group A, with more ultrafiltrate (22.64±17.9 group A vs. 5.76±5.98 group B, p<0.05). No significant difference was seen in correction of hyperkalemia, altered sensorium, or hemodynamic disturbance. Hypotension was more common in group A. There was no significant difference in outcome in the two groups. The cost of disposables was significantly more in group A (Rs6952.33±Rs 1239.65) than in group B (Rs2980±Rs1725.18, p=0.00).
George J., Varma S., Palliyil S., Leelakumari M., Kumar S., Pisharody R., Nephrology, India.
[PP-254] Proteomic Profiling and Identification in Peritoneal Dialysate of Children Treated by PD
Objectives: Proteomic technologies offer high-throughput analysis of protein expression in biologic samples. A first step for proteomics in peritoneal dialysis (PD) is protein profiling and identification for normal dialysate in a well-characterized set-up, to provide a representative overview of the proteins present. Global analysis of the proteins in PD fluid (PDF) will provide a better understanding of the biologic processes of the peritoneal membrane.
Methods: The dialysate of 9 pediatric PD patients was collected from the 2-hour dwell of a peritoneal equilibrium test with 3.86% glucose. Samples were concentrated, purified, and run on a 10% 1D-SDS-PAGE and in-gel digested with trypsin. Afterward, peptides were separated with nanoscale high-performance liquid chromatography on a reversed phase column. Peptide mass and masses of their respective fragment ions were determined by subsequent mass spectrometry (MS) and MS/MS cycles. The MS data files were then searched against the NCBI database using the Mascot search program. Relative protein abundances were calculated as exponentially modified Protein Abundance Index. All samples were measured twice.
Results: Of the 189 proteins identified in the PDF, 88 proteins were common to all 9 samples. These 88 proteins accounted for 47% of the identified proteins, and for more than 90% of the total protein content in the analyzed samples. Extracellular matrix proteins formed a large part of the total proteome in PDF as compared with the plasma proteome. Potentially interesting proteins identified were gelsolin, intelectin, and paraoxonase.
Conclusions: The representative overview provided in this study of the proteins present in PDF can serve as a reference for future proteomic studies in PD. Interesting new proteins in PDF are revealed, with potential meaning for defense against infections and complications of PD.
Raaijmakers R.1, Pluk W.2, Schröder C.3, Gloerich J.2, Cornelissen E.1, Wessels H.4, Willems J.5, Monnens L.1, Heuvel L.V.2, Dept. Paediatr. Nephrol.,1 Radboud Univer. Nijmegen Med. Ctr., and Lab. Paediatr. and Neurol.,2 Nijmegen Proteomics Facility, Radboud Univer. Nijmegen Med. Ctr.; Dept. Paediatr. Nephrol.,3 Univer. Med. Ctr. Utrecht; Nijmegen Ctr. for Mitochondrial Disorders4 and Dept. Clin. Chem.,5 Radboud Univer. Nijmegen Med. Ctr., Netherlands.
[PP-255] Leptin and Adiponectin Relationship with Inflammation in PD Patients
Adipose tissue is the source of many adipokines, such as leptin (LPN) and adiponectin (ADPN), which may not only have endocrine functions, but may also contribute to systemic inflammation. Adipokines serum levels are markedly elevated in chronic kidney disease, probably because of decreased renal excretion.
The aim of the present study was to analyze the relationship between inflammation and serum ADPN and LPN levels in patients treated with peritoneal dialysis (PD).
We studied 28 patients (16 men, 12 women) on PD and 16 healthy controls (4 men, 12 women). We analyzed several clinical, biochemical, and inflammatory parameters. Nutrition status was assessed using Subjective Global Assessment (SGA), protein equivalent of total nitrogen appearance (PNA), and body mass index (BMI). The mean age of the PD patients was 54±18 years. Mean PD duration was 25±20 months. Serum LPN (29.9±28.37 μg/L vs. 7±2.9 μg/L, p=0.001) and ADPN (31.7±23.8 μg/L vs. 9.5±10.3 μg/L, p=0.001) levels were significantly increased in PD patients as compared with controls. Female patients had higher LPN levels than did male patients (44±36 μg/L vs. 19±13.8 μg/L, p=0.03). No significant difference was observed between men and women regarding ADPN levels. In a linear correlation model, we found that high-sensitivity C-reactive protein [hsCRP (r=0.69,p=0.001)] and interleukin-6 [IL-6 (r=0.52,p=0.007)] were positively correlated with LPN levels. Serum ADPN levels correlated inversely with hsCRP (r=0.48, p=0.01). No correlation was found between ADPN and IL-6. A significant negative correlation was observed between serum LPN and ADPN (r=0.44, p=0.02). In our patients, LPN and ADPN were not correlated with residual renal function and nutrition parameters.
This study demonstrated that PD is associated with a marked increased in serum LPN and ADPN levels. Both adipokines are associated with inflammatory markers in our patients; Our results support the hypothesis that adipose tissue may play an important role in chronic inflammation in PD patients.
Pinto I.S., Bernardo I., Carrasqueira H., Faísca M., Laranjo C., Monteiro V., Neves P.L., Nephrology Dept., Faro Hosp., Faro, Portugal.
[PP-256] Endothelial Progenitor Cells as a Marker of Vessel Repair Potential in Patients on PD versus HD
Endothelial progenitor cells (EPCs) are bone marrow–derived adult stem cells participating in vasculogenesis. Circulating EPCs reflect the intensity of endothelial repair. A decreased number of circulating EPCs is a sensitive marker of cardiovascular risk, which is significantly augmented in end-stage renal disease. The present study compared circulating EPCs and factors influencing them in patients on peritoneal dialysis [PD (n=26; age: 59.5±13.5 years) and hemodialysis [HD (n=46; age: 58±16 years)]. Plasma vascular endothelial growth factor (VEGF) and endostatin, with opposite effect on EPC number and function, were also assessed. Results were compared to results in 40 healthy staff members. Circulating EPCs were estimated in whole blood by means of flow cytometry. Early EPCs were identified by the surface marker CD34 and VEGF receptor type 2 (VEGFR2). Late EPCs were identified by CD31 and lack of CD45. VEGF and endostatin were assessed in plasma by colorimetric ELISA.
Early EPCs were insignificantly reduced in PD patients, suggesting potential protective influence of PD over HD on vasculature. In HD patients, a tendency to reduced EPCs was noted. Late EPCs were significantly reduced in PD and HD patients (p=0.0029). In HD patients, significantly lower VEGF was noted, but VEGF was significantly higher in PD patients (p=0.0000). Endostatin levels were significantly higher in patients with end-stage renal disease regardless of dialysis modality (p=0.000).
EPCs are differently affected in PD and HD patients: early EPCs are reduced in HD, and late EPCs are reduced in PD. Plasma endostatin increase may be one of the factors negatively affecting EPC levels.
Watorek E.1, Paprocka M.2, Dus D.2, Kopec W.1, Klinger M.1, Dept. of Nephrology and Transplantation Medicine,1 Wroclaw Medical Univer., and Inst. of Immunology and Experimental Therapy,2 Polish Academy of Science, Wroclaw, Poland.
[PP-257] Reference Patterns: Three Years’ Experience in a Single Center
Background: Late referral to the nephrologist is an important public health problem. Late referral has been related to increased comorbid conditions and increased risk of death.
Objective: To evaluate referral time and comorbid conditions in incident peritoneal dialysis (PD) patients.
Methods: Data were recorded in a prospective cohort study in a single center. Incident PD patients between 1 January 2005 and 31 December 2007 were included. Comorbid conditions were evaluated using the Charlson Comorbidity Index (CCI). Age, sex, cause of end-stage renal disease, residual renal function (RRF), albumin, hemoglobin (Hb), Hto, need for emergency hemodialysis (HD), and nephrologist evaluation at least 2 months before the start of the renal replacement therapy (RRT) were recorded. Early referral was defined as 1st visit to the nephrologist at least 3 months before RRT. Descriptive statistics and univariate analysis of the differences in clinical and laboratory variables between late and early referral were used in the statistical analysis, with t-test for continuous variables and χ2 or Fisher exact test for discrete variables.
Results: We evaluated 127 patients, of whom only 59 (46%) were early referral:
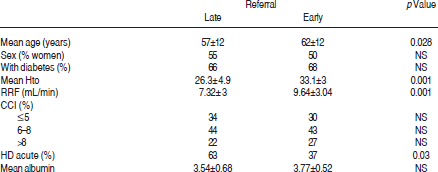
Of these patients, 55% started on continuous ambulatory PD, and 45% on automated PD.
Conclusions: Although access to the nephrologist in our institution is open, referral has been delayed in a important number of patients. These patients need emergency HD more often, and their Hto and RRF are worse than in early-referral patients. There was no difference in comorbidity between the groups. The next step is to evaluate the effect on patient outcomes and to improve referral.
Ramos A., Jusaino C., Leiva F., Perez T., Rivera K., Peritoneal Dialysis Service, Hosp. General de Zona #2, Hermosillo, Mexico.
[PP-258] Kidney Transplantation in a Patient with Previous External Iliac Vein Thrombosis
Background: The main purpose of the present study was to demonstrate that the possibility of kidney transplantation should not be excluded for patients with a history of iliac vein thrombosis.
Methods: We present a 53-year-old man who had undergone bilateral femoral venous catheterization because of recurrent hemoaccess thrombosis. Before the patient was put on the waiting list, several assessments were performed: Doppler ultrasound, computed tomographic (CT) venography, screening for thrombophilia, antiphospholipids antibodies, and lupus anticoagulant.
Results: All of the hematologic tests were negative, and no deep venous thrombosis (DVT) was detected by Doppler ultrasound. However, CT venography discovered a right external iliac vein thrombosis and provided helpful insights into the renal transplantation possibilities. The patient then received treatment with warfarin. International normalized ratio was 2–3. Ten months ago, the patient underwent a kidney transplantation on the site opposite to the DVT. Kidney transplantation was performed without any complications. The postoperative course was uneventful, and plasma creatinine slowly declined to 2 mg/dL at 1 week. At 8 months from transplantation, plasma creatinine was 2.2 mg/dL and warfarin treatment was continuing.
Conclusions: In our opinion, patients with previous diagnosis of iliac vein thrombosis should not be excluded from the waiting list for kidney transplantation, on the condition that accurate assessments have been performed and that anticoagulant treatment has been given.
Scotto P., Galfrè A., Concas G., Murtas S., Bolasco P., Unit of Nephrology and Dialysis, Asl 8, Cagliari, Italy.
[PP-259] Acute Appendicitis in CAPD Patients: Review of 2 Cases
The management of continuous ambulatory peritoneal dialysis (CAPD)–related peritonitis resistant to intraperitoneal (IP) antibiotics is a challenge. In some cases, abdominal (abdo) pathology should be suspected. A diagnosis of surgical abdomen in CAPD-related peritonitis is tough and often delayed.
Case Reports: A 72-year-old woman on CAPD presented with turbid dialysate. Initial dialysate white blood cell count was 1896/mm3, which decreased to 516/mm3 after 2 days of IP cefazolin plus ceftazidime. At day 6, dialysate cell count increased to 9876/mm3. Antibiotic regimen was changed to teicoplanin and piperacillin/tazobactam. Abdo computed tomography scan demonstrated no evidence of abdo lesion. However, abdo pain persisted, and PD catheter was removed at day 8. The patient's abdo pain improved somewhat, but was localized to the right lower quadrant at day 11. Abdo ultrasonography revealed swelling of the appendix. Emergent exploratory laparotomy showed appendix perforation. Bacteroides species was grown at day 6 of dialysate culture. The patient died of pneumonia at day 23.
A 66-year-old man was admitted after no response to 9 days of IP outpatient antibiotic treatment for CAPD peritonitis. He received IP cefazolin plus ceftazidime and missed a follow-up visit. He was admitted for abdo pain aggravation. At admission, physical examination revealed right lower quadrant tenderness. Ultrasonography of the appendix showed diffuse wall thickening.
Appendectomy without PD catheter removal was performed. At 3 weeks after surgery, a trial of PD failed for poor drainage. The patient was transferred to a local hospital with cuffed tunneled catheter.
In CAPD patients with suspected abdo pathology, radiologic study may be negative, and clinical presentation may be atypical. If close monitoring shows no improvement after meticulous radiologic work-up and antibiotic switch, surgical exploration should be considered early.
Kim S., Yang J., Lee H., Lee J., Chung W., Div. of Nephrology, Gil Hosp., Gachon Medical Science Univer., Incheon, Korea.
[PP-260] Moderate Systemic Inflammation is Not Correlated with Increased Vascular Protein Leak in PD Patients
An inverse relationship exists between plasma albumin and inflammatory status as measured by high-sensitivity C-reactive protein (hsCRP) in peritoneal dialysis (PD) patients. It is not clear whether the relationship is the result of increased systemic endothelial protein leak or reduced albumin synthesis.
Methods: In a cross-sectional study, we investigated 27 patients (17 men) established on PD (median: 22.3 months) with average age of 66 years (range: 28–83 years) to determine rates of albumin leakage from the intravascular compartment. After intravenous injection of a standard dose of 125I-labeled human serum albumin (0.185 MBq), plasma samples were collected from a remote site at 10, 20, and 30 minutes. The rate of disappearance from the systemic circulation was calculated from the best linear fit. None of the patients had had peritonitis within 1 month of the study.
Results: Albumin [31.6 g/L (range: 24–42 g/L)] and hsCRP [4.81 (range: 0.6–23.4)] were inversely correlated (r=-0.43, p=0.035). The average rate of albumin loss from the circulation was 6.9±3.7 mL/min. In healthy subjects, the rate of albumin leak from the intravascular compartment is approximately 5%/h; in these PD patients, this leakage was much higher at 14.7%/h. The albumin leak did not correlate with age, plasma albumin, comorbidity, hsCRP, peritoneal transport status, or peritoneal protein losses.
Conclusions: Our findings suggest that there is an increased albumin leak from the intravascular compartment in PD patients, but that the leakage is not an important determinant of plasma albumin. The association between plasma albumin and hsCRP would appear to be predominantly the result of reduced synthesis.
John B., Davies S.J., Dept. of Nephrology and Inst. of Science and Technology in Medicine, Univer. Hosp. of North Staffordshire and Keele Univer., Stoke on Trent, U.K.
[PP-261] Plasma Volume is Normal in PD Patients despite an Ratio of Increased Extracellular Fluid to Total Body Water
Peritoneal dialysis (PD) patients are often thought to be fluid-loaded, and an elevated ratio of extracellular fluid to total body water (ECF:TBW) determined by bioelectrical impedance analysis (BIA) is associated with worse outcomes. It is not known whether excess ECF is intra- or extravascular.
Methods: Plasma volume (PV) was measured using 125I-labeled human serum albumin (I-HSA) in 27 stable PD patients (17 men) and was compared with predicted values for the healthy population. Average age of the study population was 66 years (range: 28–83 years). The Stoke comorbidity scoring system was used. A standard dose of I-HSA was injected, and 3 samples were collected at 10-min intervals. Radioactivity was plotted on a semi-logarithmic scale against time, and the best straight line was drawn through the points. Extrapolation of this graph was used to determine the 0 time activity (used for calculation of PV). The ECF:TBW ratio was determined by BIA and also compared with values derived in a healthy population by Lindley and Lopot.
Results: PV was 2700±615 mL, -1.2% [95% confidence interval: -7.7% to +5.3%] of predicted values. In contrast, the mean ECF:TBW ratio (0.49±0.03) was higher than predicted (0.45± 0.013, p<0.001). The relative increase in ECF:TBW over predicted normal values was associated with increasing comorbidity. PV was identical with and without icodextrin use (n=17), but the ratio of PV to TBW was greater with icodextrin use (p=0.026). The near-normal type B natriuretic peptide values obtained (101.90 pg/mL; range: 0–495.13 pg/mL) reinforce our observation that PV is not expanded.
Conclusions: PD patients are not absolutely plasma-expanded, despite abnormal fluid status determined by BIA, suggesting that excess ECF occurs predominantly in the extravascular space. Icodextrin was associated with relative preservation of intravascular volume, which could be explained by the osmotic influence of icodextrin metabolites in the intravascular compartment.
John B.1, Dalley J.2, Davies S.J.1, Dept. of Nephrol. and Inst. of Sci. and Tech. in Med.,1 Univer. Hosp. of North Staffordshire and Keele Univer., and Dept. of Clin. Biochem.,2 Univer. Hosp. of North Staffordshire, Stoke on Trent, U.K.
[PP-262] Cadaveric Related Kidney Transplantation: A Rare Conclusion of Therapy by PD—Case Study
Kidney transplantation is the most effective therapy for the end-stage renal disease patient. Apart from cases of living related transplantation, the timing of the graft cannot be planned, and the patient must be always be ready for surgery. Success depends on a combination of several factors. One is the education of patients and their relatives about kidney transplantation options.
Here, we present a case study of a 48-year-old patient with chronic renal failure from chronic glomerulonephritis, treated by peritoneal dialysis (PD) since August 2002. The patient was placed on the transplant waiting list in the same year. During 49 months of dialysis (continuous ambulatory PD, automated PD), the patient was free of episodes peritonitis and exit-site infection.
An extensive cerebrovascular event—a fatal condition in a 44-year-old sister of the patient—led the family to approach the tragic situation realistically. The result was a successful transplantation of a cadaveric kidney from the deceased sister to the brother. The APD therapy was concluded effectively.
Kidney transplantation from a relative following a brain death is a rare combination. From the medical viewpoint, it is not exceptional, but the uniqueness rests in the ethical dimension and complex management of the situation.
Lešková L.1, Bena L.2, Dialysis Unit Logman,1 Prešov, and Transplantation Unit,2 Fakultná nemocnica L.Pasteura, Košice, Slovakia.
[PP-263] Noninfectious Complications of CAPD and Their Impact on Technique Survival
Background: Data on non-infectious complications of continuous ambulatory peritoneal dialysis (CAPD) are well documented, but sparse, particularly from developing countries.
Objectives: To describe the occurrence of noninfectious complications of CAPD and their possible impact on technique survival.
Methods: We studied the spectrum of noninfectious complications in 45 end-stage renal disease patients (31 men, 14 women; mean age: 54.5±11.6 years) undergoing CAPD treatment. Double-cuffed straight Tenckhoff catheters were inserted in all patients using a surgical method, and regular CAPD was started on day 15 of catheter insertion. The occurrence of noninfectious complications was noted during patient follow-up.
Results: Overall, noninfectious complications were noted in 18/45 (40%) of cases. Ultrafiltration failure was the most common complication (15.5%), followed by exit-site leak (4.4%), abdominal hernia (6.6%), hydrothorax (4.4%), scrotal swelling (2.2%), hemoperitoneum (2.2%), and catheter malposition (4.4%). Functioning catheters were removed in 6 patients (13.3%) because of refractory (n=4) and fungal (n=2) peritonitis. The cause of the hemoperitoneum was uncertain, and the patient died of bleeding. Right hydrothorax occurred within the 1st month of CAPD because of a diaphragm defect that was successfully treated with pleurodesis. Exit-site leak, catheter malposition and hemoperitoneum developed early (1–4 weeks) in the CAPD therapy; scrotal swelling and abdominal hernia occurred late (12–24 months). Patients with ultrafiltration failure were shifted to hemodialysis (n=3), and 2 underwent renal transplantation. The remaining noninfectious complications (72%) did not affect catheter survival, and CAPD continued in those cases.
Conclusions: Noninfectious complications occurred in 40% of CAPD patients, and ultrafiltration failure was the most common complication (15.5%). Most noninfectious complications (72%) did not affect catheter survival.
Prakash J., Srinivas S., Parekh A., Vohra R., Sharma N., Singh L.S., Ramchandran R., Dept. of Nephrology, Inst. of Medical Sciences, Banaras Hindu Univer., Varanasi, India.
[PP-264] Stroke in Patients with Diabetic Nephropathy
Background: The present analysis looked at the clinical profile of cerebrovascular accidents in patients with type 2 diabetes, with or without diabetic nephropathy.
Methods: Between January 2005 and December 2006, all diabetic patients admitted with stroke were included in the study. Diabetic nephropathy was defined as dipstick- or micral strip–positive proteinuria with or without deranged creatinine in the presence of diabetic retinopathy. Type of stroke, lesion diameter, and site of lesion were reported by the radiologist. National Institutes of Health (NIH) stroke score was calculated within 3 hours of admission. The two groups were compared.
Results: During the study period, stroke was confirmed in 50 patients with type 2 diabetes, 33 (66%) with diabetic nephropathy (group I) and 17 (34%) without (group II). Patients in group I were younger than those in group II [60.27 years vs. 63.88 years,p=nonsignificant (NS)]. Group I patients had higher body mass index and glycosylated hemoglobin, and longer hospital stays (all p=NS). Mean systolic (157.9 mmHg vs. 159 mmHg) and diastolic (96.43 mmHg vs. 95.76 mmHg) blood pressure and admission blood sugar levels (211.4 mg/dL vs. 198.4 mg/dL) were comparable in both groups. Group I patients had significantly higher NIH score (16.34 vs. 11.46, p<0.05), lesion diameter (36.87 mm vs. 23.11 mm, p<0.05), blood urea (53.46 mg/dL vs. 37.17 mg/dL, p<0.05), and serum creatinine (1.88 mg/dL vs. 1.12 mg/dL, p<0.05) than group II did. Mortality was also higher in group I (33% vs. 11.7%, p<0.01).
Conclusions: Patients developing stroke are more likely to have diabetic nephropathy. Patients with diabetic nephropathy develop stroke at a younger age. Severity of stroke is greater in patients with diabetic nephropathy. Presence of nephropathy predicts higher mortality in diabetic stroke.
Soni S.S., Nagarik A.P., Adikey G., Raman A., Dept. of Nephrology, Mediciti Hosps., Hyderabad, India.
[PP-265] Our Experience with Clinical Outcome and Cost Effectiveness of Bedside Permanent PD Catheter Implantation in a Developing Country
Objectives: To compare the complications, clinical outcomes, and cost effectiveness of bedside peritoneal dialysis (PD) catheter implantation with implantation in the operating theatre.
Methods: Over 24 months, we compared 33 patients (22 men, 11 women) on continuous ambulatory PD therapy. Nephrology staff placed 20 catheters percutaneously (group P), and surgical staff placed 13 using conventional surgical techniques (group S). In both groups, swan-neck Tenckhoff catheters were used. Patients were examined for feasibility of bedside implantation, and after counseling and consent, the procedure was carried out under sterile technique in a clean room of our dialysis unit. Locally injected 2% lidocaine was given subcutaneously 3 cm below the umbilicus along the midline, and the procedure for bedside implantation technique was followed. The catheter was immobilized by adhesive plaster at the incision site.
Results: Post-procedure complications included 2 cases of bloody effluent and 1 catheter malposition in group P versus 3 cases of bloody effluent, 2 pericatheter leaks, 2 postoperative peritonitis, 2 subcutaneous leaks, and 2 incisional hernias in group S. Wound healing was better in group P than in group S. Total hospital stay in group P was 3±2 days as compared with 18±2 days in group S. Physician fees for group P were $195±52 (Rs7500±2000) as compared with $325±52 (Rs12 500±2000) in group S. Bed charges for group P were $26±13 (Rs1000±500) as compared with $286±104 (Rs11 000±4000).
Conclusions: The bedside approach allows for rapid initiation of PD; minimizes patient discomfort; reduces hospital stay, surgery cost, bed charges, operating room charges, and anesthesia service charges; and helps to reduce the morbidity and mortality associated with general anesthesia. In a resource-scarce setting, bedside implantation is a cheaper option and should be practiced in developing countries.
Gupta P.1, Dawale P.1, Mandhanya A.1, Bansal D.1, Gupta G.1, Abraham G.2, Pt.J.N.M. Medical College and GBG Kidney Care Hosp.,1 Raipur, and Madras Medical Mission,2 Chennai, India.
[PP-266] Visfatin, a New Adipocytokine, and Its Relationship with Inflammation and Endothelial Function in Dialyzed Patients
Background: Visfatin (Vf) is an adipocytokine that recently generated much interest. Inflammation and endothelial cell (EC) damage or injury is invariably associated with clinical conditions such as thrombosis, atherosclerosis, and their major clinical consequence, cardiovascular disease.
Methods: In hemodialyzed (HD) and peritoneally dialyzed (PD) patients (pts), we assessed Vf and markers of coagulation [thrombin–antithrombin complex (TAT); prothrombin fragments 1+2 (PTF1+2)], fibrinolysis [tissue plasminogen activator, plasminogen activator inhibitor 1 (PAI-1), plasmin–antiplasmin (PAP)], EC function/injury [von Willebrand factor (vWF), thrombomodulin, intercellular adhesion molecule (ICAM), vascular cell adhesion molecule (VCAM), CD146], and inflammation [high-sensitivity C-reactive protein (hsCRP), tumor necrosis factor α (TNFα), and interleukin-6 (IL-6)].
Results: Triglycerides, hsCRP, urea, creatinine, IL-6, TNFα, vWF, PTF1+2, TAT, PAP, thrombomodulin, ICAM, VCAM, CD146, PAI-1, leptin, adiponectin, and Vf were elevated in dialyzed pts as compared with controls. Serum albumin, hemoglobin, and hematocrit were significantly lower in dialyzed pts than in the control group. In a univariate analysis, Vf correlated significantly in HD pts with CD146, Kt/V, IL-6, adiponectin, apelin, dialysis vintage, PTF1+2, and ICAM, and tended to correlate with hsCRP. In PD pts, Vf correlated significantly with hemoglobin, ICAM, VCAM, and CD146. In the healthy volunteers, Vf correlated significantly with ICAM, serum creatinine, and IL-6. In a multiple regression model that used parameters that correlated or tended to correlate with Vf (p<0.1), Vf was independently correlated in HD pts only with Kt/V (²=-0.22, p=0.046), dialysis vintage (²=0.19, p=0.049), and IL-6 (²=0.26, p=0.008). Multiple adjusted r2=0.24, F=3.45, p<0.00162, standard error=72.73. In PD pts, Vf was not independently correlated with any of the studied parameters.
Conclusions: Elevated Vf related to markers of inflammation may represent a novel link between inflammation and adipocytokines in dialyzed pts. Dialysis vintage and adequacy influence Vf in dialyzed pts.
Malyszko J.1, Malyszko J.S.1, Kozminski P.2, Pawlak K.1, Mysliwiec M.1, Nephrol. Dept.,1 Med. U., and Dialysis Unit,2 Poland.
[PP-267] Encapsulating Peritoneal Sclerosis in Patients on PD—A Single-Center Experience
Encapsulating peritoneal sclerosis (EPS) is a rare but most serious complication in peritoneal dialysis (PD) patients (pts), with a prevalence of 0.54%–7.3%. Progressive deterioration of the peritoneum as a result of PD and superimposition of inflammatory stimuli (peritonitis, glucose degradation products, beta-blockers, plasticizers, autoimmune disease, abdominal surgery) are thought to play a key role in the pathogenesis of EPS. Diagnosis is based on clinical symptoms (subocclusion, signs of inflammation and peritoneal adhesions, hemoperitoneum, ultrafiltration failure), radiologic findings, and macroscopic (surgical) and histopathologic criteria. Treatment includes total parenteral nutrition, transfer to hemodialysis (HD), medications (steroids, immunosuppressants, tamoxifen, angiotensin converting-enzyme inhibitors), and surgery. If recognized, even with all therapeutic modalities, EPS mortality is more than 50%.
Objectives: To confirm the prevalence, risk factors, and outcome of EPS in our cohort of pts between 2005 and 2007.
Methods: Of 75 continuous ambulatory PD and automated PD pts, 8 clinically suggestive cases (1 man, 3 women; age: 50.5±22 years; on PD: 2.5–5.7 years) were evaluated for EPS by abdominal X-ray, ultrasonography, computed tomography (CT), and laparoscopic and histologic investigations.
Results: In 4 of the 8 pts, we found CT abnormalities and histologic criteria for EPS. Before switching to PD, 2 pts had been on HD (1 also had a failed kidney transplant). One woman had recidivate ileus, and although switched to HD after the 1st ileus episode, died from gut perforation and sepsis, with a macroscopic picture of cocoon-like encapsulation of the intestine. (Her underlying disease was systemic lupus erythematosus.) Another 3 pts experienced complete relief from bowel obstruction with conservative treatment alone, including electrolyte and fluid substitution, temporary nasogastric suction, and switch to HD.
Conclusions: Clinical suspicion gave us 50% probability of EPS, which had an overall prevalence of 5.3% and varying outcomes in our cohort of pts. All suspected but unconfirmed cases need to be closely followed for early recognition of disease.
Pilcevic D.D.1, Paunic Z.T.1, Tufegdzic I.2, Kovacevic Z.1, Clin. Nephrol.1 and Inst. of Pathol.,2 Military Med. Acad., Belgrade, Serbia.
[PP-268] High Prevalence of Subclinical Hypothyroidism and Its Impact on Left Ventricular Function in CAPD Patients
Background: Despite the high prevalence of subclinical hypothyroidism in patients (pts) with chronic kidney disease, little is known about the clinical features and implications of this disorder in end-stage renal disease pts. We investigated the prevalence of subclinical hypothyroidism and evaluated the effect of subclinical hypothyroidism on left ventricular (LV) function in continuous ambulatory peritoneal dialysis (CAPD) pts.
Methods: This cross-sectional study examined 51 pts maintained on PD for more than 3 months. Those who had previous intrinsic thyroid disease or clinical symptoms or signs of heart failure were excluded. Echocardiography and blood samples for thyroid function were performed. Subclinical hypothyroidism was defined as blood thyroid stimulating hormone (TSH) level >5 mIU/L with a normal free T4 level.
Results: Subclinical hypothyroidism was detected in 14 of the 51 pts (27.5%). Autoimmune thyroiditis was less common in pts with subclinical hypothyroidism (n=4, 28.6%), considering its prevalence in the general population. Pts with subclinical hypothyroidism had a lower LV ejection fraction (57.4%±10.4% vs. 66.6%±8.7%, p=0.002) and a lower endoFS (32.1%±7.4% vs. 40.0%±8.2%, p=0.009) as compared with pts with normal TSH levels. In addition, log TSH was inversely associated with LV ejection fraction (r=-0.361, p=0.009) and endoFS (r=-0.320, p=0.022). In a multivariate linear regression analysis adjusted for age, sex, diabetes, previous cardiovascular disease, serum albumin, log C-reactive protein, and T3, log TSH was an independent correlate of LV ejection fraction (²=-0.388, p<0.001).
Conclusions: Our findings suggest that subclinical hypothyroidism is common and might be implicated in cardiac dysfunction in CAPD pts.
Kang E.1, Lee K.1, Bae J.1, Nam J.1, Yoo T.1, Shin S.1, Han S.2, NHIC Ilsan Hosp.1 and Yonsei Univer. College of Medicine,2 Korea.
[PP-269] Levels and Determinants of Prohepcidin in PD and HD Patients
Background: Iron metabolism is impaired in chronic kidney disease. Hepcidin functions as a key regulator of iron absorption in response to body iron stores, preventing iron accumulation. We evaluated prohepcidin and inflammation parameters, iron parameters, and hemoglobin levels in peritoneal dialysis (PD) and hemodialysis (HD) patients (pts).
Methods: We studied 85 PD pts (47 men, 38 women), 43 HD pts (28 men, 15 women) on regular follow-up, and a control group comprising 41 healthy controls (14 men, 27 women). Demographic characteristics of all pts were recorded. Prohepcidin, high-sensitivity C-reactive protein (hsCRP), and iron status were assessed.
Results
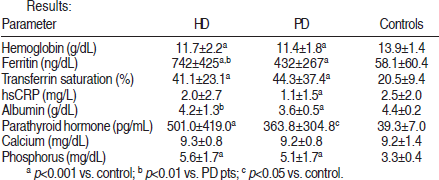
p<0.001 vs. control;
p<0.01 vs. PD pts;
p<0.05 vs. control.
Prohepcidin levels were significantly higher in pts receiving dialysis therapy than in healthy controls. Compared with PD pts, HD pts had higher prohepcidin levels, but the difference was statistically nonsignificant (393.4±157.3 vs. 361.3±40.1, p=0.19). PD pts showed a weak positive correlation between prohepcidin and creatinine (r=0.232, p=0.033, Pearson correlation). There were no correlations between prohepcidin and hsCRP, and between hemoglobin and iron parameters in PD and HD pts.
Conclusions: Results suggest that dialysis therapy is associated with elevated prohepcidin, which is not directly related to inflammation, malnutrition, indices of iron metabolism, or hemoglobin. PD pts have relatively lower prohepcidin levels than HD pts do, but larger-scale studies are needed to determine and confirm a possible different effect of various dialytic modalities.
Turgut F.1, Kanbay M.1, Altay M.2, Uz E.1, Bavbek N.1, Koca C.3, Secilmis S.2, Duranay M.2, Akcay A.1, Covic A.4, Dept. Nephrol.,1 Fatih U. School of Med.; Dept. Nephrol.,2 Ankara Research and Training Hosp.; and Dept. Biochem.,3 Fatih U. School of Med., Turkey; and Dept. Nephrol.,4 C.I. Parhon Ur. Hosp., Dial. and Transplant. Ctr., Romania.
[PP-270] Natural Rubber Latex Allergy in PD Patients
Background and Objectives: End-stage renal disease patients on continuous ambulatory peritoneal dialysis (CAPD) therapy can be a suspected risk group for natural rubber latex allergy (NRLA) because of their intense exposure to latex through catheters, gloves, and anesthetic equipment, especially during peritonitis attacks. We evaluated the incidence of NRLA in CAPD patients and the frequency of peritonitis attacks as a risk factor for NRLA.
Methods: We included 50 CAPD patients with frequent peritonitis history (group I: mean age: 38.5±10.8 years; 24 men, 26 women; mean duration of CAPD: 45.5±31.3 months), 30 patients without any peritonitis episodes (group II: mean age: 35.4±11.5 years; 18 men, 12 women; mean duration of CAPD: 28.8±32.2 months), and 26 healthy controls (group III: mean age: 35.7±9.9 years; 14 men, 12 women). Exclusion criteria were age<18 years, pregnancy, severe cardiovascular disease, unstable pulmonary disease, or therapy with beta-blockers, steroids, or antihistaminic drugs. A questionnaire-based history was taken, and an examination was carried out by an allergist for atopic diseases (food allergy, hay fever, asthma, atopic eczema, hand eczema), number of preceding invasive medical procedures (conventional, laparoscopic, endoscopic operations), immediate-type hypersensitivity reactions during medical care, NRL hypersensitivity, occupation, general medical history. Pulmonary function test (PFT) and prick skin test were done for each patient to determine allergic tendency.
Results: We excluded 8 patients because of impaired PFT with negative NRLA. All of the groups were similar in terms of demographic data, questionnaire items, PFT results (all p>0.05) and peritonitis attacks. No NRLA was present in group I or II (p>0.05). Only 3 subjects in group III had NRLA (11.5%, p<0.01).
Conclusions: In this cross-sectional study, we found no NRLA in CAPD patients. CAPD patients are not at increased risk of NRL hypersensitivity when matched with a healthy population in terms of sociodemographic data.
Altunoglu A.1, Canoz M.B.1, Yavuz D.D.1, Turkkan O.2, Ozbek O.3, Akman B.1, Eyuboglu F.O.2, Arat Z.1, Ozdemir N.F.1, Nephrology,1 Pulmonary Diseases,2 and Pediatrics,3 Baskent Univer. Faculty of Medicine, Ankara, Turkey.
[PP-271] PD in Patients with the Human Immunodeficiency Virus
Patients with HIV and chronic renal failure (CRF) are thought to have a poorer outcome with peritoneal dialysis (PD) than with hemodialysis (HD), because of an increased incidence of peritonitis with unusual infecting organisms and an increased rate of systemic infections.
Methods: We analyzed our experience from November 1995 to December 2007 with 12 PD patients (10 men, 2 women; mean age: 42±8 years; mean follow-up on PD: 30±29 months) with HIV.
Results: Ten patients had been addicted to intravenous heroin. All were positive for hepatitis C virus and negative for hepatitis B antigen. Eight were on continuous ambulatory PD, and 4 on continuous cycling PD. Causes of chronic renal failure were 7 chronic glomerulonephritis, 2 diabetic nephropathy, 1 thrombotic microangiopathy, and 2 unknown. Six patients suffered hypertension.
HIV Evolution: Viral charge lowered in all patients. CD4 levels improved in 10. All patients received long-term antiretroviral treatment. Only 1 patient developed an opportunistic infection (Pneumocystis carinii pneumonia) with excellent evolution after cotrimoxazole.
PD Evolution: Four patients had 9 peritonitis episodes (3 Staphylococcus epidermidis, 1 Mycobacterium fortuitum, 1 Candida albicans, 1 Escherichia coli, 1 Klebsiella, 1 Pseudomonas). Exit-site infection was present in only 1 patient (Corynebacterium species). Eleven patients were admitted to the hospital on 23 occasions (4 for peritonitis, 7 for respiratory tract infection, 2 for hypertensive encephalopathy, and 10 other causes). All patients showed good technique compliance. Mean bodyweight increase was 4±2.8 kg. Five patients died (1 Pseudomonas leg abscess, 2 cardiac ischemic events, 1 cachexia, and 1 peritoneal sclerosis).
Conclusions: HIV patients can be successfully treated with PD. They do not present higher rates of peritonitis, and the infecting organisms are not more difficult to treat. We think that PD must be the therapy of choice in these patients, because PD minimizes the risk of HIV transmission.
Amezquita Y., Rivera M., Merino J., Caldés S., Alarcón C., Villacorta J., Jiménez S., Teruel J., Ortuño J., Hosp. Ramon y Cajal. Alcalá de Henares Univer., Spain.
[PP-272] Quality of Life: Some Psychological Aspects of Patients on HD and PD
People with chronically progressive renal failure and patients on dialysis are forced to confront a so-called trial of re-socialization— that is, to change from one social group (healthy people) to another (chronically disabled people). They must radically change their identity, and as a result, particularly tough psychological issues arise. Disabled people have low social face, and are frequently put into an unprofitably dependent position as compared with other social groups.
Objectives: We analyzed some of the psychological problems in the period of adaptation to terminal renal failure and of start of treatment in 30 patients on continuous ambulatory peritoneal dialysis (CAPD) or 30 patients on hemodialysis (HD).
Methods: The anonymous questionnaires explored tension and anxiety (questionnaire from C. Spillburger, WIPPF test, self-estimation depressive scale by U. Zung).
Results: The period of adaptation to end-stage renal failure is a process of regaining assurance, higher self-awareness, and overall, accepting the aftereffects of a chronic disease. For patients on CAPD, as compared with patients on HD, the process is shorter, with fewer stressful situations.
Conclusions: Quality of life in the period of adaptation, estimated using several psychological indices, is better in patients on CAPD than in those on HD.
Dimitrova–Zlatkova R., Paskalev D., Ikonomov V.C., Clinic of Nephrology and Dialysis, Univer. Hosp. “St. Marina” Varna, Bulgaria.
[PP-273] Patient and Technique Survival and Factors Affecting Mortality on CAPD in Turkey: 12 Years’ Experience in a Single Center
Background: We investigated patient and technique survival and factors affecting mortality in Turkish continuous ambulatory peritoneal dialysis (CAPD) patients.
Methods: This retrospective study included 418 CAPD patients. Demographic, clinical, and biochemical data were collected from medical records.
Results: Mean age at the start of CAPD was 45.9±14.3 years, and mean peritoneal dialysis duration was 37.4±28.3 months (median: 30 months, range: 4–137 months). Diabetes mellitus was the most common cause of end-stage renal disease (34.7%). There were 89 (21.2%) deaths. Kidney transplantation was performed in 25 (6.0%) patients, and 74 (17.7%) patients were transferred to hemodialysis (HD).
Estimation of technique survival by Kaplan–Meier analysis was 96.1%, 83.2%, 67.6%, 45.8%, and 33.6% at 1, 3, 5, 8, and 10 years. Technique survival was associated with transfer from HD [relative risk (RR): 1.84; p=0.01], peritonitis rate (RR: 3.33; p<0.001), and peritoneal Kt/V urea (RR: 0.29; p<0.001) in a Cox proportional hazards model analysis. Estimation of patient survival by Kaplan–Meier analysis was 96.8%, 83.7%, 68.8%, 50.2%, and 40.7% at 1, 3, 5, 8, and 10 years respectively. In the Cox proportional hazards model analysis, age (RR: 1.01; p=0.05), transfer to CAPD from HD (RR: 1.83; p=0.03), comorbid cardiovascular disease (RR: 1.89; p=0.004), serum creatinine level (RR: 0.75; p<0.001), total Kt/V urea (RR: 0.34; p<0.001), peritonitis rate (RR: 1.86; p<0.001), and dialysate-to-plasma ratio (D/P) of creatinine (RR: 6.51; p=0.04) predicted survival.
Conclusions: Survival rates in patients in Turkey seem to be better than those in the United States and Europe; however, a definitive conclusion requires further studies adjusted for more extensive demographic features and comorbidities. The factors affecting mortality in Turkish CAPD patients are similar to those seen in other populations.
Sipahioglu M.H., Aybal A., Ünal A., Tokgöz B., Oymak O., Utas C., Erciyes Univer., Medical Faculty, Dept. of Nephrology, Kayseri, Turkey.
[PP-274] Age and Education Affect Beliefs about Medications: A Questionnaire Survey of Patients on Chronic PD
Objectives: This cross-sectional study investigated beliefs about the necessity of the prescribed peritoneal dialysis (PD) regimen and concerns about taking prescribed medications, and assessed the factors related to those specific medications beliefs in 118 patients on chronic PD.
Methods: Patients’ beliefs about their PD regimen and medicines were assessed using the modified Beliefs about Medicines (BMO) questionnaire. The modified BMO comprises two 5-item scales assessing the respondent's beliefs about the necessity for, and concerns about, their prescribed PD regimen and medicines. We analyzed relationships between the BMO scales and their sociodemographic and clinical factors.
Results: Most patients (93.1%) agreed or strongly agreed that their prescribed PD regimens were necessary for their health. However, 15.1% were concerned about potential adverse consequences of medications and dialysis treatment. The overall necessity score (17.7±3.8) was higher than the concern score (16.9±3.5, p<0.02). Young age (r=0.237, p=0.01) and high education (r=0.200, p=0.03) were correlated with a higher concern score regarding medication side effects. There was no association between necessity or concern about PD therapy and sex, marital status, PD duration, history or no history of hemodialysis, or occupation.
Conclusions: Most PD patients have positive beliefs about the necessity for and concerns about their PD therapy and prescribed medicines. However, the concern score regarding medication side effects is high and is associated with younger patients with high education.
Chen J., Liao S., Nephrology Div., Dept. of Internal Medicine, Chang Gung Memorial Hosp.–Kaohsiung Medical Ctr., Chang Gung Univer. College of Medicine, Taiwan.
[PP-275] Using Human Peritoneal Cells for Gene Expression Analysis from Peritoneal Dialysis Effluent
Peritoneal dialysis (PD) is known to be a therapeutic tool for end-stage renal failure. During PD, waste fluid is obtained. This fluid contains polymorphonuclear, mesothelial, and endothelial cells that are present in peritoneal cavity. Familial Mediterranean fever (FMF) is an autosomal recessive disease characterized by recurring inflammatory attacks of synovial membranes such as pericardium, peritoneum, and joints. More than 95% of patients show peritoneal involvement. We isolated polymorphonuclear cells obtained from peritoneal dialysis effluent and compared MEFV gene expression in those cells with MEFV gene expression in blood polymorphonuclear cells. PD effluent was obtained after informed consent from patients or parents or both. The cells were obtained in noninfectious effluent and toward the end of the dwells.
Methods: The PD effluent was centrifuged (800g, 15 minutes, 4°C). Total cells were resuspended and cultured in RPMI 1640 culture medium, fetal bovine serum, penicillin, and streptomycin. For cell culture experiments, the cell suspension was plated into 6-well plates and maintained at 37°C in a 5% CO2 environment overnight. The cells were then treated with lipopolysaccharide [LPS (10 μg/mL for 2 hours)] or other reagents. RNA was extracted with TRIzol reagent, and cDNA library was prepared. Then MEFV gene expression analysis was performed. The results of quantitative PCR showed an increase in MEFV gene expression by a factor of approximately 10 upon LPS stimulation, after normalization to internal control GAPDH.
Conclusions: PD effluent is a cell suspension. Although dialysate effluent is usually discarded after a dwell, it is a useful tool for gene expression analysis, which may help in understanding the mechanism of diseases that affect the peritoneal cavity.
Yilmaz E., Ekim M., Akar N., Ankara Univer. Medical School, Turkey.
[PP-276] is There any Relationship between Serum Zinc and other Parameters in PD and HD Patients?
Objectives: Zinc is an element that plays an important role in biologic systems as a component of proteins, enzymes, and antioxidants. The aim of the present study was to determine correlations between serum zinc and other parameters in hemodialysis (HD) and continues ambulatory peritoneal dialysis (CAPD) patients.
Methods: This cross-sectional study included 102 patients [75 on HD, 27 on CAPD; 25% <50 years of age; 32% women; median duration of dialysis: 13 months (range: 1–120 months)]. Serum zinc level and other parameters were measured in patients with chronic renal failure and in those under dialysis at least for 1 month.
Results: Mean serum hemoglobin, calcium, albumin, and zinc were, respectively, 10±2 g/dL, 8.8±1.2 mg/dL, 3.6±0.5 g/dL, and 23±4 μmol/L (range: 13–33 μmol/L). Serum zinc was not significantly different in HD and CAPD patients (25±6.9 μmol/L vs. 23.6±3.8 μmol/L), in men and women (25.5±6.9 μmol/L μmol/L vs. 23.5±4.2 μmol/L), in patients <50 and ≥50 years of age (24±3.8 μmol/L vs. 25±6.9 μmol/L), and in hypertensive and non hypertensive patients (24.6±5 μmol/L vs. 25±8 μmol/L). Serum zinc was positively correlated with serum albumin (r=0.3, p=0.0001) and with calcium (r=0.2, p=0.045). Serum zinc had no correlation with serum parathyroid hormone, phosphate, triglycerides, cholesterol, ferritin, iron, total iron binding capacity, and hemoglobin. Serum zinc was not significantly different in patients treated or not treated with calcium carbonate (25±6 μmol/L vs. 25±8 μmol/L) and treated or not treated with erythropoietin (23.9±3.8 μmol/L vs. 23.2±4.3 μmol/L).
Conclusions: We conclude that lower serum zinc correlates with lower serum albumin as a marker of nutrition status in dialysis patients. However, there are no correlations between serum zinc and other parameters in dialysis patients. Calcium carbonate as a phosphate binder does not affect serum zinc concentration.
Nouri–Majalan N., Moghadasi-mousavi S., Shaheed Sadoughi Univer. of Medical Sciences and Health Services, Iran.
[PP-277] Administration of the Sudan National Peritoneal Dialysis Program: The Challenges
Background: Continuous ambulatory peritoneal dialysis (CAPD) has an invaluable role in the integrated management of end-stage renal disease. Until recently, hemodialysis was the only option available for the growing dialysis population of Sudan, a country of vast proportion and growing economics. We present an overview of how the Sudan National Peritoneal Dialysis Program (SNPDP) came into existence.
Overview: The initiative came from Prof. Hassan Abu-Aisha. He, and a small number of dedicated doctors and nurses, with generous support from the national Ribat University and the Central Medical Supplies (CMS) corporation, established the first regular peritoneal dialysis (PD) center in Sudan in June 2005. Into an area of about 300 m2, they managed to squeeze an 8-bed ward for training and inpatient care, a small operating theater for catheter insertion, an administrative office, a central database, a training hall for doctors, a library, and a research headquarters.
Six other centers joined the program during the 1st year, by the end of which, the program was recognized as national in scope and was adopted by the federal Ministry of Health. In 30 months of operation, it has served about 196 patients and incorporated a new center based outside the capital, Khartoum.
The central office is responsible for rationalizing the program budget and participant recruitment, setting the local management protocols, providing guidebooks and patient brochures, training doctors and nurses, supervising the work of all centers, collecting and analyzing program data, organizing workshops and academic activities, and organizing the program participation at international conferences.
The program has faced the challenges of limited space, meager resources, and difficult transportation (to name but a few), but with patience and persistence, it managed to overcome many of those challenges.
Conclusions: The SNPDP has fulfilled many of its initial goals as a pilot project and has great potential for further development.
Elamin S., Abu-Aisha H., Abdul-Kareem S., Sudan National Peritoneal Dialysis Program.
[PP-278] the Sudan National Peritoneal Dialysis Program: Where are we Now?
Background: We critically analyzed the progress of the Sudan National Peritoneal Dialysis Program (SNPDP) during its 30 months of operation.
Methods: Patients who had been on continuous ambulatory peritoneal dialysis (CAPD) for at least 3 months were included in the analysis.
Results: The program maintained 137 patients on CAPD, with a median follow-up of 8.6 months, and during 2007, 46 new patients were enrolled. Mean age of the patients was 43.8 years; 63.5% were male; and 23.4% were children. A new CAPD center was established outside the capital, Khartoum; however, 36.3% of patients being followed in Khartoum come from other states. Among the patients, 78% were transferred from hemodialysis (HD), 9.8% had a failed kidney transplant, and only 12.2% were new to dialysis. Most patients (65.7%) were no longer suitable for HD.
At year-end 2008, 57 patients were on active CAPD; of the 80 patients who left the program, 16.3% received a kidney transplant, 2.5% became dialysis-independent, 35% were transferred to HD, and 46.3% died. Only 8.1% of deaths were related to peritonitis. Among the 28 patients who were transferred to HD, the cause of transfer was peritonitis in 60.9%, social or personal reasons in 26.1%, and technical difficulties in 13%. The overall peritonitis rate was 1 episode in 13.2 patient–months.
Conclusions: The SNPDP is currently burdened with a large number of patients who are no longer fit for other forms of renal replacement therapy. That situation reflects how badly needed the CAPD modality of dialysis has been in Sudan; however, it has had a negative effect on program performance indicators. Early occurrence of technical difficulties may reflect a learning curve effect. The contribution of social and personal factors to patient drop-out suggests that more focus on patient support is needed.
Abu-Aisha H., Elhassan E.M., Elamin S., Sudan National Peritoneal Dialysis Program.
[PP-279] Noninfectious Complications of CAPD among Sudanese Patients
Objectives: To measure the frequency of noninfectious complications among Sudanese continuous ambulatory peritoneal dialysis (CAPD) patients, to identify their potential risk factors, and to measure the affect of those factors on dialysis.
Methods: This retrospective survey included all patients who were on CAPD between June 2005 and July 2007. Data were collected from patient records using a checklist.
Results: A total of 148 patients [90 men; mean age: 41.8 years (range: 1.5–76 years); overall treatment duration: 1123.1 patient–months (mean: 8.2 months; range: 0.07–34.27 months)] were implanted with 155 catheters. Noninfectious complications occurred in 75 patients (50.7%). Exit-site leak occurred in 12 patients (8.1%), with an incidence of 0.13/patient–year. Leak was associated with higher body mass index (BMI) and exit-site infection (p=0.01 and 0.007 respectively). Hemorrhagic effluent was experienced by 12 patients (8.1%), with an incidence of 0.13/patient–year. The condition was minor in 10 patients (4 with menstruation). Only 2 patients had hernia (1.4%), with an incidence of 0.02 hernia/patient–year. Catheter block was detected in 19 patients (12.1%): 5 because of omentum (all in children), and 14 because of fibrin. Catheter malposition was identified in 7 patients (4.7%). There were no associated risk factors for hernia, hemorrhagic effluent, and catheter block or malposition. Hypokalemia, hypoalbuminemia, and gastrointestinal symptoms were fairly common (experienced by 23, 19, and 14 patients respectively) and were associated with longer dialysis duration (p=0.001, 0.05, and 0.048 respectively). Noninfectious complications were responsible for drop-out of 18 patients (20.5% of total drop-out), and were associated with 3 deaths, mainly from underdialysis.
Conclusions: Noninfectious complications of CAPD were fairly common in our patients, but the rates were comparable to those in regional and international reports.
Mekki M.O., Sanousi H., Fedail H.M., Khamis A., Abu-Aisha H., Sudan National Peritoneal Dialysis Program.
[PP-280] Peritoneal Dialysis after Medial Abdominal Laparotomy
Abdominal laparotomy is considered a relative contraindication for peritoneal dialysis (PD). Thus, clinical reports concerning this subject are scarce. Here, we report 3 patients with a past history of abdominal surgery who were initiated onto PD at our unit.
Methods: We retrospectively reviewed the medical records of patients who received treatment with PD and, previous to dialysis, underwent a middle laparotomy.
Case 1: A 31-year-old man with chronic renal failure (CRF) secondary to vesicoureteral reflux was transferred to hemodialysis because of the absence of a permanent vascular access. One month before collocation of a peritoneal catheter, the patient suffered a gastrointestinal hemorrhage. A bleeding ulcer was found in the posterior wall of the duodenum, and a middle laparotomy was performed. PD was initiated 1 month later. This patient remains on PD 81 months later without relevant problems.
Case 2: A 66-year-old man with CRF secondary to nephroangiosclerosis had undergone PD for 35 months. A partial gastrectomy through a middle laparotomy had previously been performed because of a gastric ulcer. His evolution in PD has been favorable, except for 3 episodes of bacterial peritonitis.
Case 3: A 67-year-old man with bilateral renal carcinoma was treated with PD for 44 months. He was successfully maintained on PD after radical bi-nephrectomy, resection of retroperitoneal ganglionic metastases, and inferior cava thrombosis.
Conclusions: In our experience, patients with previous abdominal surgery must not be routinely excluded from PD, because PD can be successfully performed in those patients.
Caldes S., Rivera M., Amezquita Y., De La Morena C., Rodriguez Mendiola N., Martins J., Jiménez S., Villacorta J., Ortuño J., Hosp. Ramon y Cajal. Alcalá de Henares Univer., Spain.
[PP-281] Impact of Government Policy on PD Penetration: A Model of Thailand
Generally peritoneal dialysis (PD) penetration has been only 10%–12% of end-stage renal disease (ESRD) cases. Only countries that currently run a “PD First” policy such as Mexico and Hong Kong have high PD penetration. In Thailand, PD had been used by only about 10% for a decade, only 800 cases were on PD in 2007 as compared with 14 000 cases on HD. Fewer than 60 hospitals provided continuous ambulatory PD (CAPD) therapy, and most of them cared for fewer than 20 cases.
Effective 1 January 2008, the Thai government decided to provide free CAPD for poor ESRD patients through the National Heath Security Office. Along with that policy, a CAPD practice guideline was developed by the Nephrology Society of Thailand to set a standard for PD practice, and a national curriculum for CAPD training is under development. At least 23 hospitals were pleased to join the project, and they sent their medical personnel to attend a short intensive training course on PD.
At the end of Jan 2008, about 100 new patients had started on CAPD therapy, and more than 100 patients has registered for catheter implantation. In the first year, 1000 new PD cases are expected to be recruited, and about 10 000–15 000 cases in the decade. Surprisingly, the price of PD solution has declined more than 30% because of bulk processing, meaning that Thailand can save at least 25% over the former regular cost.
Government policy has clearly affected PD practice and promoted PD penetration. With proper measures, a catastrophic effect on Thai economic status can be overcome.
Sirivongs D., Pongskul C., Chunlertrith D., Wiangnon P., Homnan N., PD Training Ctr., Faculty of Medicine, Khon Kaen Univer., Thailand.
[PP-282] Heparin Improves Abdominal Pain in PD Patients
Heparin is a glycosaminoglycan with well-known anticoagulant activity. However, heparin has a host of biologic actions beyond its role as an anticoagulant. It modulates the activity of various inflammatory cells, affects the synthesis of extracellular matrix, prevents the development of peritoneal adhesions, and has antiproliferative effects.
In a prospective study between January 2006 and December 2007, all peritoneal dialysis patients with unknown abdominal pain were entered. For exclusion of peritonitis, peritoneal fluid cellular count and culture were examined, and all secondary causes of peritonitis and abdominal pain were excluded. During the night dwell, heparin 5000 U in 2 L 1.5% dextrose solutions was intraperitoneally infused for 7 days. If clinical improvement did not occur, treatment was continued for up to 10 days.
A total of 7 patients (4 women, 3 men; 25–70 year of age) met the criteria. The peritoneal fluid white blood cell count was 2–50/ mL. In 2 patients, pain occurred during fluid inflow. In all 7 patients, abdominal pain was improved after 7–10 days of intraperitoneal heparin administration, and peritoneal white blood cell count was reduced to 0–10/mL.
It seems that most of the abdominal pain in peritoneal dialysis patients is inflammatory in origin. We speculate that formation of C3a and C5a, complement-dependent chemotactic activity, and neutrophil recruitment are inhibited by heparin.
Zolali N., Ardalan M., Tabriz Univer. of Medical Sciences, Peritoneal Dialysis Unit, Turkey.
[PP-283] Eleven Years of PD: Experience of a Single Center
In this retrospective study, we reviewed all 49 patients (25 men, 24 women) on peritoneal dialysis (PD) program at our center from 1996 to 2007 (82.3 treatment years).
Dialysis was managed by continuous ambulatory PD (CAPD) in 47 patients, and by automated PD only 2 patients. The patients were 18– 78 years of age (mean: 46.95±17.7 years). Mean follow-up was 20.16±20.03 months (range: 1–87 months). Patient survival rates after 1, 2, 3, and 4 years were 89%, 89%, 77%, and 41% respectively. Glomerulonephritis was the major cause of end-stage renal disease (14/28 patients, 50%); NAS and diabetic nephropathy were represented at 24.4% and 22.4% in our PD population. PD was the first-choice treatment in 32 patients (65%). Straight Tenckhoff (n=39) and swan-neck double-cuff catheters (n=15) were inserted by laparoscopic and classical surgical implantation techniques. Patients on CAPD used 4 or 5 exchanges daily. The peritonitis rate was 1 episode/28 months. The main causative agent in peritonitis was Staphylococcus aureus (36.4%). Exit-site infection occurred in 19 patients, tunnel infection in 6, hernias in 8, and dialysate leak in 6. During follow-up, 10 patients (20.4%) died, 10 (20.4%) were transferred to hemodialysis, 4 (8.2%) were transplanted, and 25 (51%) are still on PD. The most common causes for discontinuing treatment were ultra-filtration failure, catheter problems, and relapsing peritonitis.
In conclusion, our data suggest that PD is an equally worthy choice for treating end-stage renal disease (ESRD). PD should be considered as a first-choice treatment in ESRD.
Stojkovski L.1, Oncevski A.1, Simeonov R.2, Jovcevski A.3, Zafirovska K.1, Sikole A.1, Polenakovic M.4, Nephrology Clinic,1 Pediatric Surgery Clinic,2 and Abdominal Surgery Clinic,3 Univer. Clinical Ctr., and Macedonian Acad. of Science and Arts,4 Skopje, Macedonia.
[PP-284] Pregnancy and Successful Birth in a Nephritic Patient on PD
A 24-year-old women who came to the hospital with a complaint of headache was hospitalized with a diagnosis of hypertension and nephritic syndrome. In addition to the nephritic syndrome diagnosis, the patient had a secondary chronic kidney failure. After the examinations at the hospital, it was understood that the woman was 4 weeks pregnant. Because the urea and creatinine values in the patient were high, a peritoneal dialysis catheter was implanted. The patient, who was prescribed 2000 mL 1.5% dextrose solution 4 times daily, was sent home after examinations and inspections were completed to continue her dialysis in the same manner until her last trimester. At that time, no negative consequences had occurred for baby or mother.
During the pregnancy, urea was 97–115 mg/dL, and creatinine was 4.1–7.34 mg. At the 28th week, her peritoneal prescription was changed to 6 exchanges daily with 1750 mL solution. At the 35th week, blood pressure has started to exceed 120/80 mmHg, and the patient was started on once-daily 250 mg methyldopa. For anemia, the patient was given subcutaneous darbepoetin alfa and oral iron and calcium.
At week 37.5, preterm contractions started, and because the patient had ended her first pregnancy with a caesarean delivery, her second birth was done by caesarean too. The baby was a boy, 2300 g, 46 cm, and Apgar score 9–10. After the birth, it was decided to switch the patient to hemodialysis.
In conclusion, the pregnancy ended successfully with the patient continuing to use continuous ambulatory peritoneal dialysis treatment.
Akay H., Parpucu H., Altay M., Tekeli N., Çeri M., Duranay M., Dept. of Nephrology, Ankara Education and Research Hosp., Ankara, Turkey.
[PP-285] PD Offers Lower Risk of Infection from HCV among Dialysis Patients
Objectives: Hepatitis C viral (HCV) infection represents one of the main factors limiting renal transplantation in the hemodialysis (HD) population in our country. Peritoneal dialysis (PD) as the first-choice treatment is well known as the best solution to prevent spread of HCV infection in end-stage renal disease (ESRD) patients. We assessed the prevalence of anti-HCV antibodies in our PD and HD pts.
Methods: We enrolled 49 PD patients (25 men, 24 women; mean age: 47 years; mean duration of PD: 20 months) and 168 HD patients (100 men, 68 women; mean age: 54.7 years; mean duration of HD: 101 months) in the study. PD was the first-choice treatment in 32 patients (65%). Records and past history of blood transfusion and HD were reviewed. The presence of anti-HCV was determined by ELISA.
Results: Anti-HCV prevalence was 26.5% in PD patients and 61% in HD patients. In the subgroup of PD patients in whom PD was the first-choice treatment, anti-HCV positivity was significantly lower than it was in the subgroup of PD patients with a history of intermittent HD (1.28% vs. 52.9%, p<0.00).
Conclusions: PD offers significantly lower risk of infection with HCV among dialysis patients. PD should be considered as first-choice treatment of ESRD.
Stojkovski L., Dzekova P., Stojceva O., Selim G., Nephrology Clinic, Univer. Clinical Centre, Skopje, Macedonia.
[PP-286] Nephrologists’ Perception of PD in the Netherlands
It is known that about 50% of patients with stage 5 chronic kidney disease can be treated with peritoneal dialysis (PD). However, penetration of PD in the Netherlands has never been more than 30%. Currently, it has even decreased to less than 25%. Our aim was to visualize current obstacles to advising PD as first renal replacement therapy. Accordingly, we asked the opinion of nephrologists about how to tackle these problems.
Methods: A questionnaire was sent to Dutch nephrologists (n=277; 184 clinically active, 34 fellows). Questions were distributed by e-mail. The response rate was 35%.
Results: Medical contraindications (82%), impossibility to train the patient (62%), and unsuitable accommodation (42%) were most common reasons not to start with PD. Establishment of a nationwide registry of encapsulating peritoneal sclerosis [EPS (66%)], reducing the price difference between conventional and more biocompatible PD fluids (60%), and improving information and the education of patients and of nephrologists (both 53%) were the most frequently suggested improvements to PD. All nephrologists believed that their experience with PD was sufficient. Fears about EPS resulting from PD were held by 16%.
Of the 48 nephrologists who indicated that reducing the price difference between PD fluids would improve penetration of PD, 58% did not believe that unrestrained expansion of the capacity of center HD should be discouraged. Establishment of a nationwide registry of EPS (77%) and improvement in the information and education of patients (63%) and of nephrologists (60%) were important factors for improving PD. This group also found the development of a guideline for monitoring peritoneal function important (65%; 51% of all respondents).
Conclusions: Medical, psychosocial, and logistic problems are main reasons nephrologists do not choose PD. There is room for improvement of information and education. A nationwide registry of EPS is warranted. The development of a guideline for monitoring peritoneal function was regarded to be important. Financial issues are likely to be involved in modality choice.
Coester A.1, Krediet R.1, Boeschoten E.1, Dept. of Internal Med.,1 Div. Nephrol., Academic Med. Ctr., Univer. of Amsterdam, and Hans Mak Inst.,2 Naarden, Netherlands.