
Abstract

[PP-320] Hypercalciuria and Recurrent Urinary Tract Infections among Children in Zahedan, Southeast Iran
Background: Idiopathic hypercalciuria is a common metabolic abnormality in children of all ages. There is evidence of an association of idiopathic hypercalciuria with urinary tract infection (UTI). We evaluated the association of idiopathic UTI and hypercalciuria in Iranian children.
Methods: We studied 70 children with episodes of UTI and 70 healthy controls. We measured random urine calcium–creatinine ratio (UCa/Cr) and plasma calcium.
Results: Hypercalciuria was found to be significantly higher (p<0.05) in UTI patients (30%) than in normal subjects (11.4%):
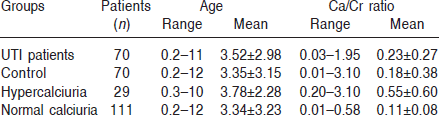
The results showed that frequency of hypercalciuria is higher in female (42.9%) than male (17.1%) children.
Conclusions: We suggest investigation of urinary calcium excretion in children with recurrent UTI.
Sadeghi–Bojd S.1, Hashemi M.2, Pediatic Nephrology1 and Biochemistry Dept.,2 Zahedan Univer. of Medical Sciences, Iran.
[PP-321] An Extraordinary Complication of PD in a Child, Demonstrated by CT Peritoneography
As the number of children on continuous ambulatory peritoneal dialysis (CAPD) increases, new, rarer complications are being recognized. Here, we report recurrent peritonitis in a 15-year-old girl with leakage of dialysis fluid from the peritoneum by the way of the Fallopian tubes to uterus and finally through the vagina without any detectable vaginal fistula being demonstrated by computed tomographic peritoneography.
Simsek B.1, Noyan A.1, Bayazit A.1, Inal M.2, Anarat A.1, Dept. of Pediatric Nephrology1 and Dept. of Radiology,2 Cukurova Univer., School of Medicine, Adana, Turkey.
[PP-322] Hydrothorax in Two Children on CAPD: Review of Clinical Approach and Treatment Options
Pleural effusions are relatively common in end-stage renal disease (ESRD) patients; on the other hand, hydrothorax secondary to pleuroperitoneal leak in continuous ambulatory peritoneal dialysis (CAPD) patients is rare. Because treatment modalities differ widely with regard to other causes of pleural effusion seen in CAPD patients (such as uremia, volume overload, congestive heart failure, infection, and malignancy), pleuroperitoneal leak should always be kept in mind in the differential diagnosis and should be excluded urgently. To draw attention to this point, we present a report on 2 children on CAPD who developed hydrothorax secondary to a pleuroperitoneal communication, and we provide an overview of diagnostic tools and treatment modalities.
Simsek B., Noyan A., Soran M., Bayazit A., Anarat A., Dept. of Pediatric Nephrology, Cukurova Univer., School of Medicine, Adana, Turkey.
[PP-323] Simultaneous Removal and Reinsertion of PD Catheter in Refractory Exit-Site Infection in a Child with Prune Belly Syndrome
The abdominal muscular defects in prune belly syndrome (PBS) are speculated to pose technical problems in achieving successful peritoneal dialysis (PD).
Case Report: An 11-year-old boy with PBS on long-term (7 years) automated PD had Staphylococcus aureus exit-site infection (ESI) refractory to antibiotic treatment. We describe a successful simultaneous removal and reinsertion of the PD catheter in this child in whom deficiency of abdominal musculature posed potential problems for use of this procedure.
During the operation, the new catheter was inserted into the opposite side of the abdomen before the old catheter was removed. The patient received appropriate antibiotic cover, given intravenously before the operation and continued for 7 days postoperatively. The child was temporarily switched to hemodialysis, and PD was resumed 2 weeks later. Early postoperative complications (fluid leakage, catheter anchorage) and ESI within 4 weeks after the operation were uncommon.
Our experience suggests that simultaneous removal and reinsertion of the PD catheter is feasible in eradicating refractory ESI in children with prune belly syndrome, without serious complications.
Sahpazova E.1, Petrovski M.2, Simeonov R.2, Kuzmanovska D.1, Pediatric Clinic,1 Department of Nephrology, and Clinic of Pediatric Surgery,2 Skopje, Macedonia.
[PP-324] Prilocaine-Induced Methemoglobinemia in a Child with End Stage Renal Disease after Percutaneous PD Catheter Placement
Cyanosis caused by methemoglobinemia is a rare condition in pediatric patients. This condition may arise as a result of a genetic defect in red blood cell metabolism or hemoglobin structure, or it may be acquired following exposure to various oxidant drugs and toxins. Here, we report an acute cyanotic condition attributable to prilocaine-induced methemoglobinemia in a child after percutaneous peritoneal dialysis (PD) catheter placement.
Case Report: A 6-year-old girl with end-stage renal disease resulting from focal segmental glomerulosclerosis was admitted for percutaneous PD catheter placement. The process was performed under local anesthesia with prilocaine (Citanest 2%: AstraZeneca). Two hours later, the patient developed central and peripheral cyanosis without significant respiratory distress. Her body temperature was 37°C; heart rate, 98 beats/min; respiratory rate, 22 breaths/min; blood pressure, 90/60 mmHg; oxygen saturation, 76% (by peripheral transcutaneous pulse-oximetry) on room air. Although a non re-breather mask was placed immediately, no improvement of the child's color and oxygen saturation was observed. Echocardiographic and chest X-ray examinations were normal. Arterial blood gas analysis revealed that pH, PaO2 and PaCO2 were 7.35, 95 mmHg, and 27 mmHg respectively. Her hemoglobin level was 7.4 g/dL. Because central cyanosis and low oxygen saturation in conjunction with normal PaO2 level persisted, methemoglobinemia was suspected. Her methemoglobin concentration was then found to be 8.6% (normal range: 0%–2%). Packed red cells (10 mL/kg) were transfused. No specific treatment for methemoglobinemia was performed. The patient's oxygen saturation rose to 85% after transfusion and to 96% after 36 hours. At hour 48, the methemoglobin concentration was 1.2%.
After percutaneous catheter insertion, physicians should be aware of this rare complication of local anesthetics in patients with unexpected cyanosis.
Anil M., Bal A., Çakmak B., Anil A.B., Aksu N., Dept. of Pediatric Nephrology, Tepecik Teaching and Research Hosp., Izmir, Turkey.
[PP-325] Gram-Negative Peritonitis in Children Undergoing Chronic PD
Gram-negative peritonitis is a well-known risk factor for peritoneal failure in children undergoing chronic peritoneal dialysis (CPD). The present study describes the causative agents and their antibiotic sensitivity at our center, and also shows 3rd-day early initial response and final treatment outcome.
We observed a series of 31 episodes in 23 children (median age: 47 months; 11 boys; 16 in diapers; 1 with a vesicostomy). The micro-organisms isolated were Pseudomonas, 28%; Klebsiella, 20%; Acinetobacter, 17%; Escherichia coli, 14%; Enterobacter, 14%; and Serratia, 9%. Antibiotic sensitivity was ceftazidime, 91%; amikacin, 94%; cephalothin, 25%; imipenem, 97%; ciprofloxacin, 90%. Initial empiric treatment was vancomycin or cephalothin plus ceftazidime (treatment 1) in 24 episodes, and vancomycin plus amikacin (treatment 2) in 7 cases. Early treatment response (3rd day) was evaluated by the Disease Severity Score. Improvement was found in 15/24 episodes (72%) with treatment 1 and in 6/7 episodes (86%) with treatment 2. Final outcome showed that it was possible to continue PD after 26/31 episodes, but in 5 cases continuation was not possible because of ultrafiltration failure or development of plastic peritonitis. Ten catheters were removed: 7 because of relapse, and 3 because of Candida peritonitis. Fifty percent of relapses and removals followed Pseudomonas peritonitis.
Conclusions: Pseudomonas peritonitis tended to be associated with greater number of relapses and catheter removal. Because the final outcome in gram-negative peritonitis in children is influenced by initial treatment response, it seems reasonable to initiate empiric treatment with amikacin associated with vancomycin or cephalothin, although our sensitivity in vitro for ceftazidime is higher than that seen in other centers. More cases should be included in further studies to make a change in the empiric initial treatment.
Adragna M.S., Hernandez C., Mosquera V., Grosman M., Hernandez M.G., Blanco A., Sojo E., Servicio de Nefrología, Hosp. de Pediatría J.P. Garrahan, Buenos Aires, Argentina.
[PP-326] Psychopathology of Children on PD: Effect of Residual Urine Volume on Anxiety
In a few studies of adults on chronic peritoneal dialysis (PD), depression and anxiety (D&A) have been reported to be correlated with anemia, malnutrition, inadequate dialysis, and peritonitis episodes. In the present study, we investigated D&A in children on PD and analyzed their relationship with morbidity.
We included 46 children on PD (23 girls; age range: 9–16 years) and a control group of 41 healthy children matched for age and sex. Psychopathologic assessment used the Child Depression Inventory and the Trait and State Anxiety Scale. Age of patients (pts), duration of PD, number of peritonitis episodes per pt, hypervolemia, hypertension, anemia, hyperparathyroidism, adherence to therapy, ultrafiltration (UF), and residual urine volume (RUV) were recorded.
Mean age was 12.8±2.03 years (pts) and 12.9±2.03 years (controls). Median PD duration was 20 months; daily UF, 1400 mL; and daily RUV, 750 mL. Depression scores of PD pts were significantly higher than those of healthy children (11.12±6 vs. 2.5±0.37, p=0.000). Similarly, anxiety scores of PD pts were significantly higher than those of controls (state anxiety score: 32.2±5.8 vs. 24.4±0.41, p=0.000; trait anxiety score: 33.8 ±1.07 vs. 24.8 ±2.5, p=0.000).
RUV was negatively correlated with state anxiety (r=-0.38, p=0.013). No correlations were found between age, dialysis duration, peritonitis episodes, or UF and levels of depression or anxiety (state or trait). D&A scores (state and trait) of pts who had hypervolemia (n=5), hypertension (n=14), anemia (n=15), and hyperparathyroidism (n=10) were similar to those of pts who did not have those problems (n=16; p=0.91, p=0.78, and p=0.12 respectively).
D&A are common among children on PD. Preservation of RUV may be beneficial in decreasing anxiety in this population.
Akman S.1, Fettahoglu Ç.2, Sever L.3, Aksu N.4, Ekim M.5, Bakkaloglu S.6, Poyrazoglu H.7, Noyan A.8, Özçakar B.5, Fidan K.6, Koyun M.1, Dept. of Pediatric Nephrol.1 and Dept. of Pediatric Psychiatri,2 Akdeniz Univer.; Dept. of Pediatric Nephrol.,3 Istanbul Univer.; Dept. of Pediatric Nephrol.,4 Tepecik Res. and Training Hosp.; Dept. of Pediatric Nephrol.,5 Ankara Univer.; Dept. of Pediatric Nephrol.,6 Gazi Univer.; Dept. of Pediatric Nephrol.,7 Erciyes Univer.; Dept. of Pediatric Nephrol.y,8 Çukurova Univer., Turkey.
[PP-327] Modified Short Peritoneal Equilibration Test in South African Children on PD
Background: Because of financial constraints, we have been doing short peritoneal equilibration tests (PETs) in our children on peritoneal dialysis (PD). In this test, a single blood test is taken at 2 hours, and dialysate samples are taken at 2 and 4 hours. At the same time, weekly Kt/V and creatinine clearances are calculated.
Methods: Retrospective evaluation of PET data obtained from 21 children receiving PD in a single center. A 4-hour modified short PET was performed in each patient after about 1 month on PD. The fill volume was 1100 mL/m2 body surface area (BSA) of 2.5% glucose solution. BSA was estimated by the method of Gehan and George. Blood samples for creatinine were taken at 2 hours, and dialysate samples for creatinine were taken only at 2 hours and 4 hours. The dialysate-to-plasma (D/P) ratio for creatinine was determined at 2 and 4 hours and was plotted on reference curves by Warady. Weekly Kt/V and creatinine clearance were also calculated using the Mellits– Cheek formulas for total body water.
Results: We audited results for 21 patients. Average age was 113 months (range: 15–192 months). Of the 21 children, 8 were high, 7 were high-average, 3 were low, and 3 were low-average transporters. Mean dialytic Kt/V was 2.54±0.6. Mean creatinine clearance per 1.73 m2 BSA was 67±20.
Conclusions: South African children on PD are high or high-average transporters in most cases. Adequate clearances were achieved in most cases.
Nourse P., Gajjar P., Mcculloch M., Red Cross and Tygerberg Children's Hosp., Dept. of Paediatric Nephrology, Cape Town, South Africa.
[PP-328] Outcome of Long-Term Peritoneal Dialysis in Infants
Peritoneal dialysis (PD) is the major choice of treatment for infants with end-stage renal disease. The complications and mortality rates are higher in infants than in older children. We evaluated the course and outcome of children starting PD before 1 year of age and compared the results with results in older children.
We retrospectively evaluated 22 infants (≤1 year of age) who were taken into a long-term PD program at a single center from 1999. The control group consisted of 22 children (>1 year of age) who started PD consecutively to the index cases. Outcome and complications were noted. Mann– Whitney U-test was used for statistical analysis.
In infants, median age was 0.36 year (range: 0.01–1.07 year), and mean weight at the start was 5.3 kg (range: 2.3–10.9 kg). Duration of PD was 11.7 months (range: 1.0–81.4 months months). Nine infants continue to receive PD, 12 died, and 1 was switched to hemodialysis (HD). Causes of death were sepsis in 6, heart failure (with congenital heart disease) in 3, pneumonia in 2, and unknown causes in 1. In the control group, median age at the start was 11.54 years (range: 6.60–15.85 years). Median PD duration was 31.1 months (4.7–81.8 months). Eleven children continue to receive PD, 6 switched to HD, and 5 received renal transplants in this group. The peritonitis rate was 1.4 episodes and 0.5 episodes per patient–year in the study group and control group respectively (p=0.03). There were no significant differences in exit-site and tunnel infections and catheter-related complications, including dialysate leak and hernia, between the two groups. The number of replaced catheters was 0.9 and 0.4 per patient–year in study group and control group respectively (p<0.001).
As compared with older children, infants receiving PD have greater risk of infection and a higher mortality rate; hence, intensive care should be provided by both the family and the medical team.
Canpolat N.1, Sever L.1, Caliskan S.1, Candan C.1, Civilibal M.1, Pehlivan G.1, Emir H.2, Arisoy N.1, Dept. of Pediatric Nephrology1 and Dept. of Pediatric Urology,2 Istanbul Univer. Cerrahpasa Medical Faculty, Turkey.
[PP-329] Five Years’ Experience with PD in Children in Belarus
Objectives: To review the incidence and causes of renal replacement therapy (RRT) and mortality of end-stage renal disease (ESRD) and acute renal failure (ARF) in children in Belarus.
Methods: The case records of 69 children (age: 10.97±4.43 years) diagnosed with ESRD from 1997 to 2008 and of 80 children (age: 11.33±7.32 years) diagnosed with ARF from 2005 to 2008 were reviewed.
Results: The principal cause of ESRD in children on dialysis was obstructive uropathy (29%); less-frequent causes included glomerulonephritis (14.5%) and renal aplasia/dysplasia/hypoplasia (13%). The initial method of treatment was hemodialysis (HD) in 42 patients (since 1997) and peritoneal dialysis (PD) in 30 patients (since 2002). Until 2002, all children under 7 years of age who had ESRD died. In 2007, PD was started in 23 pts [9 on automated PD (APD),14 continuous ambulatory PD (CAPD)] and HD in only 12. Children on PD were significantly younger than children on HD (8.68±5.26 years vs. 12.63±2.59 years, p<0.005). Mortality on RRT was 17.4% (6 on HD, 3 transplanted, 3 on PD). Hemolytic uremic syndrome [HUS; 57 pts (71.25%)] was the major cause of ARF; 13 pts (16.25%) had acute glomerulonephritis, and 4 pts (5%) had obstructive uropathy. In 2007, the basic RRT method for ARF was PD in 74% of cases (16% CAPD, 58% APD). Until 2005, the only method of RRT was HD. Using PD in children with ARF has considerably reduced mortality (to 3.75% in 2005–2007 from 22.1% in 2004, p<0.001).
Conclusions: The main causes of ESRD in children are still congenital and hereditary renal disease and the leading method of RRT is PD. The main cause of ARF requiring the use of RRT is still HUS. Using acute PD in children with ARF has led to considerably reduced mortality for the last 3 years.
Baiko S.V., Soukalo A.V., Hrushko I., Republican Ctr. of Children's Nephrology and Dialysis, Belarus.
[PP-330] Experience with Statin Use in Children Receiving PD
Dyslipidemia is a well-known risk factor for atherosclerosis in patients with end-stage renal disease (ESRD). The guidelines recommend treatment of dyslipidemia in adult and adolescent patients. To our knowledge, no data are available on statin use in children with ESRD. In this retrospective study, we evaluated the effects of statin therapy on lipid and lipoprotein parameters and potential adverse effects on liver and muscle enzyme levels in children receiving peritoneal dialysis (PD).
The study included 15 children on PD who had elevated levels of total cholesterol (TC>200 mg/dL) or low-density lipoprotein cholesterol (LDL-C>130 mg/dL) and who were treated with statins (atorvastatin 5–10 mg, or simvastatin 10 mg daily) for 6–12 months. Levels of serum triglycerides (TG), TC, LDL-C, and high-density lipoprotein cholesterol (HDL-C) were documented at 2-month intervals during therapy and were compared using the Wilcoxon signed rank test. The same method was also used to test for alterations of serum alanine aminotransferase (AST), aspartate aminotransferase (ALT), and creatine phosphokinase (CPK) levels during therapy.
At the start of statin therapy, median age of the patients was 8.7 years (range: 4.0–19.6 years). Median duration of statin therapy was 11.2±2.6 months. After 6 months of therapy, there were significant reductions in median values of LDL-C (48%), TC (25%), and TG (19%, all p<0.01). After 12 months of therapy, significant reductions were found for LDL-C (37.5%) and TC (26%, both p<0.01). There were no significant changes from baseline for AST, ALT, and CPK levels, and no case was complicated by myopathy.
The use of statins in pediatric PD patients with lipid disorders seems to be safe and efficient. Inthese children, randomized controlled trials are needed.
Canpolat N., Sever L., Civilibal M., Candan C., Caliskan S., Arisoy N., Dept. of Pediatric Nephrology, Istanbul Univer. Cerrahpasa Medical Faculty, Turkey.
[PP-331] Laparoscopic Omental Folding: A New Procedure to Prevent Omental Wrapping of Continuous PD Catheters
Objectives: Omental wrapping is a common cause of catheter obstruction in continuous ambulatory peritoneal dialysis (CAPD). We describe a new procedure to prevent omental wrapping.
Methods: Pneumoperitoneum at 9 mmHg was induced under general anesthesia. Two 3-mm ports and one 5-mm port was used. The omentum was then folded onto itself with intracorporeal suturing. A double-cuffed catheter was pulled through into abdominal cavity through a trocar site, and positioned. Peritoneal dialysis was initiated immediately after surgery.
Results: Four boys with end-stage renal disease were underwent laparoscopic omental folding and catheter placement. The operating time averaged 35 minutes. No intraoperative complications occurred. All catheters functioned well postoperatively. One patient had minimal port-site leakage of dialysate, which managed conservatively. After a median follow-up of 9 months, the results revealed no catheter malfunction or abdominal complications.
Conclusions: Omental folding is a safe, simple, and effective technique, which can be chosen instead of omentectomy to prevent omental wrapping.
Kaya M.1, Soran M.2, Boleken M.E.1, Yücesan S.1, Dept. of Pediatric Surgery1 and Dept. of Pediatric Nephrology,2 Harran Univer., Sanliurfa, Turkey.
[PP-332] Bone Mineral Density in Patients on PD and in Renal Recipients: A Follow-Up Study in Adolescents
Metabolic bone disease is common in patients with chronic renal failure. In children, those skeletal effects may result in serious impairment of bone growth and bone formation. The purpose of the present longitudinal study was to assess change of bone mineral density (BMD) in patients who underwent renal transplantation (RT) and in patients on peritoneal dialysis (PD).
The study included 33 children and adolescents (16 PD, 17 RT). At visits 1 and 2, regular biochemistry, anthropometry, and bone density were measured. In 15 patients (45%), height was below the 10th percentile. To minimize the effect of skeletal size, bone mineral apparent density (BMAD, in grams per cubic centimeter) was calculated. The results showed an increase, not statistically significant, in spine, femur, and total body BMD between the two measurements. However BMD in distal radius was significantly decreased in both groups of patients (p<0.01). The significant predictors of bone density change between two measurements were parathyroid hormone (p<0.05) and serum Ca (p<0.0001).
Our results suggest that bone loss resulting from renal failure cannot be fully recovered after successful renal transplantation. Cortical bone loss may be associated with hyperparathyroidism, which is the prominent biochemical deviation in patients with renal failure.
Slavicek J.1, Karacic I.1, Puretic Z.1, Kes P.1, Cvijetic S.2, Dialysis Dept.1, UHC Zagreb, and Inst. for Medical Research and Occupational Health,2 Zagreb, Croatia.
[PP-333] Low Quality of Life Scores Are Associated with Higher Complication Rates in Children on PD
There is a little information on quality of life (QOL) in children with chronic renal disease. We investigated QOL and its relationship with morbidity in children on chronic peritoneal dialysis (PD).
We included 53 children (28 girls; age: 9–15 years) in the study. A cross-sectional assessment of health-related QOL for physical, emotional, social, and school domains was performed using the PedsQL Generic Core Scale. Higher scores indicate better health-related QOL. Age, sex, PD duration, PD modality, peritonitis episodes, clinical complications, adherence to therapy, ultrafiltration (UF), and residual urine volume (RUV) were recorded.
Mean age of the patients (pts) was 12.1±2 years, and median PD duration was 20 months (range: 1–119 months). Median daily UF was 350 mL (range: 0–800 mL), and RUV was 200 mL (range: 0–1500 mL). Means of physical, emotional, social, and school domain scores were 63.6±26.1, 71.4±19.3, 73.8±25.3, and 65.8±26 respectively. In the emotional and physical domains, boys had higher QOL scores than did girls (p=0.001 and p=0.018 respectively). Duration of PD was negatively correlated with the emotional domain score (p=0.035, r=-0.32). Those results demonstrate significantly higher complication rates, including anemia, hypervolemia, hypertension, and hyperparathyroidism in the low-scoring pts as compared with the high-scoring pts on the physical and social domains (p=0.004 and p=0.046 respectively). Adherence to treatment was positively correlated with QOL score in the physical, social, and school domains (p=0.006, p=0.016, and p=0.022 respectively). No association was found between QOL score and age, PD modality, peritonitis episodes, RUV, or UF volume.
A low QOL score is associated with higher complication rates and lower compliance. Female sex and long-duration on PD may be additional risk factors for a low QOL score in children.
Akman S.1, Fettahoglu Ç.2, Sever L.3, Aksu N.4, Ekim M.5, Bakkaloglu S.6, Poyrazoglu H.7, Noyan A.8, Koyun M.1, Ωzcakar B.5, Fidan K.6, Dept. of Pediatric Nephrol.1 and Dept. of Pediatric Psychiatri,2 Akdeniz U.; Dept. of Pediatric Nephrol.,3 Istanbul U.; Dept. of Pediatric Nephrol.,4 Tepecik Res. and Training Hosp.; Dept. of Pediatric Nephrol.,5 Ankara U.; Dept. of Pediatric Nephrol.,6 Gazi U.; Dept. of Pediatric Nephrol.,7 Erciyes U.; and Dept. of Pediatric Nephrol.,8 Çukurova U., Turkey.
[PP-334] Psycho-Socioeconomic Status of Parents and Its Effects on Morbidity in Children on Chronic PD
In childhood, chronic peritoneal dialysis (PD) may be very distressing and tiresome for patients (pts) and parents (prs) alike. Reports on the psychological (psy) problems of prs are rare. We investigated psy problems of 44 prs (32 women; age: 28–53 years) and the relationship between those problems and morbidity in children and the socioeconomic status of the family.
Mean age of prs was 38.3±6.06 years and of pts, 12.1±2 years. A cross-sectional assessment of depression (DP), anxiety (ANX), anger, obsession–compulsion (O-C), and somatic symptoms (SOM) in prs was performed using the SCL-90-R. Lower scores indicate better psy status. We recorded duration of PD, PD modality, peritonitis episodes, clinical complications, adherence to therapy, ultrafiltration (UF), and residual urine volume (RUV) of the pts; age, sex, level of education, and income of the prs; and comfort of the home.
In pts, the medians of PD duration, daily UF, and RUV were 18 months (range: 1–108 months), 350 mL (range: 0–800 mL), and 280 mL (range: 0–800 mL) respectively. Mean scores for D P, ANX, anger, O-C, and SOM domains were 0.94±0.66, 0.75±0.66, 0.72±0.68, 1.07±0.58, and 0.91±0.61. Fathers had higher scores than did mothers on ANX and O-C domains (p=0.03, p=0.012). Adherence to treatment was negatively correlated with the O-C domain (p=0.009, r=-0.42). The results demonstrate significantly lower age of prs in the low-scoring as compared with high-scoring pts on the SOM domain (r=0.04, p=0.04). Comfort of the home was negatively correlated with DP and O-C scores. No association was found between psy problems of prs and age, PD modality, PD duration, peritonitis episodes, RUV, or UF in pts; or education or income of the family.
Better psy status of prs (low SCL-90 score) is associated with higher adherence to treatment. Male sex, older age, and an uncomfortable home may be additional risk factors for psychopathology of the pr.
Akman S.1, Fettahoglu Ç.2, Sever L.3, Aksu N.4, Ekim M.5, Bakkaloglu S.6, Poyrazoglu H.7, Noyan A.8, Fidan K.6, Koyun M.1, Ozcakar B.5, Dept. Pediatr. Nephrol.1 and Dept. Pediatr. Psychiatri,2 Akdeniz U.; Dept. Pediatr. Nephrol.,3 Istanbul U.; Dept. Pediatr. Nephrol.,4 Tepecik Res. and Training Hosp.; Dept. Pediatr. Nephrol.,5 Ankara U.; Dept. Pediatr. Nephrol.,6 Gazi U.; Dept. Pediatr. Nephrol.,7 Erciyes U.; and Dept. Pediatr. Nephrol.,8 Çukurova U., Turkey.
[PP-335] Extraosseous Calcification in an Adolescent Treated with Long-Term PD
Extraosseous calcification is an important complication of end-stage renal disease. The use of large doses of vitamin D and calcium-containing phosphate binders, hypercalcemia, hyperphosphatemia, elevated CaxP, parathyroid hormone, and duration of dialysis have been found to be associated with extraosseous calcifications. In this report, we describe a patient with soft-tissue calcification.
Case Report: A 17-year-old boy on continuous ambulatory peritoneal dialysis (CAPD) for 87 months was admitted to the hospital with bone pain. He had received erythropoietin, iron, antihypertensive drugs, calcitriol, and calcium-containing phosphate binder, but he was incompatible with his medication and had been followed by various centers for the preceding 2 years. He was pale and growth-retarded. He had fatigue and severe bone pain. Physical examination revealed hypertension, severe edema, pain in his extremities. Laboratory investigations found hemoglobin 5.4 g/dL, hematocrit 22%, serum urea 382 mg/dL, creatinine 9.8 mg/dL, albumin 3.1 g/dL, calcium 10.6 mg/dL, inorganic phosphorus 8.6 mg/dL, CaxP 91.1 mg2/dL2, parathyroid hormone 589 pg/mL (normal range: 9.5–75 pg/mL), C-reactive protein 5.6 mg/dL (normal range: 0–0.8 mg/dL). Radiographic examination of hands, legs, and feet revealed vessel-wall calcifications in the radial, ulnar, posterior, and anterior tibial arteries and their distal branches. Computed tomography revealed calcifications in the mitral valve, chordae tendinae, left coronary artery, abdominal aorta, and iliac arteries. He was transferred to hemodialysis with low dialysate calcium because of persistent ultrafiltration failure. Calcium-containing phosphate binder was changed to calcium-free phosphate binder. His complaints subsided, and his serum phosphorous level declined.
Soft-tissue and vascular calcifications can be seen in pediatric patients; these patients should therefore be regularly evaluated for extraosseous calcification development—especially patients on long-term PD.
Ekim M.1, Yuksel S.1, Fitoz S.2, Ozcakar Z.1, Acar B.1, Yalcinkaya F.1, Dept. of Pediatric Nephrology1 and Dept. of Radiodiagnostic,2 Ankara Univer., Ankara, Turkey.
[PP-336] Free and Acylcarnitine Levels and Cardiac Function in Pediatric CPD Patients
Patients (pts) on dialysis have been shown to be carnitine (CRN)– deficient. We evaluated acylcarnitine profile and relationships between CRN and cardiac function and plasma lipids in 96 pediatric chronic peritoneal dialysis (PD) pts [50 on continuous ambulatory PD (CAPD),46 on automated PD (APD); age: 13.6±4.9 years; PD duration: 27±25 months (range: 3–108 months)] and in 25 healthy age-and sex-matched controls. Besides routine biochemical parameters, hemogram, ferritin, parathormone and CRN fractions were measured and echocardiography was done.
Free, acetyl-l, and propionyl-l CRN were lower (25±23 μmol vs. 33±13 μmol, 14±8 μmol vs. 20±12 μmol, and 0.7±0.5 μmol vs. 1.7±0.8 μmol/L) and glutarylcarnitine was higher (0.4±0.3 μmol/L vs. 0.06±0.04 μmol/L) in PD pts. APD and CAPD pts had similar age and CRN levels. Pts in different peritoneal equilibration test groups had also similar CRN levels. CRN and hemoglobin, albumin, and Kt/V urea showed no correlations. Acetyl-l-CRN was positively correlated with triglycerides (r=0.222, p=0.037). Glutarylcarnitine was correlated negatively with glomerular filtration rate (r=-0.480, p=0.000) and positively with PD duration (r=0.204, p=0.050), uric acid (0.244, p=0.024), P (r=0.415, p=0.000), and daily dialysate glucose concentration (r=0.286, p=0.007). Systolic and diastolic cardiac dysfunction were detected in pts. Acetyl-l, propionyl-l, and glutarylcarnitine levels were positively correlated with isovolumic relaxation time (r=0.267, p=0.014; r=0.262, p=0.039; and r=0.222, p=0.039 respectively).
Our cross-sectional data showed that pediatric CPD pts are CRN-deficient. l-CRN supplementation and its potential beneficial effect on cardiac dysfunction should be evaluated in longitudinal studies.
Bakkaloglu S.A.1, Aksu N.2, Noyan A.3, Akman S.4, Ekim M.5, Sever L.6, Saygili A.7, Doganay B.8, Biberoglu G.9, Genc Derin B.9, Yildiz N.10, Duzova A.11, Soylu A.12, Akalin F.13, Dept. Ped. Nephrol.,1 Gazi U.; Div. Ped. Nephrol.,2 Tepecik Teaching Hosp.; Dept. Ped. Nephrol.,3 Cukurova U.; Dept. Ped. Nephrol.,4 Akdeniz U.; Dept. Ped. Nephrol.,5 Ankara U.; Dept. Ped. Nephrol.,6 Ýstanbul U.; Dept. Ped. Cardiol.,7 Gazi U.; Dept. Biostatistics,8 Ankara U.; Dept. Ped. Metab.,9 Gazi U.; Div. Ped. Nephrol.,10 Göztepe Teaching Hosp.; Dept. Ped. Nephrol.,11 Hacettepe U.; Dept. Ped. Nephrol.,12 Dokuz Eylül U.; Dept. Ped. Cardiol.,13 Marmara U., Turkey.
[PP-337] Topical Treatment of Peritoneal Catheter Exit Site Granulomas in Pediatric Patients with Acetamidohexanoic Acid Ointment Combined with Gentamicin and Fusidic Acid
Exit-site acute lesions (ESALs) are very frequent in children on chronic peritoneal dialysis (CPD). They can lead to tunnel infections or peritonitis. Exuberant granulation tissue or granulomas around the exit or in the sinus are often seen during acute infections or they appear related to micro-traumas. They are generally cauterized with a silver nitrate stick, but this treatment can lead to damage of the adjacent epithelium.
Acetamidohexanoic acid (AA) in combination with gentamicin (G) in ointment is used to treat skin ulcers (5 g AA and 0.1 g G in 100 g ointment). The ointment has healing and antibiotic properties and is safe for healthy skin and plastic elements. We evaluated the effectiveness of this ointment combined with a fusidic acid (FA) cream (2 g FA in 100 g cream) to treat granulomas.
Between January 2005 and January 2008, we recorded 16 ESALs (14 equivocal, 2 acute infection) in 18 pediatric patients on CPD [9 girls; median age: 10.2 years (range: 1–20.7 years); mean CPD duration: 22.4 months (range: 3–43 months); 14 granulomas]. Ointment was administered twice daily to the ESALs. In the acutely infected exit-sites, oral antibiotics were added. Patients were re-evaluated after 1 week and 1 month.
Of the 14 granulomas, 11 (79%) disappeared within a maximum of 30 days; only 3 had to be cauterized with silver nitrate stick because of incomplete resolution with the topical treatment. No ESAL led to chronic exit-site infection, peritonitis, or cuff infection. No damage of the healthy skin or peritoneal catheter was found.
Topical ointment (AA combined with G) and FA cream was effective and safe for exit-site granuloma treatment in children.
Coccia P.A.1, Mendoza L.E.1, Musso C.G.2, Ferraris J.R.1, Ramirez J.A.1, Service of Pediatric Nephrology1 and Service of Nephrology,2 Hosp. Italiano Buenos Aires, Argentina.
[PP-338] a Recent Experience of Pediatric Acute PD in a Developing Country
Objectives: To assess the modality of acute peritoneal dialysis (PD) performed in children admitted to the intensive care unit (ICU) at our center.
Methods: We retrospectively evaluated the data for children who received PD in the ICU between January 2004 and September 2007. The anthropometric values, causative factors, dialysis details, laboratory findings, medications, involvement of other organs, and outcomes were recorded.
Results: PD was administered to 14 children (8 boys, 6 girls; 3 days to 14 years of age, including 7 premature infants, of whom 3 had very low birth weights). Mean duration in ICU before renal replacement was 6.61±5.14 days (range: 0–17 days). Mean duration of continuous PD was 164.84±109.95 hours (range: 40–396 hours). All patients, except for 1 full-term neonate, had some PD complications including fluid retention, overfiltration, leakage, catheter revision, or peritonitis. Eleven of the patients were oligoanuric and needed pressors. Half had an electrolyte imbalance during PD, and 11 had at least a doubling in serum creatinine level. Each patient had complications associated with the type of dialysis modality and catheters, but none solely led to mortality. One patient received both PD and intermittent hemodialysis upon vancomycin toxicity, which improved without hearing loss. All 3 very low birth-weight infants received PD via peripheral venous catheters. The 3 survivors received short-term PD, and 2 needed no pressors.
Conclusions: PD is still an encouraging, easily performed renal replacement therapy for acute renal failure, especially in small children. It is even accessible in very low birth-weight infants through simple catheters. Sharing recent clinical experiences may encourage PD use when other techniques are not available.
Kasap B.1, Türkmen M.A.1, Soylu A.1, Akan M.2, Hazan E.3, Köroglu T.4, Duman N.5, Kavukcu S.1, Dept. of Pediatrics,1 Div. of Nephrology; Dept. of Anesthesiology and Reanimation2; Dept. of Cardiovascular Surgery3; Div. of Pediatric Intensive Care Unit4 and Div. of Neonatology,5 Dept. of Pediatrics, Turkey.
[PP-339] Malnutrition and Inflammation in Children on Chronic Peritoneal Dialysis
We prospectively evaluated nutrition status and inflammation in children on chronic peritoneal dialysis (CPD).
Our study included 30 children (16 girls, 14 boys) on CPD. Patients’ nutrition status was evaluated according to anthropometric parameters and body composition assessed by measurement of skinfold thickness and body mass index (BMI). Inflammation was measured by C-reactive protein (CRP), ferritin, and albumin. Anthropometric parameters were compared with biochemical parameters, Kt/V values, duration of dialysis, and age at initiation to dialysis.
The mean age of the patients was 12.5±3.7 years (range: 7–20 years). Mean CRP concentration was 1.4±0.8 mg/dL, with 30% of patients presenting CRP levels above 0.5 mg/dL. Mean ferritin was 147.5±165.6 mg/dL (range: 8–786 mg/dL) and was above the normal reference values in 30% of patients. On the other hand, mean albumin was 3.7±0.4 g/dL, and 30% of patients presented serum albumin levels below 3.5 g/dL. There was no significant correlation between malnutrition and CRP (p>0.05). In a Standard Deviation Score (SDS) calculation for our patients, malnutrition was found in 53.3% for SDS calculated according to weight and in 73.3% for SDS calculated according to height. In our cases, Kt/V was found to be 2.2±0.8. There was a significant difference between Kt/V and malnutrition calculated for height according to age and to SDS for height (p<0.01). There was a significant decline in height SDS and weight SDS values for our patients in whom CPD was started before 10 years of age.
We concluded that malnutrition in pediatric patients cannot be evaluated using only one parameter. When evaluated with different parameters, the results obtained can be more reliable. We think that height–weight SDS and height for age is a more reliable parameter in these patients for evaluation of malnutrition.
Dönmez O., Aynaci D., Dept. of Pediatric Nephrology, Uludag Univer., Bursa, Turkey.
[PP-340] Control of Linear Height in Chronic Renal Failure Followed by PD
Normal growth in children involves an interaction between genetics, feeding, metabolism, and hormonal control. Growth retardation in children suffering from chronic kidney failure is an important finding. The growth retardation in chronic kidney failure is a result of electrolyte disorders, feeding disorders, hormonal and metabolic disorders, renal osteodystrophy, and chronic inflammation.
We evaluated data from the files of patients in the peritoneal dialysis (PD) program. None were using growth hormone. For patients started on PD, we studied their decimal age, body weight, height, and height standard deviation score (HSDS) values at the beginning and after the 1st and 2nd year of the treatment period.
For 43 patients under study (19 girls, 24 boys; mean age: 10.96±3.17 years), the average HSDS value was calculated as - 3.01 at the beginning. In year 2 of PD, the average HSDS was calculated as -3.61. The height improvement at year 1 of the treatment period (ΔHSDS1) was calculated as -0.22, and at year 2, ΔHSDS2 was -0.26. There were no statistical difference between those values.
Chronic kidney failure has an adverse effect on linear growth in children. It is believed that PD may have a positive effect on growth when applied effectively and sufficiently. In our research, follow-up of the patients in the PD program showed that the effect on growth was not adquate. This study shows that PD alone does not have a positive effect on height growth, and that these patients need exogenous growth hormone. However, it is very hard in Turkey to apply this treatment because of insurance problems.
Ergün H.1, Galip N.1, Özçakar Z.B.1, Köse K.2, Altugan F.a,1, Yalçinkaya F.1, Ekim M.1, Dept. of Pediatric Nephrology1 and Dept. of Biostatistics,2 Ankara Univer. School of Medicine, Ankara, Turkey.
[PP-341] Dialysis Catheter Infections and Peritonitis in Children Receiving CAPD with a Low-Cost, Multi-Exchange-Per-Bag Technique
Objectives: For financial reasons, we initiated a modified continuous ambulatory peritoneal dialysis (CAPD) protocol to utilize most of the dialysis fluid from a commercial double-bag system. Most children receive 4 exchanges daily. Children may use one 2-L bag of dialysis fluid for 2–4 exchanges, depending on dialysis fill volume, with flush-before-fill technique. The dialysis system is disconnected during the day for school attendance. The natural history related to catheter infection and peritonitis in children receiving this low-cost technique remain undefined.
Methods: We reviewed clinical aspects of dialysis catheter infections and peritonitis in children receiving peritoneal dialysis (PD) from May 1996 to December 2007.
Results: Of 28 children, 3 were on automated PD and 25 on CAPD. The CAPD children (mean age: 10.2±3.7 years) received dialysis treatment for 69.2 patient–years (mean duration: 2.8±1.9 years). There were 34 catheter-related infections (0.49 episode/patient–year) in 15 children (60%), and 56 episodes of peritonitis (0.81 episode/patient–year) in 14 children (56%). Staphylococcus aureus was the major causative organism [14 episodes (25%)]. Gram-negative bacteria grew in 24 episodes (42.9%), and 15 episodes (26.8%) were culture-negative. There was 1 episode of Candida peritonitis. The mean time from initiation of dialysis to the first episode of peritonitis was 8.2 months. A nasal culture for S. aureus is obtained at the start of dialysis. S. aureus nasal carriage was positive (NSA+) in 3 children (12%). Staphylococcus catheter infection and peritonitis were more frequent in NSA+ children (p<0.05).
At study end, 9 children remained on CAPD, 4 had been transferred to adult units, and 2 had been switched to hemodialysis. Seven children underwent kidney transplantation. The mortality rate was 12% (3/25), with no deaths related to peritonitis.
Conclusions: Incidence of peritonitis was 0.81 episode/patient–year. S. aureus was the major causative organism. Staphylococcus catheter infection and peritonitis were more frequent in NSA+ children.
Kingwatanakul P., Deekajorndech T., Dept. of Pediatrics, King Chulalongkorn Memorial Hosp., Faculty of Medicine, Chulalongkorn Univer., Bangkok, Thailand.
[PP-342] Candida Meningitis Secondary to PD-Related Peritonitis in a Child with Spina Bifida and Ventriculoperitoneal Shunt
In this case report, we emphasize infectious complications in children with spina bifida (SB) and ventriculoperitoneal shunt (VPS) treated with chronic peritoneal dialysis (PD).
Case Report: An 11-year-old PD patient with spina bifida and ventriculoperitoneal shunt presented with peritonitis symptoms. She had neuropathic bladder and chronic renal failure secondary to SB, and at the age of 7, she had been started on chronic PD. She had 4 peritonitis episodes in 38 months. Three episodes had been culture-negative, and 1 was caused by coagulase-negative Staphylococcus aureus. These peritonitis episodes were treated with cefazolin and ceftazidime and were not complicated by a shunt infection. On her last admission, this patient presented with a new peritonitis episode 10 months after the last peritonitis. Culture of the peritoneal fluid revealed Candida parapsilosis. Liposomal amphotericin B was added to the nonspecific antimicrobial treatment. As soon as the microorganism was identified, the peritoneal catheter was removed, and the girl was transferred to hemodialysis. The VPS was externalized because of the risk of an invasive fungal shunt infection. Culture of the cerebrospinal fluid (CSF) revealed C. parapsilosis, and the shunt was removed. C. parapsilosis was also isolated from the tip of the shunt catheter. Afterwards, the patient showed progressive neurologic deterioration and ventricular hydrocephaly. One week later, a new ventriculopleural shunt was placed. Treatment with amphotericin B continued for 5 weeks, and a control CSF culture was negative.
We conclude that PD is an effective renal replacement therapy for patients with SB. Although PD has been reported not to be contraindicated in children with myelomeningocele, regardless of the presence of a VPS, such a shunt makes PD more complicated. These children are prone to developing severe shunt infections secondary to PD-related peritonitis, as in our case.
Yildiz N.1, Turhan P.1, Erguven M.1, Tosyali N.2, Simav G.3, Dept. of Pediatric Nephrology,1 Dept. of Pediatric Surgery,2 and Dept. of Neurosurgery,3 Health Minister Goztepe Teaching Hosp., Istanbul, Turkey.
[PP-343] Homocysteine is an Important Marker of Cardiovascular Disease in Children on PD
Cardiovascular disease (CVD) mortality is a leading cause of death in adult chronic kidney disease. However, little information is available regarding cardiac risk factors in children with end-stage renal disease. Generally, carotid intima media thickness (IMT), left ventricular ejection fraction, and left ventricular mass index (LVMI) are routinely performed for definition of CVD. In the present study, we investigated levels of homocysteine, high-sensitivity C-reactive protein (hsCRP), von Willebrand factor, apolipoproteins A and B, lipoprotein(a), insulin resistance, and KtV urea as independent risk factors for IMT and LVMI in 14 pediatric chronic dialysis patients.
IMT was assessed by high-resolution ultrasound, and LVMI was calculated from standard echocardiographic measurements. All of the investigated risk factors were higher in patients than in controls (p<0.05). Stepwise regression analysis showed that homocysteine levels and blood pressure (systolic and diastolic) were independent variables for predicting IMT and LVMI (p<0.05 and p<0.01 respectively). There were positive correlations between LVMI and systolic and diastolic blood pressure (p<0.05). Also, there was a negative correlation between LVMI and hemoglobin (p<0.05). IMT was negatively correlated with homocysteine (p<0.05).
In conclusion, homocysteine seem to be the most useful marker for determination of cardiovascular risk in children treated with peritoneal dialysis. Our study suggests that hypertension and anemia should be better treated, because they may be priorities for preventing CVD in these patients.
Yildiz B.1, Kural N.1, Kilic Z.2, Akcar N.3, Baylan Z.1, Dept. of Pediatric Nephrology,1 Dept. of Pediatric Cardiology,2 and Dept. of Radiology,3 Eskisehir Osmangazi Univer., Faculty of Medicine, Eskisehir, Turkey.
[PP-344] the Effectiveness of a Preventive Protocol for Staphylococcus aureus Peritonitis in Children Receiving Long-Term PD
Objectives: Staphylococcus aureus (SA) remains the major organism causing dialysis catheter infection and peritonitis. We determined the effect of SA nasal carriage and a dialysis catheter infection treatment protocol for prevention of SA peritonitis in children.
Methods: Before initiation of chronic peritoneal dialysis (CPD), all children are tested for SA nasal carriage; intranasal mupirocin is prescribed for positive cases (NSA+). Topical mupirocin is also given to children who have exit-site infection (ESI). Oral antibiotics are used in children who do not respond to mupirocin or whose cultures grow gram-negative organisms. Tunnel infection (TI) was identified by ultrasonogram and treated with a 7-day course of intraperitoneal cefazolin. The data of children receiving CPD from May 1996 to December 2007 was reviewed for ESI, TI, and peritonitis.
Results: There were 28 children (age: 9.8±4.3 years) receiving CPD (duration: 2.7±1.8 years) during the study period. There were 37 ESIs or TIs (0.49 episode/patient–year) in 17 children (60.7%). SA remained the most common infecting organism [20/37 episodes (54.1%)]. There were 56 episodes of peritonitis (0.74 episode/patient–year) in 14 children (50%). SA was the major causative organism [14/56 episodes (25%)]. In 24 episodes of peritonitis (42.9%), cultures grew gram-negative organisms; 16 episodes (28.6%) were culture-negative. The mean time from initiation of CPD to first episode of peritonitis was 12.1 months. The annualized rate of peritonitis has declined to less than 0.5 episode/patient–year over the last 5 years, with only 1 episode of SA peritonitis. In 3 children (10.7%), tests showed NSA+. SA catheter infection and peritonitis were more frequent in NSA+ children (p<0.05). There was no correlation between ESI or TI and peritonitis.
Conclusions: Incidence of peritonitis in this study was 0.74 episode/ patient–year; the incidence declined sharply over the last 5 years. S. aureus was the major causative organism of ESI or TI and peritonitis, but the incidence of SA peritonitis has been decreasing.
Deekajorndech T., Kingwatanakul P., Dept. of Pediatrics, King Chulalongkorn Memorial Hosp., Faculty of Medicine, Chulalongkorn Univer., Bangkok, Thailand.
[PP-345] Quality Program in Peritoneal Dialysis in Children—7 Years’ Follow-Up
Objectives: To analyze the outcome of children on chronic peritoneal dialysis (PD) submitted to a systematic evaluation program.
Methods: Analysis of all patients on PD between July 2000 and July 2007, who performed at least 1 complete evaluation consisting of anthropometric measurements; blood pressure and cardiologic status; laboratory evaluations; peritoneal equilibration test; Kt/V; intraperitoneal pressure (IPP); occurrence of infections, hernias, or constipation; and need to change the catheter. We then compared all the evaluations, considering a p value <0.05 significant.
Results: At least 1 evaluation was available in 84 patients; 2 evaluations were available in 68; 3 in 38; and 4 in 21 (6 months between evaluations). Mean age of the patients at the beginning of dialysis was 8±2 years. A great number of patients were converted from continuous ambulatory PD to continuous cycling PD and nightly intermittent PD (NIPD); some had to increase daytime dwells. Anthropometric parameters remained stable over time. Most patients had hypertension at the first evaluation, without improvement during follow-up. Laboratory evaluations remained stable, but patients with residual renal function (RRF) had lower creatinine levels and improvement of hematocrit. Mean IPP was 11.9 cmH2O. It was significantly lower in small children (p=0.003) as compared with patients older than 7 years. There was no association between IPP and occurrence of hernia. There was no significant decrease in RRF in the patients with 4 evaluations, but it was significantly higher in PD patients as compared with patients transferred to hemodialysis earlier. Kt/V remained stable. There were 109 peritonitis episodes and 61 exit-site infections, 21 catheter exchanges, and 15 hernias. Over the study period, 40% of patients were transferred to hemodialysis, 30% were transplanted, 5% transferred to other centers, 6% died, and 19% remained on PD.
Conclusions: We observed a stable long-term outcome in our patients. Infection control and preservation of RRF are important points to be assessed with the aim of preserving the PD technique until transplant can be performed.
Sylvestre L.C., Souza J.F., Vargas E.T., Wladika E.I., Meneses R.P., Filho D.G., Pediatric Nephrology Dept., Hosp. Pequeno Principe, Curitiba, Brazil.