
Abstract
Background
Peritoneal dialysis (PD) is associated with functional and structural alterations of the peritoneal membrane, particularly new vessel formation and fibrosis. In addition to anticoagulant effects, heparin displays anti-inflammatory and angiostatic properties. Therefore, the effects of administration of heparins on function and morphology of the peritoneal membrane were studied in a rat PD model.
Methods
Rats received 10 mL conventional PD fluid (PDF) daily, with or without the addition of unfractionated heparin (UFH) or low molecular weight heparin (LMWH) in the PDF (1 mg/10 mL intraperitoneally) via a mini access port. Untreated rats served as controls. After 5 weeks, a 90-minute functional peritoneal transport test was performed and tissues and peritoneal leukocytes were taken.
Results
PD treatment induced loss of ultrafiltration (p < 0.01), a twofold increase in glucose absorption (p < 0.03), increased urea transport (p < 0.02), and loss of sodium sieving (p < 0.03), which were also found in the PDF + heparin groups. Increased peritoneal cell influx and hyaluronan production (p < 0.02) as well as an exchange of mast cells and eosinophils for neutrophils after PD treatment were observed in PD rats; addition of heparin did not affect those changes. Mesothelial regeneration, submesothelial blood vessel and matrix formation, and accumulation of tissue macrophages were seen in PD animals. Spindle-shaped vimentin-positive and cytokeratin-negative cells indicated either partial injury and denudation of mesothelial cells or epithelial-to-mesenchymal transition. Neither UFH nor LMWH affected any of these morphological changes.
Conclusion
Within 5 weeks, PD treatment induces a chronic inflammatory condition in the peritoneum, evidenced by high transport, leukocyte recruitment, tissue remodeling, and induction of spindle-shaped cells in the mesothelium. Addition of LMWH or UFH to the PDF did not prevent these adverse PDF-induced peritoneal changes.
Keywords
Heparin is a highly sulfated polysaccharide belonging to the glycosaminoglycan family and is synthesized by mast cells. Although it is most known for its anticoagulant effect, heparin has a number of immunomodulatory and anti-inflammatory activities, including binding of cytokines, chemokines, and growth factors (6). Earlier reports demonstrated that heparin can inhibit leukocyte rolling along the vessel wall, a process known to involve selectins (7,8). The function of selectins in this process depends on recognition of specific glycoprotein ligands. However, a variety of carbohydrate structures, including heparin, may bind these lectin-like molecules and interfere with ligand binding (9). In addition to unfractionated heparin (UFH), low molecular weight heparin (LMWH) is one of the most commonly used types of heparin in clinical settings. Fractions of LMWH are prepared from standard UFH and are similar to UFH in many aspects. The main advantages of this class of antithrombotic agent compared with UFH are improved bioavailability, prolonged half-life (which may permit one single daily subcutaneous injection), and improved efficacy (10,11).
In the clinical PD setting, heparin is used to prevent catheter obstruction and the formation of fibrin during peritonitis. Results of studies on the effects of intraperitoneal heparin administration on peritoneal transport and inflammation have been contradictory (12-16). Therefore, we studied the effects of long-term addition of UFH, as well as LMWH, to the PDF on function, defense, and tissue remodeling of the peritoneal membrane to determine whether heparin can improve peritoneal transport and whether it can also prevent morphological changes in peritoneal tissues. In the present study, either UFH or LMWH was added to the PDF for 5 weeks in a chronic peritoneal exposure model in the rat (17,18).
Material and Methods
Animals
Male Wistar rats (Harlan CPB, Horst, The Netherlands) weighing 250 – 275 g at the beginning of the experiment were used throughout the study. They were allowed 1 week of acclimatization before the start of the experiment. Animals were housed under conventional laboratory conditions and were given food and water ad libitum. The Animal Experimental Committee of the Vrije Universiteit of Amsterdam approved the experimental design.
Experimental Design
Fluids were instilled via a peritoneal catheter connected to an implanted subcutaneous mini access port, as previously described (19). Rats that were not surgically treated and received no fluid instillation served as the control group (n = 8). The rest of the animals (n = 34) received 2 mL saline with 1 IU/mL heparin to allow wound healing during the first week after their operation. Thereafter, during a 5-week period (20-23), rats were instilled daily with 10 mL standard PDF (Dianeal PD4, 3.86% glucose, pH 5.2; Baxter R&D, Utrecht, The Netherlands; PDF-control; n = 14), PDF with the addition of UFH (PDF-UFH; n = 10), or PDF with the addition of LMWH (nadroparin calcium; PDF-LMWH; n = 10). The concentrations used for UFH and LMWH (1 mg/rat/day: equivalent to 175 IU UFH/rat/day and 100 IU LMWH/rat/day) are consistent with the concentrations used in the clinical setting and proportional to the dose used in deep venous thrombosis prophylaxis in humans (24). To check whether the animals were not over-heparinized due to daily heparin administration, blood samples were taken after 4 weeks of treatment 3 hours after PDF + heparin instillition to measure APTT clotting times and anti-factor Xa levels. At the end of the experiment, a functional 90-minute peritoneal equilibrium test (PET) was performed (see below) under a mixture of fentanyl–fluanisone (0.05 mL/100 g) and midazolam (0.08 mL/100 g) anesthesia. After the animals were sacrificed, tissues and peritoneal leukocytes were taken to analyze functional, morphological, and cellular parameters.
Analysis of Peritoneal Cells and Effluents
After 5 weeks of treatment, a PET was performed by injecting 30 mL standard PDF into the peritoneal cavity via a direct intraperitoneal catheter (Venflon Pro; BD Medical Systems, Franklin Lakes, NJ, USA). After 90 minutes, the PDF was drained and ultrafiltration capacity was calculated. Cells were isolated by centrifugation and cell number, and viability was determined by trypan blue exclusion. Cytocentrifuge preparations were stained with May–Grünwald–Giemsa and cells were differentiated. After the PET, the animals were sacrificed and a cardiac puncture was performed. Glucose, sodium, creatinine, and urea concentrations were analyzed in serum samples and in the cell-free effluents at t = 90 minutes of the PET. At t = 0 and t = 45 minutes, sodium concentrations in the effluents were analyzed to measure sodium sieving. The amount of hyaluronic acid in the supernatant of the peritoneal effluent was determined using an ELISA-based assay according to Fosang et al. (25).
Morphologic Analysis
Mesentery and Omentum: A part of omental and mesenteric tissue was dissected and spread on a glass slide for fluorescence microscopic examination. Both tissues were stained with antibodies to CD31 (PECAM; Serotec, Oxford, United Kingdom) to visualize vasculature and to ED2 (Serotec) to visualize macrophages. As a negative control, conjugate controls (Invitrogen, Carlsbad, CA, USA) without the first antibody were used. Images were analyzed by computerized digital image analysis (AnalySIS; Soft Imaging System; Olympus, Hamburg, Germany). The areas positive for CD31 and ED2 were calculated as percentages of the total area of the tissue.
Parietal Peritoneum: The parietal peritoneum was taken at the contralateral side to the tip of the implanted catheter using a standardized method. Cryostat sections (7 μm) were cut and stained for CD31 and ED2. Images were analyzed by computerized digital image analysis and the areas positive for CD31 and ED2 were calculated as percentages of the total area of the submesothelial matrix layer. Frozen sections were also used to quantify fibrosis formation. The thickness of the submesothelial extracellular matrix was determined after Van Gieson staining (Merck, Darmstadt, Germany) as the mean of 10 independent measurements for each animal.
Liver Imprints: Imprints of the mesothelial monolayer of the liver were taken with 3% gelatin-coated slides according to a previously described method (26) and stained with May–Grünwald–Giemsa. Mesothelial cell density per 0.1 mm2 area was counted using a scored eyepiece; the mean of 15 areas was calculated for each slide and expressed as cells per square millimeter. Liver imprints were also stained for vimentin (Serotec) and cytokeratin (DakoCytomation, Glostrup, Denmark) to determine spindle-shaped cells that underwent EMT.
Statistical Analysis
All data are presented as median and interquartiles. The Kolmogorov–Smirnov test for normality showed that the groups were not normally distributed; therefore, differences between groups were analyzed using the nonparametric Mann–Whitney U-test. We made three comparisons, namely, control versus PDF-control, PDF-control versus PDF-UFH, and PDF-control versus PDF-LMWH. According to a Bonferroni correction, probability values of p < 0.03 were considered significant. Correlation analysis was performed using the nonparametric Spearman's rho test. Survival analysis was performed using the Kaplan–Meier method.
Results
During the experiment, the well-being of all animals was monitored daily and no apparent abnormalities were observed. Throughout the experiment a number of animals dropped out due to abdominal fat or omental tissue wrapping around the tip of the catheter, which was consistent with earlier experience (17,20). Although it was expected that heparin would impair fibrin formation and possibly prevent adhesion and omental wrapping, Kaplan–Meier survival analysis showed no differences in dropout rates (in time or in number) between the three treatment groups. Development of peritonitis during the experiment was very unlikely since there was no loss of body weight, the animals did not show any other clinical signs, and there were no abnormalities in neutrophil counts in peritoneal dialysates or in peritoneal tissues. After 5 weeks of fluid instillation, 8, 5, and 5 rats in the PDF-control, PDF-UFH, and PDF-LMWH groups, respectively, remained for analysis. All 8 control rats were used for the PET and morphologic analysis. APTT and anti-factor Xa measurements showed that daily intraperitoneal treatment with clinical concentrations of 1 mg/day heparin did not significantly influence clotting times 3 hours after heparin injection. Plasma anti-factor Xa levels were higher in the PDF-LMWH group compared to the control groups (p = 0.048). Although this difference was not significant, it indicated that heparin was administered in an adequate dose without over-heparinization of the animals.
Transport Parameters and Composition of Peritoneal Cells
Table 1 shows the transport parameters measured in the PET effluents at t = 90 minutes for all four groups. The PET in the control animals demonstrated a net ultrafiltration capacity of 8.6 mL per 90 minutes. Exposure to PDF reduced peritoneal performance significantly to a net ultrafiltration volume of 6.5 mL. Addition of UFH or LMWH further reduced the ultrafiltration capacity. In addition to the reduced net ultrafiltration capacity, PDF induced a significantly enhanced glucose absorption (p < 0.03) and an increased urea transport (p < 0.02). Sodium measurements at t = 0, t = 45, and t = 90 minutes of the PET showed a reduction in the sodium dip upon PDF treatment (control vs PDF-control at t = 90: p < 0.03). Addition of UFH or LMWH did not restore PDF-induced changes in peritoneal transport (Table 1).
Values of Peritoneal Transport Parameters Determined by Peritoneal Equilibrium Test
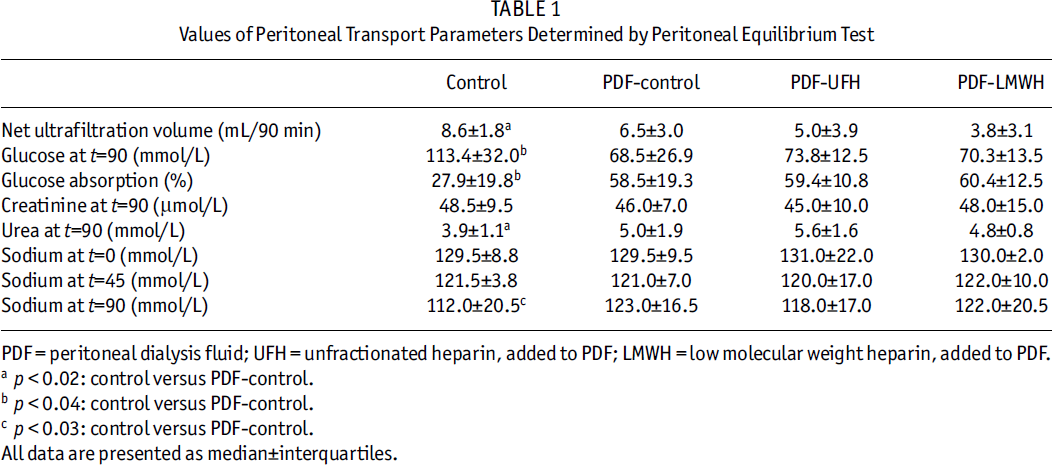
PDF = peritoneal dialysis fluid; UFH = unfractionated heparin, added to PDF; LMWH = low molecular weight heparin, added to PDF.
p < 0.02: control versus PDF-control.
p < 0.04: control versus PDF-control.
p < 0.03: control versus PDF-control.
All data are presented as median±interquartiles.
The total cell numbers and differentiation of peritoneal cells recovered from the PET dialysate are shown in Table 2. Significantly more cells were found in the peritoneal effluents of the three PDF-treated groups compared to the control animals (p < 0.02). No difference in cell numbers was seen between PDF-control and the heparin groups. Cell differentiation revealed an exchange of mast cells and eosinophils for neutrophils after PD treatment. Treatment with UFH as well as LMWH seemed to nearly abolish the PD-induced inflammation by reducing neutrophil recruitment. Furthermore, the addition of UFH or LMWH resulted in slightly reduced hyaluronan synthesis compared to the PDF-control group (Table 2).
Composition of Peritoneal Leukocytes and Hyaluronic Acid Synthesis
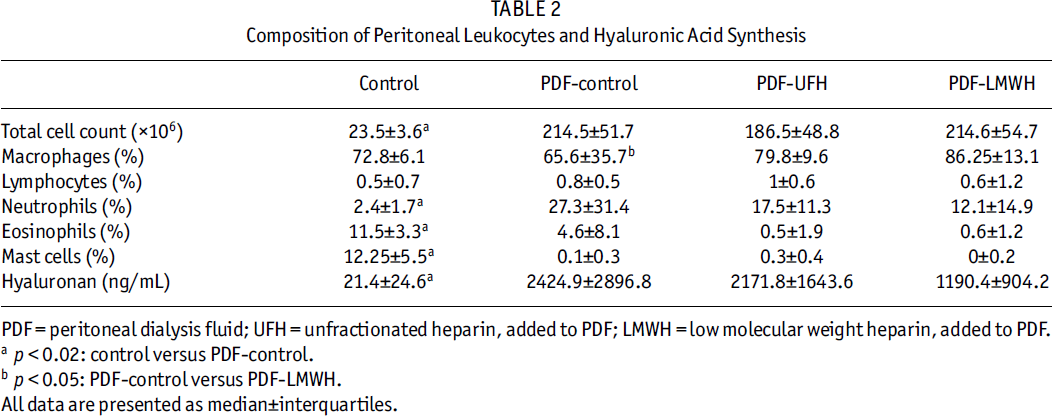
PDF = peritoneal dialysis fluid; UFH = unfractionated heparin, added to PDF; LMWH = low molecular weight heparin, added to PDF.
p < 0.02: control versus PDF-control.
p < 0.05: PDF-control versus PDF-LMWH.
All data are presented as median±interquartiles.
Morphological Changes
Mesentery and Omentum: All groups exposed to PDF showed a significant increase (p < 0.01) in accumulation of mature macrophages (ED2) and new blood vessel formation (CD31) compared to the control group (Figure 1). Neither UFH nor LMWH was able to prevent the increased density of macrophages and blood vessels seen in the mesentery and omentum. When all four groups were combined, the increased accumulation of macrophages was positively correlated to increased blood vessel density: r = 0. 64 and r = 0.89 for mesentery and omentum respectively; both p < 0.01.
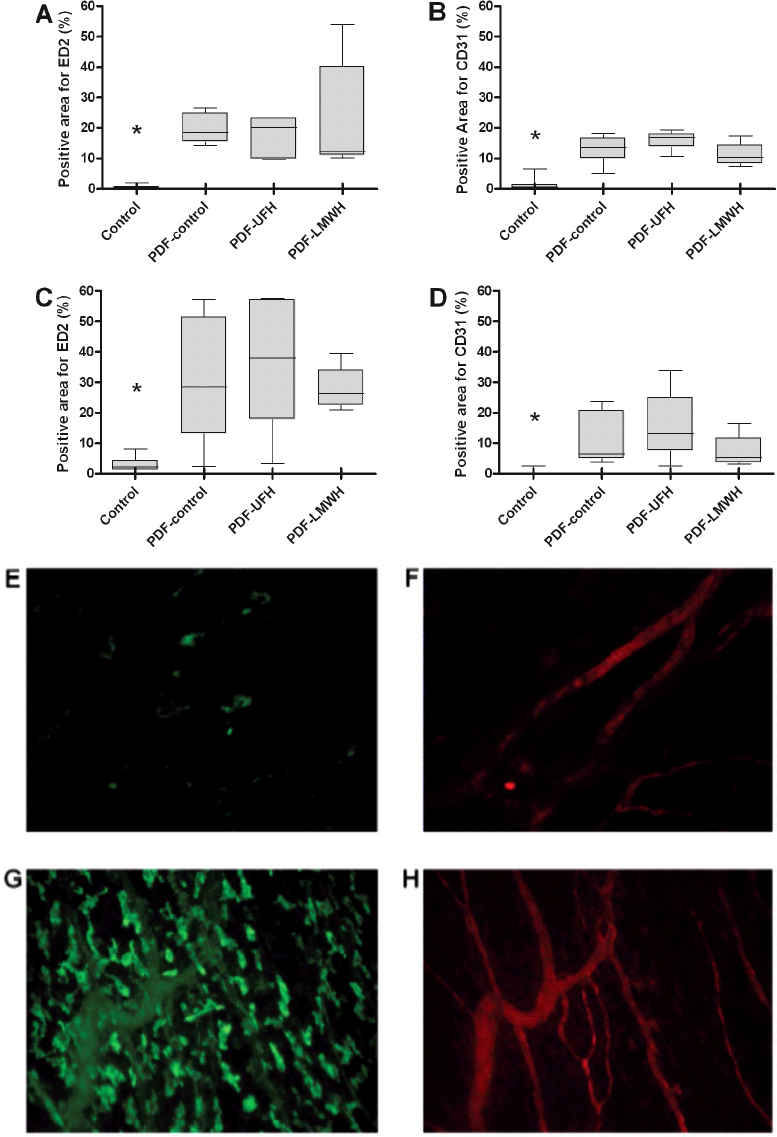
Macrophage and blood vessel density in mesentery and omentum. Percentage of area positive for macrophages (ED2) (A and C) and vessels (CD31) (B and D) in mesentery (A and B) and omentum (C and D).
Parietal Peritoneum: Frozen sections of the peritoneum were stained with Van Gieson to observe changes in the extracellular matrix underneath the mesothelial layer. Peritoneum taken from control animals showed thickness of extracellular matrix to be 8.4 ± 4.1 μm. Thickness was significantly increased (p < 0.01) in the peritoneum of animals of the PDF-control (14.7 ± 5.2 μm), PDF-UFH (12.4 ± 3.4 μm), and PDF-LMWH (12.8 ± 6.3 μm) groups [Figure 2(a)]. No differences were found between the PDF-treated groups. Sections of the peritoneum were also stained for CD31 and ED2. Similar to the morphological changes found in the mesentery and the omentum, significantly more macrophages and blood vessels were seen in the PDF-treated animals compared to the control group, with no differences between the three PDF-treated groups [Figures 2(b) to 2(g)]. Correlation analysis showed again a significant positive relation between increased macrophage accumulation and blood vessel density (r = 0.76, p < 0.01). Positive correlations were also found between matrix thickness and CD31 (r = 0.78, p < 0.01) and between matrix thickness and ED2 (r = 0.76, p < 0.01).
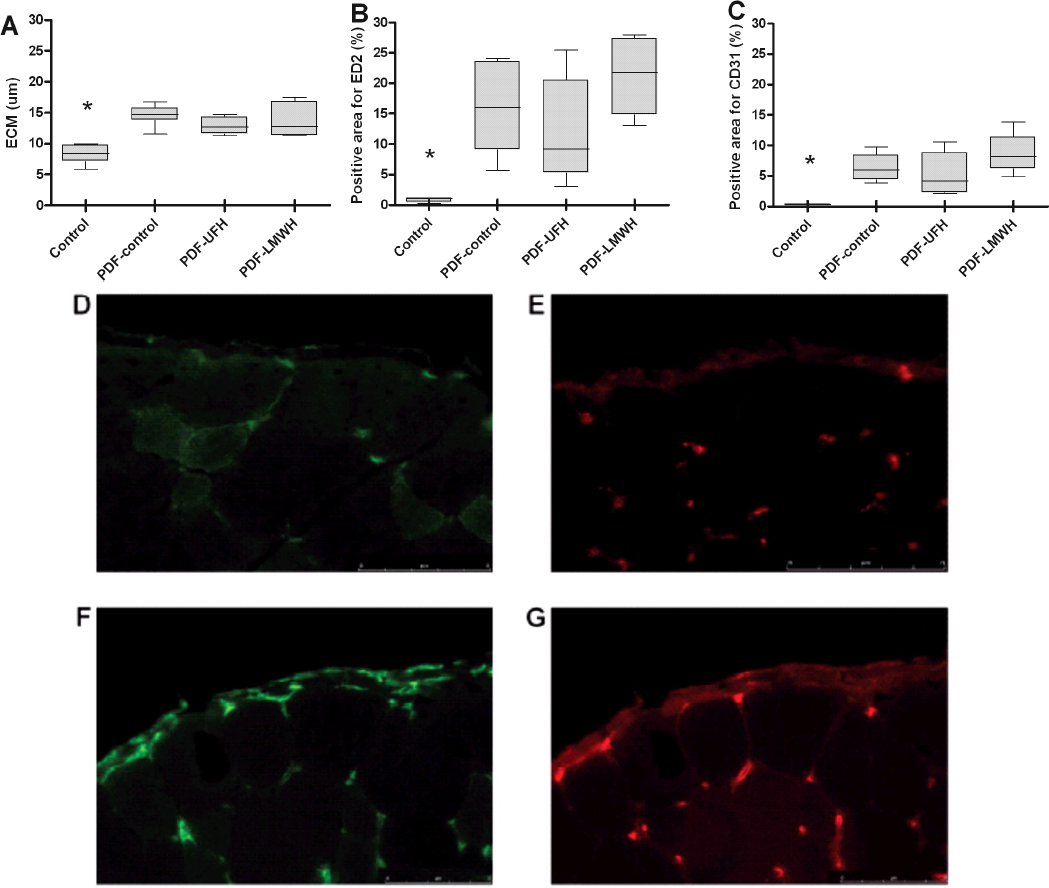
Morphology of parietal peritoneum. Ultrastructural measurements of the thickness of the abdominal submesothelial extracellular matrix (ECM) (A). Percentage of submesothelial layer positive for ED2 (B) and CD31 (C) in parietal peritoneum.
Liver Imprints: Mesothelial cell density was measured as a marker for mesothelial cell regeneration. The number of mesothelial cells on the liver showed a significant twofold increase (up to 2045 ± 1167 cells/mm2) in the PDF-control group compared to the untreated animals (1168 ± 273 cells/mm2, p < 0.01) [Figures 3(a) and 3(b)]. Neither of the two heparins was able to influence mesothelial cell regeneration. Spindle-shaped cells were found between mesothelial cells in PDF-treated animals [Figure 3(b)]. An average of 7% – 10% of the cells found on the liver imprints of PDF-treated animals showed this phenotype, whereas these cells were not found in control animals (p < 0.01). No differences in the numbers of spindle-shaped cell were found between the three PDF-exposed groups. Vimentin-positive and cytokeratin-negative staining [Figures 3(c) and 3(d)] identified those cells as fibroblast-like cells, indicating either that the imprint picked up submesothelial fibroblasts due to partial injury and denudation of mesothelial cells, or possibly mesothelial cells undergoing EMT [Figure 3(d)].
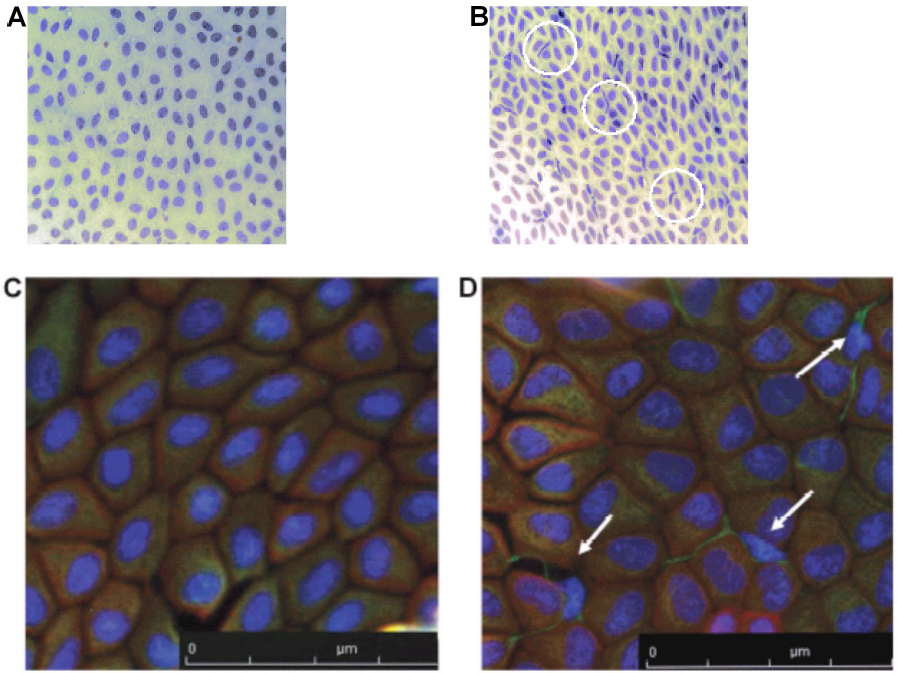
Morphology of the liver imprints. Representative example of mesothelial imprints of a control (A) and a PDF-treated (B) animal. Spindle-shaped cells (indicated by circles) are present between mesothelial cells on liver imprints of PDF-treated animals (B). Representative example of vimentin (green) and cytokeratin (red) staining of a liver imprint of a control (C) and a PDF-treated animal (D); nuclei are stained in blue. Arrows indicate spindle-shaped cells. PDF = peritoneal dialysis fluid.
Discussion
In our study, either UFH or LMWH was added to conventional PDF, based on the characteristics of heparins to reduce new vessel formation and block leukocyte rolling and adhesion, and their ability to bind cytokines and growth factors (6). We showed significant worsening in peritoneal performance after 5 weeks of PDF exposure, as evidenced by high transport characteristics, inflammation, and peritoneal tissue remodeling. Moreover, mesothelial imprints revealed fibroblast-like cells upon PDF exposure. However, none of these PDF-induced events were diminished or prevented by the addition of UFH or LMWH to the PDF.
We decided to add heparins to the PDF in order to obtain maximal local availability and to minimize systemic effects of the heparin intervention. Nonsignificant changes in APTT clotting times and anti-factor Xa levels indicated that the animals were not over-heparinized during the experiment, whereas increased plasma factor Xa levels after LMWH administration showed that adequate working doses were administered. The concentrations used for UFH and LMWH were clinically relevant doses and were similar or even higher compared to the literature (15,24,27-29). Higher concentrations of heparin might have led to bleeding complications or heparin-induced thrombocytopenia (30). The normal clotting times in animals that received daily heparin might be due in part to the fact that intraperitoneal heparin barely reached the circulation or that it already left the circulation within 3 hours after administration. In line with our results are the unaffected APTT and anti-factor Xa measurements of PD patients that received an intraperitoneal injection of LMWH (14,31,32), whereas increased plasma factor Xa levels were seen after subcutaneous injection (32). These data indicate that intraperitoneal administration of heparin has only minor and partial systemic effects (31,32).
Although our intention to avoid systemic effects of heparin treatment was successful, none of the PDF-induced peritoneal changes could be (partly) prevented by the local heparin treatment. Since we were especially interested in the long-term effects of heparin treatment and wanted to avoid direct effects of heparin, we treated the animals daily during 5 weeks and performed the PETs without heparin 1 day after the last heparin administration. An identical methodological approach has been successfully applied in the past with intraperitoneal aminoguanidine treatment (21). This is an important difference with some other studies and might explain why others reported beneficial effects of glycosaminoglycans, such as heparin or hyaluronan, present in PDF during the PET procedure (15,33), which is explained by a reduction of the peritoneal fluid reabsorption rate due to the formation of a filter-cake of the glycosaminoglycan chains at the tissue–cavity interface.
The fact that chronic treatment with either of the heparins did not prevent peritoneal membrane remodeling (new vessel formation, fibrosis, macrophage influx, and mesothelial EMT) might explain why the peritoneal transport values in the heparin-treated groups were not different from the PDF-control group, since molecular transport is highly dependent on vascular surface area and the thickness and composition of the submesothelial matrix (34). Positive effects of heparin on peritoneal transport are reported in studies by Pawlaczyk et al. (13) and Sjoland et al. (14). However, the first study showed only marginal and nonsignificant differences with heparin after 30 days of treatment and, to the best of our knowledge, the second study has not been confirmed by others.
The absence of any effect of chronic heparin treatment on peritoneal inflammatory markers such as cell influx might be explained by the fact that intraperitoneal cell recruitment occurs at the level of postcapillary venules (22) and via the omentum (23). We show that microvascular density in the peritoneal tissues was unchanged by heparin treatment. Moreover, the absence of heparin in the circulation during the PET allowed normal selectin–ligand interaction, which is the first step in leukocyte–endothelial interaction. There have been reports of anti-inflammatory properties of heparinoids in other peritoneal inflammatory models. However, in all those studies, the heparinoids were given intravenously and were present in systemic circulation, thereby inhibiting L- and/or P-selectin-dependent peritoneal cell influx (8,35-38). In line with our results, heparin showed no effects on PDF-induced neutrophil numbers (15), nor did it show any effect on inflammatory cells, fibrosis, or angiogenesis in an animal model of abdominal wound healing (29).
Concerning the role of heparins in angiogenesis, opposite results have been described (29,39). In general, tumor angiogenesis seems to be highly dependent on fibrin formation and tissue factor pathway, processes that are highly modulated by heparin (40). However, not all forms of new vessel formation are fibrin- and/or tissue factor-dependent. An impressive number of factors and mediators might be involved, depending on the model system used (41). The fact that chronic heparin treatment did not prevent neoangiogenesis suggests that intraperitoneal fibrin formation is not involved in our experimental PD model.
Another intriguing finding was the appearance of vimentin-positive cytokeratin-negative spindle-shaped cells within the mesothelial monolayer, which suggests EMT of the mesothelial cells. An alternative explanation would be that the spindle-shaped cells might be submesothelial fibroblasts picked up by the imprint and indicative of partial injury and denudation of mesothelial cells. Addition of either of the heparins did not modify this process and neither heparin affected mesothelial regeneration, as evidenced by increased mesothelial cell density on the liver imprints.
In conclusion, we have confirmed that PD induces significant damage to peritoneal tissues within 5 weeks. Moreover, we have shown an induction of spindle-shaped cells in the mesothelium, indicating either mesothelial damage or EMT. We also conclude that, based on our findings, addition of UFH or LMWH to PDF does not prevent these changes. Therefore, our data do not support long-term peritoneal administration of heparin during chronic PD treatment.
Footnotes
Acknowledgment
This work was supported by Dutch Kidney Foundation grant #C05-2142.