
Abstract
Background
Angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs) are widely used in clinical practice. The safety and efficacy of these agents in peritoneal dialysis (PD) patients are unclear.
Objectives
We conducted a systematic review to study the safety and efficacy of ACEI and ARB use in PD patients. Primary outcome measures were mortality and cardiovascular (CV) events; secondary outcome measures were renal function, proteinuria, hyperkalemia, and erythropoietin requirement at 3 months.
Methods
We searched Medline, EMBASE, Cochrane Central Register of Controlled Trials, trial registry Web sites, reference lists of eligible and review articles, as well as abstracts from the American Society of Nephrology and Canadian Society of Nephrology meetings. To be eligible, studies had to be randomized controlled trials that allocated PD patients to ACEI and ARB use or to placebo or other antihypertensive medications, included adult patients, and reported on at least one of the outcome measures.
Results
418 citations were identified. Four met the eligibility criteria. Three examined CV events and mortality, of which two studies did not have any events. The third showed no statistically significant difference between control and treatment groups in either CV events or mortality: odds ratio 1.56 [95% confidence interval (CI) 0.24 – 10.05] for mortality and odds ratio 1.00 (95% CI 0.19 – 5.40) for CV events. Two studies reported renal function at 12 months and the weighted mean difference was 0.91 mL/minute/1.73 m2 (95% CI 0.14 – 1.68), favoring ACEI and ARB use.
Conclusions
In PD patients, evidence for the use of ACEIs and ARBs for reduction of mortality and CV events is lacking. Limited data suggest that they slow the loss of residual renal function.
Angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs) have been shown to decrease mortality and morbidity in patients with congestive heart failure (1,2) and in patients with acute myocardial infarction (3). They remain the first-line therapy for patients with cardiovascular (CV) disease (4). Similarly, in patients with diabetic and nondiabetic kidney disease, several large trials have demonstrated their effectiveness in reducing proteinuria and delaying progression of chronic kidney disease (5–9). Unfortunately, most large trials excluded patients with end-stage renal disease. The major adverse effects associated with ACEI and ARB use are hyperkalemia, decrease in glomerular filtration rate (GFR), and erythropoietin resistance (10–12). The risk of hyperkalemia increases with the degree of decrease in GFR in the nondialysis population (11). Patients with end-stage renal disease are at high risk of hyperkalemia with ACEI and ARB use, likely due to a combination of decreased urinary and gastrointestinal excretion of potassium (11).
While ACEI and ARB use has been shown in long-term trials to delay progression of chronic kidney disease, there is a hemodynamically mediated decrease in GFR at initiation of therapy that may lead to loss of residual renal function in patients with end-stage renal disease (11). In patients with end-stage renal disease who are on peritoneal dialysis (PD), an association exists between residual renal function and mortality and morbidity (13,14). Interventions that delay loss of residual renal function could have substantial benefit in these patients. Observational studies have shown that each 1 mL/minute increase in residual GFR is associated with a nearly 30% reduction in mortality in this group of patients (14,15).
The other potential side effect of ACEI and ARB use is erythropoietin resistance. Observational studies in the general population have shown that ACEI and ARB use is associated with lower hemoglobin levels, and there is the potential that ACEI and ARB use may aggravate anemia through induction of erythropoietin resistance (16). Erythropoietin resistance has not been rigorously explored in patients on PD.
Thus, while ACEI and ARB use is advocated in PD patients (17), the supporting evidence is unclear. In order to answer questions about safety and efficacy of ACEI and ARB use in patients on PD, we performed a systematic review of randomized controlled trials (RCTs) comparing ACEI and ARB use to other antihypertensive agents.
Material and Methods
The study was conducted using a predefined protocol developed by 5 reviewers (AA, MB, GK, DF, BM, and AD). The primary outcomes of the study were mortality and CV events. A cardiovascular event was defined as any one of the following events: (1) myocardial infarction, (2) new onset angina, (3) congestive heart failure, (4) cerebrovascular accident or transient ischemic attack, and (5) coronary reperfusion procedure. The secondary outcomes were (1) renal function at 12 months, (2) change in proteinuria at 12 months, (3) incidence of hyperkalemia (potassium concentration >5.5 mmol/L), and (4) change in erythropoietin requirements at 3 months. We could not find any study examining proteinuria at 12 months and thus we report any change in proteinuria.
Study Eligibility
The studies were selected by predefined eligibility criteria. Studies were eligible if they were RCTs that randomly allocated PD patients to either ACEI or ARB use or to placebo or other antihypertensive medications, included adult patients (>18 years old), and reported on any one of the outcome measures listed above. There was no restriction of language (except, because of lack of resources, records that did not have title or abstract in English were excluded). There were no restrictions on type of records.
Search Strategy
With the help of an experienced librarian (AD) we electronically searched Medline (1950 to 8 February 2007). We used the key terms “renal replacement therapy,” “renal dialysis,” “peritoneal dialysis,” “angiotensin-converting enzyme inhibitors,” and “angiotensin II type 1 receptor blockers” using the Dickersin filter (18).
Similarly, the EMBASE database was searched from 1980 to 8 February 2007. A filter was developed for the EMBASE database by choosing different headings and text words translated from the Dickerson Medline filter and the article by Haynes (19). The Cochrane Central Register of Controlled Trials was searched until issue 1, 2007. The above three electronic searches were carried out using the Ovid interface.
Additional publications were obtained by searching the reference lists of eligible articles and review articles. In addition, we searched the following trial registries: www.clinicaltrials.gov, www.york.ac.uk/inst/crd/htadbase.htm, and http://controlled-trials.com. The terms used for these electronic searches were “dialysis,” “angiotensin-converting enzyme inhibitors,” and “angiotensin receptor blocker.” This search was performed on 29 January 2007. Manual search of abstracts from the American Society of Nephrology and Canadian Society of Nephrology scientific meetings from 2004 to 2006 was conducted. We also contacted investigators known to conduct trials in this field.
Selection of Studies
Two reviewers (AA and MB) independently screened all the titles and abstracts for potential eligibility. The full texts of all the articles identified by either of the two reviewers were independently assessed using a standard form to determine eligibility. Disagreement between the two reviewers (AA and MB) was resolved by third party discussion (GK). Reasons for exclusion after initial screen were recorded.
Data Abstraction
Data abstraction was performed by two reviewers (AA and MB), independently, using a standardized form. Where data were provided only in tables or graphs, data were extracted from these tables and graphs (20) using the Adobe Acrobat Professional 7.0 program (www.adobe.com). In the event of unclear or unreported data, authors of published articles were contacted for clarification.
Analysis
The results were analyzed by the software Review Manager (RevMan), version 4.2 (The Cochrane Collaboration, Oxford, UK). Continuous data are expressed as mean ± standard deviation. Dichotomous outcomes (mortality, CV events) are reported as odds ratio with its 95% confidence interval (CI). Pooled results are expressed as weighted mean differences (random effects model) and their 95% CIs for continuous outcomes. Homogeneity was assessed clinically as well as statistically by I2 test (21). Due to the small number of studies, publication bias could not be assessed.
Quality Assessment
Quality of the included studies was assessed independently by two reviewers (AA and MB), without blinding to journal or authorship, using the prespecified Delphi list criteria (22) and the criteria of completeness of follow-up.
Results
Included Studies
The search strategy identified 294 records from Medline, 145 from EMBASE, 61 from the Cochrane Central Register of Clinical Trials, and 3 from conference proceedings. After removing duplicates, 418 records were reviewed. Of these, 13 records were found to be potentially relevant and their full articles were reviewed in detail (Figure 1). There was 100% agreement among reviewers about the included studies.
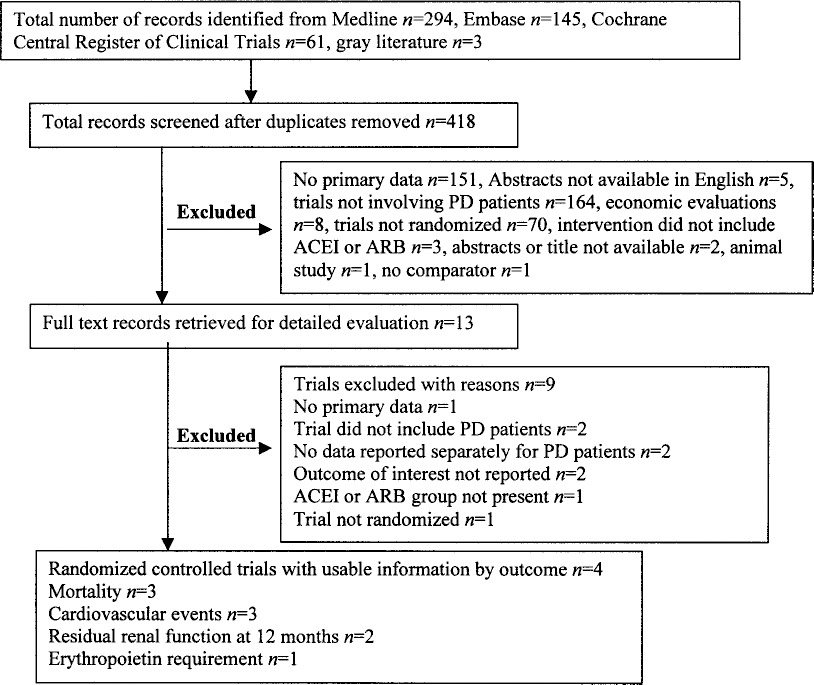
Search results and selection of randomized trials for analysis. PD = peritoneal dialysis; ACEI = angiotensin-converting enzyme inhibitor; ARB = angiotensin receptor blockers.
Tables 1 and 2 summarize the baseline characteristics of the studies included in the analysis. Quality assessment of the studies is summarized in Table 3. There was 100% agreement between the reviewers regarding quality of study.
Baseline Characteristics of Studies Included in the Review
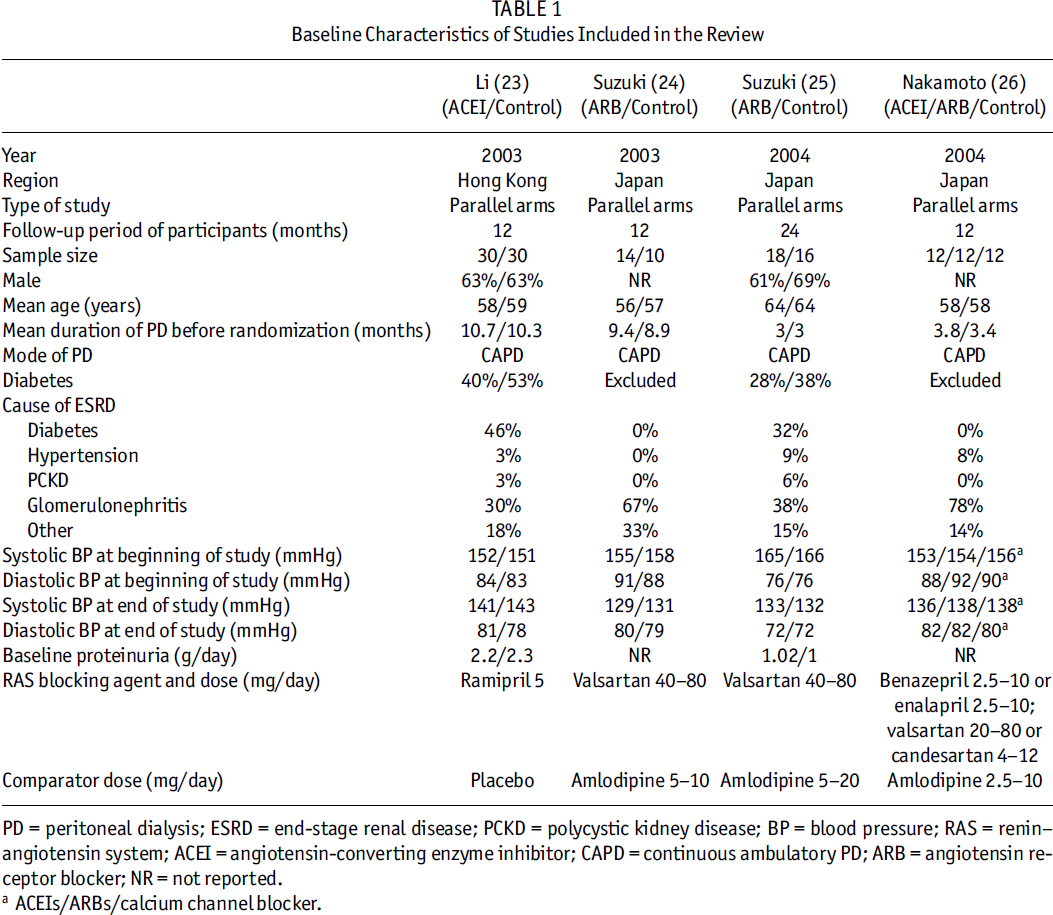
PD = peritoneal dialysis; ESRD = end-stage renal disease; PCKD = polycystic kidney disease; BP = blood pressure; RAS = renin–angiotensin system; ACEI = angiotensin-converting enzyme inhibitor; CAPD = continuous ambulatory PD; ARB = angiotensin receptor blocker; NR = not reported.
ACEIs/ARBs/calcium channel blocker.
Patient Inclusion and Exclusion Criteria of the Studies
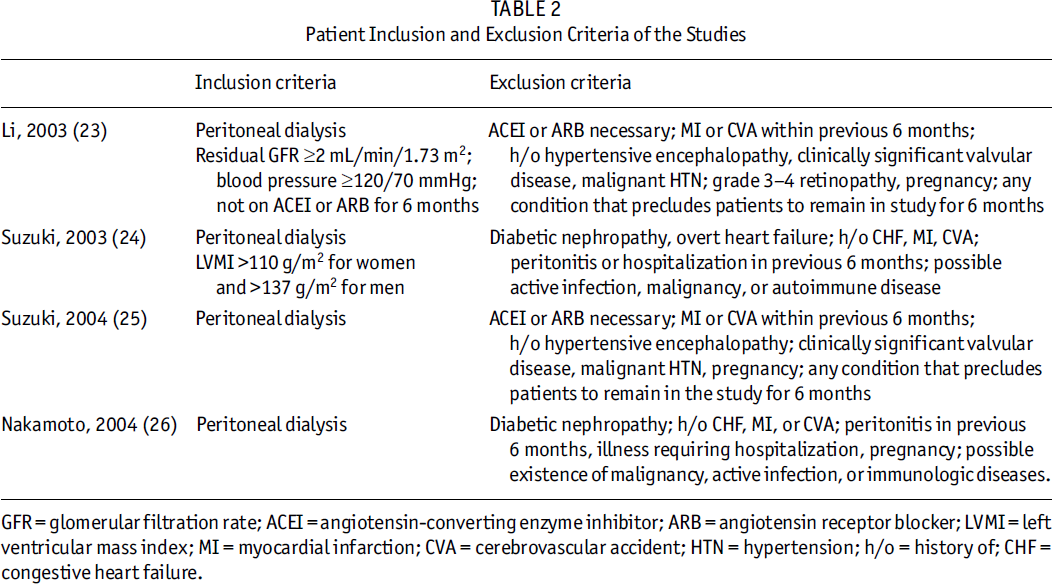
GFR = glomerular filtration rate; ACEI = angiotensin-converting enzyme inhibitor; ARB = angiotensin receptor blocker; LVMI = left ventricular mass index; MI = myocardial infarction; CVA = cerebrovascular accident; HTN = hypertension; h/o = history of; CHF = congestive heart failure.
Assessment of Study Quality
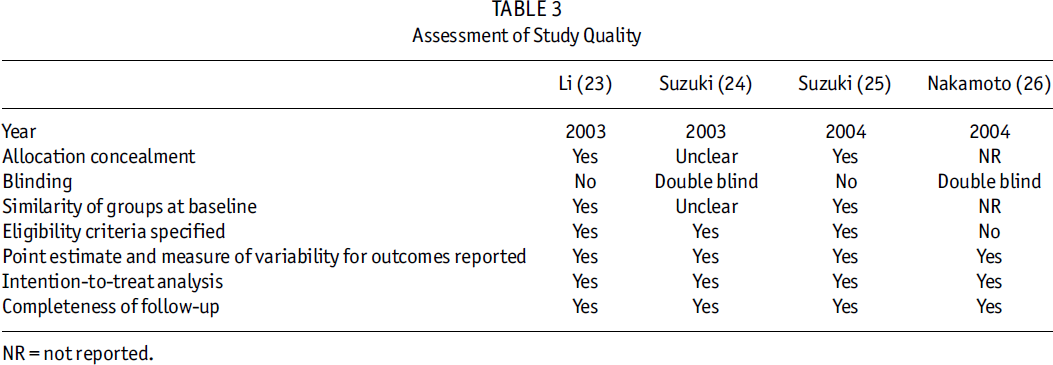
NR = not reported.
Outcomes
Mortality and CV events were reported in three studies (23–25). Two studies by Suzuki et al. (24,25) reported no mortality or CV events. The other study, by Li et al., reported an odds ratio of 1.56 (95% CI 0.24 – 10.05) for mortality and an odds ratio of 1.00 (95% CI 0.19 – 5.40) for nonfatal CV events (23). Both results were statistically not significant. Renal function at 12 months was reported in two studies (23,25). Li et al. reported that, with ACEI, the average decline in GFR was 0.93 mL/minute/year/1.73 m2 compared to control. Suzuki et al. reported that, in their control group, GFR declined from 4.5 ± 2.12 to 3.29 ± 2.14 mL/min/1.73 m2, whereas in their valsartan group, GFR increased from 4.1 ± 1.02 to 4.5 ± 2.12 mL/min/1.73 m2. Statistically, there was no evidence of heterogeneity between the two studies (I2 = 0%). The pooled estimate revealed that use of ACEI and ARB was associated with a statistically significant higher GFR of 0.9 mL/min/1.73 m2 (95% CI 0.14 – 1.68). Change in proteinuria at 24 months was reported by Suzuki et al. (25) and was not statistically different between their two groups (ACEI and ARB use group 1.11 ± 0.51 vs 1.12 ± 0.4 g/day, p > 0.05). In addition, Li et al. reported median protein excretion at 6 months to be 0.28 (range 0 – 7.9) g/day in their ACEI and ARB group, versus 0.30 (range 0 – 1.6) g/day in their control group.
Adverse Events
None of the studies reported incidence of hyperkalemia at 3 months. One study (26) reported erythropoietin requirements at 3 months. The change in erythropoietin requirement was reported as statistically significant, indicating ACEI and ARB use leads to erythropoietin resistance. We believe the calculations in this paper are in error, as standard error instead of standard deviation was used in test procedures.
Discussion
ACEI and ARB are widely prescribed medications to control blood pressure, decrease CV mortality and morbidity, and preserve renal function. Several large trials have established their role as first-line therapy for proteinuric renal disease as well as for prevention of CV disease (1–3,5–9). We conducted this review to determine the evidence for ACEI and ARB use in the PD population. Our systematic review reveals that, in PD patients, evidence for the use of ACEI and ARB for reduction of mortality and CV events is lacking; however, limited data suggest that these agents slow the loss of residual renal function.
The major strength of our systematic review is the application of rigorous methodology in the conduction of our study: we followed the published recommendations of “the QUOROM statement” (27) for reporting our review; we used strict criteria to define our outcomes; we attempted to extract all data that could affect our outcomes; and we performed a broad search to find relevant studies and did not limit our search to English literature.
The inclusion criteria of our review limited us to four studies. Mallet and Clarke (28) reported a median of 6 trials per systematic review (interquartile range 3 – 12) and Jadad et al. (29) reported a median of 5 trials for Cochrane review and a median of 13.5 trials for paper-based journals. (Jadad et al. did not report interquartile range.) The number of trials in our study is thus comparable to typically published systematic reviews. We could have increased the number of trials by allowing weaker designs, such as nonrandomized trials, to be included in our study but this would have been at the expense of study quality and may have resulted in biased results.
Although ACEIs and ARBs are widely used medications, the data regarding their impact on PD patients are limited. We could locate only three (23–25) randomized studies that commented on mortality and CV events, and none of these trials were adequately powered to detect a difference in mortality or CV events. All these trials were of short duration, the longest one having a follow-up of 2 years. All three trials included low risk patients, and the small number of observed events limited the generalizability of our findings such that we were unable to make any firm conclusions regarding the efficacy of ACEIs and ARBs for reduction of mortality and CV events in PD patients. The issue of inconclusive results in systematic reviews has been addressed by Naylor in his publication “The Case for Failed Meta-Analyses” (30). He emphasizes that, “So long as the process of finding and analyzing the studies has been systematic and unbiased, the review should be documented and disseminated with an appreciation of its potential value to clinicians, managers and researchers alike.” Our study highlights the limited data regarding ACEI and ARB use in patients on PD and the need for further research.
Limitations to our study should be noted. First, we had to exclude the study by Robson et al. (31) as we were unable to obtain primary data from the authors. This potentially important study randomized a total of 107 patients of which 47 were CAPD patients, but the authors presented combined results and no results were presented separately for PD patients. Availability of these data would have helped improve the precision of our systematic review. Second, pooling of the data for renal function involved only two trials (23,25) (one trial of 12 months duration did not report GFR at termination), with total number of patients randomized being 94, leading to imprecision of our results. Third, erythropoietin requirement was assessed by only one trial (26) of 3 months duration, the quality of which was not optimal (did not report on allocation concealment) and the sample size was small, thus limiting our ability to make any firm conclusions. Last, three of the trials were from one center, again limiting the generalizability of our findings.
Although large trials have proven the efficacy of ACEIs and ARBs in delaying the progression of chronic kidney disease as well as improving mortality, data from patients with chronic kidney disease who are not on dialysis cannot be conclusively extrapolated to the dialysis population. Wanner et al. (32) randomized 1225 patients on hemodialysis to atorvastatin 20 mg per day or placebo for 2 years, with their primary end point being a composite of CV death, fatal stroke, nonfatal myocardial infarction, and nonfatal stroke. Wanner et al. were not able to detect a statistically significant difference in their primary end point. Similarly, retrospective evidence indicated that ACEI provides clinical benefit to patients on hemodialysis. Zannad et al. (33) randomized 397 hemodialysis patients with left ventricular hypertrophy to ACEI (fosinopril) or placebo. Their primary end point was first fatal or nonfatal CV event. They again failed to show a statistically significant benefit for ACEI (fosinopril), although the trial was inadequately powered. These examples suggest the efficacy of ACEIs and ARBs needs to be tested directly in PD patients with adequately powered randomized trials. To detect a significant difference of 10% for the primary end point of mortality with alpha of 5% and power of 80%, and assuming a baseline 5-year mortality rate of 69% (34) in the PD population, a minimum of 716 patients would have to be randomized and followed for 5 years to answer the question whether ACEIs or ARBs improve mortality in this population. Similarly, limited available data suggest that ACEIs and ARBs preserve residual renal function. To conclusively answer this question, calculation of sample size using alpha of 5%, power of 80%, standard deviation of 2.5 mL/minute, and clinically significant preservation of renal function to be 1 mL/minute/year reveals that a minimum of 198 patients would need to be randomized and followed for 1 year.
Conclusion
Insufficient evidence exists to determine the benefit of ACEIs or ARBs for reduction of mortality and CV events in PD patients. Limited data indicate that ACEI and ARB use may slow the loss of residual renal function. In the randomized trials, no significant adverse events were reported but it should be noted that these trials were not appropriately designed to examine for adverse events. Large RCTs of high quality are needed to determine the benefits of ACEI and ARB use in the PD patient population.
Scheduled Review Update
We plan to update this review after 3 years.
Funding
No funding was obtained for this study.
Footnotes
No financial conflict of interest exists.
Acknowledgments
This study was conducted as a part of the systematic review course at the University of Ottawa in 2007.