
Abstract
During the 2008 Congress of the International Society for Peritoneal Dialysis, academic nephrologists, nephrology societies, and government officials from Colombia, Brazil, Argentina, Chile, Central America, Ecuador, and Mexico participated in a roundtable discussion on the Economics of Dialysis and Chronic Kidney Disease in Latin America. The main focus was policy and health care financing. The roundtable promoted open discussion between policymakers and clinicians on how to find viable solutions to contain spending on treatment for end-stage renal disease into the future. A number of options were proposed, including early medical intervention (disease management programs) to slow the progression of chronic kidney disease in high-risk patients, promotion of pre-emptive renal transplantation, and use of the most cost-effective dialysis therapy that can be offered to a patient without compromising outcome. It was concluded that the burden of treating more patients in the future could be alleviated by wider utilization of peritoneal dialysis (PD). However, important changes in health care reimbursement systems and realignment of incentives in the region are required to support wider PD penetration.
In recent years, the global number of patients with chronic kidney disease (CKD) at all stages grew, with a particular rise in the number of patients with end-stage renal disease (ESRD) in need of some form of renal replacement therapy (RRT), either hemodialysis (HD, 6.4%), peritoneal dialysis (PD, 5.8%), or renal transplantation (6.8%). The number of patients requiring maintenance dialysis worldwide has been projected to increase to more than 2 million by the year 2010, with the associated treatment cost rising to US$1.1 trillion for the decade 2001 – 2010. In Latin America, broad variation in the prevalence and incidence of ESRD is observed, but the growth trend is very similar to the world trend. The distribution of patients by therapy and the sources of funding for dialysis therapy, which are determined by local health care financing systems, also vary widely between the countries of Latin America.
During the 2008 Congress of the International Society for Peritoneal Dialysis (ISPD), academic nephrologists, society leaders, and government officials from Colombia, Brazil, Argentina, Chile, Central America, Ecuador, and Mexico participated in a successful roundtable discussion on the Economics of Dialysis and Chronic Kidney Disease in Latin America. The meeting was organized by the Latin American Chapter of the ISPD. The main focus was policy and health care financing. The roundtable promoted open discussion between policymakers and clinicians on how to find viable solutions to contain spending on ESRD treatment into the future. The remainder of the present paper summarizes the main themes discussed during the meeting.
Overview of CKD and Dialysis Treatment in Latin America
Latin America encompasses a territory of 20.5 million square kilometers, with a population that was 551 million in the year 2005, that is growing at an annual rate of 1.3%, and that is concentrated primarily (78%) in urban areas (1). Latin America has made some progress in economic issues—for example, per capita gross national income is currently US$4008, and mean annual income growth is 4.4% (2)—but 37% of the population is still living in poverty, and inequality in income distribution in the region is among the highest in the world (1). The human development index is 0.8 in this region (3), and the illiteracy rate is 9.5% in people over 15 years of age. Homes without piped water and sanitation respectively comprised 11% and 26% of the total (1). With regard to health issues, life expectancy at birth is now 72 years, and the elderly population (over 65 years of age) is 8.7% of the total, but is expected to increase to 12.6% by 2020 (1). The mortality rate in children under 5 years of age is 32 per 1000 inhabitants, 8.8% of newborns are of low birth weight (less than 2.5 kg), and daily energy intake in the adult population is 2861 Kcal. A major problem is the low percentage of gross domestic product devoted to health care in these countries, which is reflected in low rates of physicians (1.8), nurses (0.8), and hospital beds (1.9) per 1000 inhabitants (4).
According to the 2002 Annual Report from the Latin American Society of Nephrology and Hypertension (the report most recently published), the prevalence of dialysis (both HD and PD) and renal transplantation was 363 patients per million population (5). In the same document, an acceptance rate of 103 new patients per million population for RRT was noted (5).
In Latin America, hemodialysis is the predominant form of RRT (6), although four countries (Colombia, Guatemala, El Salvador, and Mexico) use PD in 30% or more of ESRD cases (Figure 1). In particular, Mexico is the country with the greatest PD utilization in the world (7), and it is estimated that approximately 25% of the world PD population comes from Latin America.
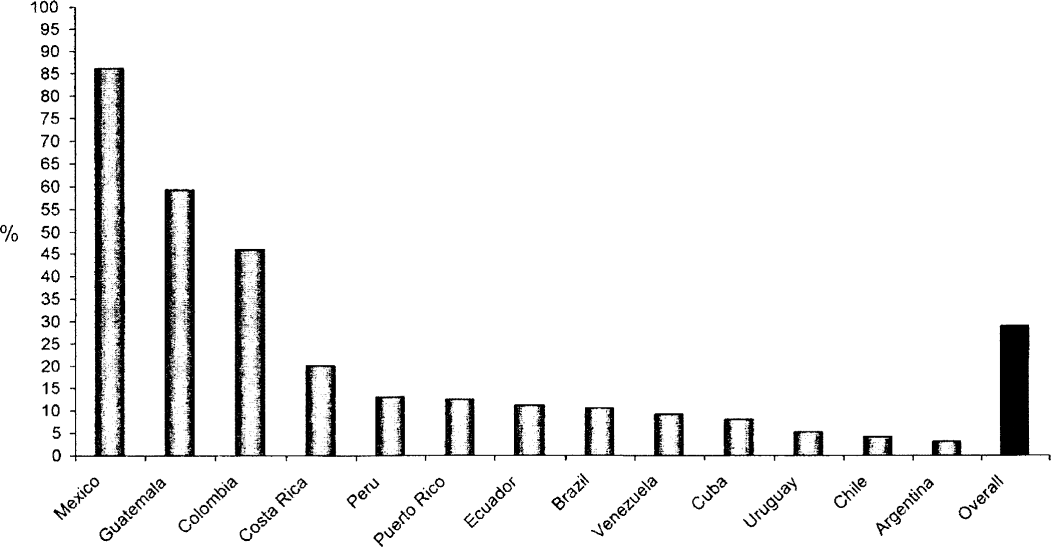
Individual and global penetration of peritoneal dialysis in various countries of Latin America, showing an important variation in utilization.
Clinical Outcomes by Dialysis Modality: A Latin American Perspective
In recently published studies, PD survival rates are as good as HD rates in incident patients, at least during the early years of therapy. The literature has consistently documented PD as being less costly than in-centre HD worldwide. Most patients needing dialysis meet the criteria for both PD and HD, and with pre-dialysis education, patients are as likely to choose PD as HD, with a strong preference for home therapy given comparable clinical outcomes. Health economic evaluation can help in making complex decisions about the allocation of limited health care funds and can help policymakers to implement cost-effective strategies for treating ESRD now and into the future.
The Colombian model of RRT is unique in Latin America. Mainly because of equilibrium in the reimbursement for HD and PD, the proportion of patients on HD and PD is also equilibrated, with 40% of patients on PD. This situation permitted an interesting retrospective cohort study to be conducted, comparing clinical results for PD and HD. Although not a randomized controlled clinical trial, the Dialysis Outcomes in Colombia (DOC) study provided robust data on the comparative performance of these two modalities in the Latin American setting (8). The study observed incident patients on dialysis (HD or PD) in several units in Colombia from 2001 until 2005. The 923 patients included (437 on HD and 486 on PD) were analyzed in both an as-treated and an intent-to-treat fashion. Both groups were similar in terms of demographics and clinical characteristics, but PD patients presented more comorbidities (mainly diabetes and cardiovascular disease) and a lower socio-economic level. The main results point to very similar patient survival for HD and PD. This finding held true both in the intent-to-treat analysis and in the as-treated analysis, and remained similar after adjustment for confounding factors. In the subgroup analysis, younger patients (less than 65 years of age) with fewer comorbidities (nondiabetic patients) experienced significantly better survival on PD as compared with HD.
The results of the DOC study point to an interesting reality of dialysis treatment in Colombia, showing that PD patients present a lower socio-economic level and a higher degree of comorbidity. Nevertheless, the overall clinical results in comparison with HD were satisfactory and equivalent.
Applying Health Economics for Better Resource Allocation in Dialysis
With the numbers of ESRD patients challenging available health care funding, particularly in lower-income countries, the need is urgent to find solutions to managing the treatment of ESRD and to controlling ESRD spending without compromising patient care or quality. Interesting strategies that could help in a cost-effective approach to CKD treatment include early medical intervention to slow the progress of renal disease in high-risk patients, avoidance of later referral or an unplanned start to treatment, provision of grafts if available, provision of primary care by nephrologists, and choice of the most cost-effective dialysis therapy that can be given to a patient without compromising outcome.
With lower total component expenses than those for HD, PD has economic benefits that should be considered when analyzing the costs and benefits of various treatment modalities. Although supplies cost more for PD than for HD, hospitalization expenses are similar. Erythropoietin and other drugs, staff, facilities, infrastructure, and transportation costs incurred by PD are considerably less than they are for HD. Simply cutting back on the dialysis dose does not actually lower expenses if the adverse health consequences of inadequate HD are taken into account. Similarly, despite the initial product outlay with PD, reducing peritonitis saves money, because the fewer complications offset the extra expense. A number of reimbursement barriers give health care providers less financial incentive to use PD. Realigning incentives to support equally effective, lower-cost treatments when these are right for the patient would permit health care funders to offer quality treatment to more patients within a given budget.
Dialysis Pharmacoeconomy in Dialysis: The Chilean Experience
Because of the view in Chile that HD treatment was significantly less expensive than PD treatment, a public policy limiting access of patients to PD was reinforced. The real cost of both therapies was recently reanalyzed (9), taking into consideration the total costs of both HD and PD. In that study, 159 patients from five selected dialysis units in Chile were retrospectively studied. The HD and PD groups did not show differences in a quality-of-life index, although better customer satisfaction was observed in PD than in HD. Annual global costs for HD were US$20810; for PD, they US$20750. The cost–utility index in HD was 3.16; it was 3.10 in PD, mainly because of the lower consumption of erythropoietin and the better capacity for work in PD patients as compared with HD patients.
Overview of Reimbursement for Dialysis in Selected Latin America Countries
Reimbursement for dialysis in Latin America varies extensively, depending on the country. In general, only a few countries offer universal coverage based on a public (Brazil, Chile, Uruguay) or private health care system (Argentina). Some still have major restrictions in terms of offering access to dialysis (Bolivia, Ecuador, Peru). Most countries offer a mixed system for dialysis reimbursement, with different shares attributed to private and public systems. The main characteristics of reimbursement in selected Latin America countries (in alphabetical order and restricted to the countries represented in the meeting) are described in the following subsections.
Argentina
The access to RRT (HD and PD) is universal, and all patients have a health care provider. A large proportion (30%) of patients are covered by PAMI (Argentina's state-funded medical care system); fewer than 3% are in the public system. Almost all dialysis centers are private (95%); about half have national capital, and 43% belong to international chains. Reimbursement for dialysis (US$903/month) includes transport for patients to the unit, peritoneal or vascular access, erythropoietin, calcitriol, iron, vitamins, phosphate binders, antibiotics, and professional charges.
Brazil
Dialysis patients are universally covered, 90% by the public health system. Public reimbursement (in October 2006) for HD was US$76 per dialysis session, and for PD, it was US$1085 per month, not including specific medications. Reimbursement for automated PD was slightly higher at US$1395 per month.
Central America and the Caribbean
In Guatemala, the reimbursement system allows for universal access to dialysis through social security, but in most of the other countries, the reimbursement system is limited and not well defined.
Chile
Private and public health systems both cover dialysis therapy, governed by the same legal guarantees. By law, citizens have the same level of accessibility, opportunity, and quality for treatment of all diseases, including ESRD. The public health insurance system is FONASA. For HD treatment, FONASA covers 66.4% of the population (according to the last report of the annual survey of the Chilean Society of Nephrology). No information is available about public coverage of PD, because, by law, FONASA covers mainly HD treatment. In 2005, reimbursement per patient–year was US$14654 for PD and US$10909 for HD, universally covered by public funds. Recently, an initiative was started to increase access and coverage to PD, which may affect PD use in Chile.
Colombia
Dialysis reimbursement in Colombia allows an equal amount for HD and for PD, approximately US$1400 per month for both treatments. Dialysis treatment is offered to most patients with CKD, mainly through insurance systems.
Ecuador
Insurance systems (ISSFA from the military and ISSPN from police) cover only a small part of the population. It is estimated that only 5% are able to cover dialysis expenses from private resources. The reimbursement for HD is US$1300 per month and includes all access, medication, treatment of comorbidities, and laboratory services.
Mexico
Three social security institutions cover 50% of the population: Instituto Mexicano del Seguro Social, Instituto de Seguridad y Servicios Sociales para los Trabajadores del Estado, and the armed forces. The remaining half of the population has no public coverage. In the last 2 years, a new voluntary popular insurance administered by the Health Ministry began support the low-income population, currently 10 million people. Only patients within the social security systems have universal coverage, including RRT.
Potential Obstacles to Wider Utilization of PD in Latin America
Despite a potential cost–benefit advantage of PD over HD when the characteristics of the region are analyzed, the utilization of PD in the treatment of ESRD remains low in many Latin American countries. Medical factors alone cannot account for the low utilization rate. Training in, and exposure to, PD are clearly inadequate for many nephrologists in the region. Many centers have small numbers of PD patients, which affects their clinical results. As patients reach ESRD status, they may not be sufficiently informed about dialysis modalities and therefore may not be able to choose properly. Even more important, it appears that the choice of dialysis modality in individual countries is closely related to the local health care reimbursement system.
Economics of CKD in Latin America: The Way Forward
Although most countries in Latin America with established RRT offer PD as a viable option, there is clearly a potential for more widespread use of PD in the region. Geographic conditions (large distances from dialysis centers), financial limitations, lack of access to HD technology, and a shortage of nurses and nephrology are all reasons for a potentially higher penetration of PD in Latin America. Moreover, most countries in the region have a large number of patients with ESRD who are undiagnosed and lack access to RRT. As health care improves in the region, there will be a need to discuss the best model to provide dialysis to a growing population. Peritoneal dialysis plays an important role in this expansion in access, which should be universal.
Regarding the ideal resource allocation for the management of ESRD, a number of options were proposed, including early medical intervention (disease management programs) to slow the progression of CKD in high-risk patients, promotion of pre-emptive renal transplantation, and use of the most cost-effective dialysis therapy that can be offered to a patient without compromising outcome. This burden of treating more patients in the future could be alleviated by wider utilization of PD, which could be equal to or more cost-effective than HD. However, important changes in the health care reimbursement systems and realignment of incentives in the region are required to support wider PD penetration. Additional obstacles that account for a low PD utilization in some Latin America countries are the inadequate training and exposure to PD for many residents and nephrologists, and the insufficient and inaccurate information about PD and HD delivered to patients as they reach ESRD status.
Footnotes
Acknowledgment
This roundtable was made possible by an unrestricted educational grant from Baxter Healthcare. The authors thank Juan Carlos Blackburn for his important help in preparations for the meeting.