
Abstract

Resurgence of the Percutaneous Technique for Positioning the Tenckhoff Catheter at the Start of Peritoneal Dialysis
Introduction: Currently, the design of the Tenckhoff catheter and the surgical techniques used for positioning are diverse. The catheters can be placed percutaneously, surgically, laparoscopically, or with the aid of specialized equipment such as fluoroscopy and ultrasound. Of the various dialytic therapies, peritoneal dialysis (PD) is the renal replacement method most used in our institution, and the positioning of the peritoneal access is a priority.
Objectives: To report the results of Tenckhoff catheter positioning by the percutaneous technique used in our institution.
Methods: This retrospective study looked at a period of 3 years (January 2004 to December 2006) and identified patients [403 men (46%),478 women (54%); average age: 58.9 years (range:18 – 78 years)] with chronic renal insufficiency who required a peritoneal access. The causes of their renal failure, their demographic distribution, their age groups, their diabetes status, related complications, catheter survival during the first year, and the costs generated by the procedure were recorded.
Results: Tenckhoff catheters (n = 881), spiral type, were placed by 2 nephrologists using the Quinton–Kendal mark and percutaneous technique. The causes of chronic renal failure were type 2 diabetes mellitus (57%), arterial hypertension (13%), chronic glomerulonephritis (4%), obstructive uropathy (2%), rejection of renal graft (1%), polycystic kidney (1%), eclampsia (1%), and unknown (19%). Complications were exit-site infection (15%), dialysate leak (2%), bleeding (0.5%), perforation of hollow viscera (0.3%), and slow drainage (5%). In 6% of catheters, a guide wire was used for catheter relocation 3%, and catheter survival was 100%, 97%, and 91% at 3, 6, and 12 months respectively.
Conclusions: The percutaneous technique allowed for immediate dialysis start with minimum complications. Catheter survival was considered excellent, and the procedure cost less than the equivalent surgical positioning. The percutaneous technique is ideal in patients who are initiating PD therapy and who present with a useful abdomen.
Peritoneal Dialysis Catheter Insertion Using a Double-Lumen Hemodialysis Catheter
Objectives: Among several techniques for insertion of a continuous ambulatory peritoneal dialysis (CAPD) catheter, blind percutaneous placement is still used. However, the technique is time-consuming and may induce serious complications such as pre-peritoneal placement, bowel perforation, and hemoperitoneum. To perform CAPD catheter insertion more easily, quickly, and safely at bedside, we developed a new method using a double lumen hemodialysis (HD) catheter instead of a 16 gauge angio-needle and trocar (16ANT). We investigated the clinical utility of this approach in establishing access for PD.
Methods: A double-lumen HD catheter (You-Bend two-lumen HD catheterization set, Arrowguard Blue: Arrow International, Reading, PA, U.S.A.) was inserted by the modified Seldinger method, aiming 15 degrees of perpendicular direction toward the patient's coccyx. Dialysis solution (2 L) was infused through the arterial port. After the HD catheter was removed, a CAPD catheter with a stylet was introduced into the insertion site. The guidewire remained through the insertion site until the CAPD catheter insertion succeeded. We applied this method in new patients during 2008 – 2009 (group 1, n = 13) and compared the results with results from 16ANT during 2006 – 2007 (group 2, n = 51).
Results: Baseline characteristics were similar in the two groups. However, compared with group 2, group 1 showed a significantly shorter time for infusion of 2 L of fluid (13.7 ± 1.3 min vs. 28.7 ± 3.2 min, p < 0.05) and for the total operation (88.0 ± 13 min vs. 105.7 ± 7.5 min, p < 0.05). Early technical complications were not statistically different between the groups; however, there was a tendency for fewer serious complications with the new method.
Conclusions: Compared with the old method, the new method showed a significantly shorter infusion time and total operation time. Early technical complications tended to be fewer with the new method. Thus, this new method seems to offer considerable savings in operating time and reductions in short-term serious complications.
Success Rates for Peritoneoscopically-Inserted Coiled versus Straight Tenckhoff Catheters
Aim: Continuous ambulatory peritoneal dialysis (PD) has been advocated by the Malaysia government as the renal replacement therapy of choice. The PD catheter remains the Achilles heel of PD programs worldwide. Our center has been actively performing peritoneoscopic Tenckhoff catheter (TC) insertion since February 2006. In this study, we compared the success rates of coiled versus straight TCs.
Methods: We prospectively analyzed the survival of 42 catheters peritoneoscopically implanted (Y-Tec system: MediGroup, Etobicoke, ON, Canada) with regard to the catheter type. From August 2008, all procedures were performed by the in-house interventional nephrologists. The patients were randomized to receive either a straight or a coiled TC. All patients who required catheters for the purpose of intermittent PD or through referral from other institutions for sole purpose of TC insertion were excluded. A total of 19 doubled-cuffed coiled TCs (57.5 cm, Jet) were implanted by the right paramedian approach with the tip directed toward to the left pelvic cavity. Another 24 double-cuffed straight TCs (42 cm, 47 cm, Jet) were implanted by the left paramedian approach with the tip directing toward the left pelvic cavity. We defined primary catheter dysfunction as failure of inflow, outflow, or both, within 1 month of TC insertion. Standard catheter care with mupirocin and povidone iodine was used for all cases.
Results
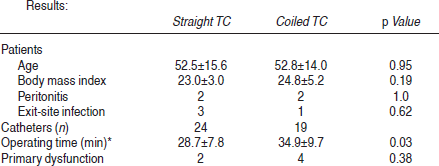
There was no significant difference in terms of primary failure, peritonitis, and exit-site infection for the two TCs. However the operating time needed to implant a straight TC is significantly shorter.
Conclusions: We demonstrated that a straight TC implantation with the tip toward the left pelvic region produces results similar to those with a coiled TC. Besides the substantial cost saving of US$50 per catheter, a straight TC saves significant implantation time.
Effect of Ultrasonography in Peritoneal Dialysis Catheter Placement
Objectives: The surgical approach is the most common way to insert a peritoneal dialysis (PD) catheter. The key is to make sure that the catheter is placed in the right place of the abdominal cavity. Our study investigated the feasibility and effect of ultrasonography in the placement of PD catheters.
Methods: From January 2008 to January 2009, ultrasonography-guided placement of PD catheters was attempted in 22 chronic renal failure patients. A straight Tenckhoff catheter was placed into a rectovesical excavation or rectouterine excavation using routine surgical procedures under ultrasound guidance. All patients were operated by the same surgeon and ultrasound operator. Routine postoperative treatment was performed.
Results: PD catheters were successfully placed in all 22 patients. All patients started PD successfully after placement and were followed for a median of 5.4 months. None experience catheter drift, colic omentum circumvolution, or inferior abdomen discomfort.
Conclusions: Placing the PD catheter in the right place in the abdominal cavity is critical. Our study shows that ultrasonographic technique allows for accurate assessment of the entry into the abdominal cavity. This technique can reduce the incidence of complications such as abdominal discomfort, inadequate drainage, and catheter drifting. In addition, the technique is easier to perform and more suitable than peritoneoscopic placement, which needs special technique. Thus, this ultrasound-assisted placement of the PD catheter is worthy of application.
Clinical Experience of Peritoneal Dialysis Catheter Replacement
Objectives: Displacement of peritoneal dialysis (PD) catheters (caths) occurs for various reasons. To ensure dialysis efficacy, the cath should be re-placed in the correct position. This study explored methods and clinical experience in how to re-place displaced caths.
Methods: Patients underwent PD cath insertion and were then examined by plain abdominal radiograph and type-B ultrasound. These examinations were repeated when the PD cath was suspected to have been displaced. In combination with radiographs, clinical experience was used diagnose the displacement of the PD caths. Manipulative replacement, guidewire technique, and surgery were all used to re-place displaced caths. Signs of a successful PD cath re-placement included improved inflow and outflow of PD fluid, and imaging showing that the cath was in the right position.
Results: In the past 3 years, 75 patients underwent PD cath insertion, and 11 experienced cath displacement (14.6%), with 6 cases happening in the first week, 4 cases after 2 months, and 1 case after 18 months. The main reasons for displacement were cath distortion (3 cases), incorrect posture such as sitting cross-legged for a long time (3 cases), constipation (2 cases), enterokinesia caused by PD fluid (2 cases), excessive PD fluid used at an early stage (1 case). Of the 6 cases choosing manipulative re-placement, 4 cases were successful, and the other 2 failed (the caths were later successfully re-placed by guidewire). Another 2 cases took laparoscopic re-placement. Operation was chosen in 1 case, and 2 patients transferred to hemodialysis after failure of both manipulative and operative re-placement.
Conclusions: Cath displacement is a common complication of PD. Displacements can happen in the first week or up to 18 months after implantation. The extent and direction of displacement was determined by X-ray before re-placement. Manipulative cath re-placement is possible if the radiograph shows the cath to be in the upper right edge of the sinus rectales. Guide wire is another choice when manipulative re-placement fails. If these two methods don't work, laparoscopic or traditional surgical re-placement may be used according to the specific circumstances and patient choice.
Effect of the Technique of Affiliation to the Abdominal Wall in Peritoneal Dialysis Catheter Insertion Operation under Direct Vision
Objectives: Survival of the peritoneal dialysis (PD) catheter (cath) largely affects long-term survival in PD patients. One common complication of PD cath insertion is cath shift. We observed re-affiliation to the abdominal wall in the PD cath insertion operation and its effect on the ratio of PD cath shift. Methods: We allocated 38 chronic renal failure patients who chose PD as their renal replacement treatment to one of two groups according to their PD cath insertion operation: with affiliation (AF) or without affiliation (NAF) to the abdominal wall. After 1 month, we compared inflow and outflow velocity of PD fluid, ultrafiltration, and ratio of PD cath shift between the two groups. In the NAF group, a median incision was made 1 – 2 cm below the umbilicus. In successive steps, skin, subcutaneous tissue, and anterior aponeurosis of the recti abdominis (ARA) were separated, and the rectus abdominis was bluntly dissected. Finally the posterior ARA and peritoneum were exposed and cut open; a purse-string suture was used for two layers without tightening the thread. In the AF group, a single double-strand loop was used to ligate the abdominal cavity segment of the dialysis cath (3 cm below Terylene cowl 2), and the two ends of the thread were placed outside the incision before cath insertion. Using a wire, the cath was inserted straight down and back toward the vesicorectal or Douglas pouch approximately 2 – 3 cm under the purse-string suture. Then a small incision was cut in the posterior ARA and peritoneum, and curved forceps were used to deliver the detained thread of the abdominal cavity segment of the cath. The incision was closed with interrupted sutures; the purse-string was tightened; and needles were used in the double-strand thread to let it go through the abdominal membrane. Finally, the strand was ligatured and fixed, and the anterior ARA, subcutaneous tissue, and skin were successively sutured. In the NAF group, we placed the cath into the vesicorectal or Douglas pouch only after suturing the purse. After that, we tightened the purses and successively sutured anterior ARA, subcutaneous tissue, and skin. Results: There was no difference in inflow and outflow velocity of PD fluid or in ultrafiltration between the groups. However, the cath shift ratio was 0 in the AF group, significantly lower than in the NAF group (15%). Conclusions: Using the technique of affiliation to the abdominal wall significantly reduced the cath shift ratio after operation.
Clinical Observation of Laparoscopy for Continuous Ambulatory Peritoneal Dialysis Procedures
Objectives: Peritoneal dialysis (PD) is the preferred type of treatment for patients (pts) with end-stage renal disease. One of the most common problems encountered during therapy is catheter displacement after conventional catheter placement, which frequently leads to failure of long-term PD. More effective techniques of PD catheter placement are required to avoid catheter problems and maintain normal dialysis. This study reviewed and evaluated laparoscopic (Lap) catheter (cath) placement in our hospital.
Methods: From 2004 to 2009, 460 PD caths were placed at our center. No selection criteria were applied regarding the choice between hemodialysis (HD) and PD. After being informed about the consequences of each modality, pts chose the treatment option. We retrospectively reviewed the records of 32 pts (30 with a history of abdominal or pelvic operation) who underwent Lap procedures. Clinical details of the cath placement procedures and outcomes (cath function and complications) were reviewed. A comparative analysis of traditional open surgery was also carried out. All Lap procedures in this study were performed under general anesthesia by two surgical specialists.
Results: Lap cath placement was used in 32 pts, and 1 cath was displaced and removed. Meanwhile, 428 pts underwent cath placement by open surgery under local anesthesia, and 24 caths were displaced and subsequently fixed by Lap procedure under general anesthesia. There was no statistically difference in the absolute number or percentage of functional caths implanted by the different methods (p > 0.05). Pts with a history of abdominal or pelvic operation had better clinic outcome. In addition to displacements, other complications such as hernia, leakage, and wound sepsis also occurred in both groups (4 in the Lap group, 65 in the open-surgery group). However, the statistical difference was between two groups was nonsignificant (p > 0.05). In the Lap group, the operative time was significantly shorter than it was in the traditional open-surgery group (p < 0.05).
Conclusions: Lap cath placement is a quicker and less complicated technique than is conventional cath implantation. In particular, Lap technique can reduce the incidence of cath displacement. Disadvantages include expensive equipment and general anesthesia.
Coiled versus Straight Catheters in Peritoneal Dialysis: A Meta-analysis of Randomized Controlled Trials
Objectives: As many as 15% – 50% patients with end-stage kidney disease are on peritoneal dialysis (PD). Current clinical practice guidelines indicate that no particular type of peritoneal dialysis (PD) catheter has been proved superior to another. Our goal was to evaluate clinical outcome with two different catheters.
Methods: The Cochrane CENTRAL Registry, PubMed, and EMBASE were searched for randomized trials of catheter types (coiled vs. straight) in PD. Two reviewers extracted data on rates of peritonitis and exit-site or tunnel infection, catheter removal and replacement, technique failure, and all-cause mortality. The analysis used a random-effects model, and results are expressed as relative risk (RR) and 95% confidence intervals (CIs).
Results: Seven full-article eligible trials (480 patients) were identified. There was no significant difference in the risk of peritonitis (five trials, 376 patients—RR: 1.12; 95% CI: 0.58 to 2.17) or exit-site or tunnel infection (five trials, 384 patients—RR: 0.93; 95% CI: 0.55 to 1.58) between catheters with a straight or a coiled intraperitoneal portion. With no significant heterogeneity, there was no significant difference in all-cause mortality with the use of straight as compared with coiled catheters (three trials, 261 patients—RR: 0.64; 95% CI: 0.24 to 1.68). There was also no significant difference in the risk of catheter malposition (catheter migration) between the use of straight and coiled catheters (five trials, 308 patients—RR: 0.65; 95% CI: 0.37 to 1.14), but heterogeneity in this analysis was significant (heterogeneity X2 = 15.37, I2 = 74.0%).
Conclusions: In this meta-analysis, no advantage is achieved by inserting catheters with a coiled intraperitoneal portion.
Catheter Migration in Adults on Peritoneal Dialysis: A Prospective Comparison of Two Types of Peritoneal Catheters
Objectives: Current clinical practice guidelines indicate that no particular type of peritoneal dialysis (PD) catheter has been proved superior to another. PD catheter survival is challenging because of infection and malfunction. We evaluated clinical outcome for two types of PD catheters, the standard double-cuff Tenckhoff catheter (TC) and the double-cuff swan-neck Tenckhoff catheter (SN).
Methods: In this prospective study in a single-center setting, patients implanted by the open surgical method were randomized to receive either a TC or a SN from January 2007 to November 2008. All patients were followed at 6 months. The primary outcome was catheter tip migration at 6 months; the secondary outcomes were catheter-related peritonitis at 6 months, catheter survival at 6 months, and surgery-related bleeding.
Results: The study enrolled 208 consecutive patients: 91 in the SN group, and 117 in the TC group. At 6 months, more significantly different catheter tip migration was observed in the SN group than in the TC group (19/91 vs. 10/117, p = 0.011). However, peritonitis episodes within 6 months were similar in the SN group and in the TC group (10/91 vs. 14/117, # p = 0.827). Catheter survival within six months was 83/91 (91.2%, 8 switching to hemodialysis) in the SN group and 107/117 (91.5%, 5 switching to hemodialysis, 3 undergoing transplantation, 2 dying) in the TC group (p = 0.950). Exit-site and main wound bleeding post surgery were generally mild and similar in the two groups. No dialysate leakage or subcutaneous cuff protrusion events were observed in either group.
Conclusions: Placement of the double-cuff swan-neck Tenckhoff catheter appears to result in higher catheter migration, and no benefit is achieved.
An Original Non Traumatic Maneuver for Repositioning Migrated Peritoneal Dialysis Catheters
Objectives: To describe an original non traumatic maneuver for repositioning migrated peritoneal dialysis (PD) catheters (caths).
Methods: Our method includes dissociation, determination of the return route, and manual repositioning.
In dissociation, the dialysate is partially drained, and clockwise and anticlockwise movement are used to lessen the pain at the migration site, after which gentle force is used to dissociate the greater omentum that possibly wraps around the cath.
In determination of return route, a return route is designed based on the position of the catheter in the abdominal radiograph (right and left upper quadrants and right lumbar; epigastrium; left lumbar; right or left iliac fossa).
In manual repositioning, five steps of (1) pressing; (2) palpating; (3) vibrating; (4) wave vibrating, and (5) rotating to move the cath to the epigastrium. At this point, the patient can sit up and lean slightly back, with the upper limbs resting on the arms of chair, both knees flexed, feet touching the ground, and the whole body relaxing naturally.
Three more steps of (6) back-pushing and vibrating; (7) swaying; and (8) compressing are then used to complete the maneuver.
Results: The success rate for manual repositioning using this procedure is usually high within 12 h from onset of migration signs and radiologic confirmation. Of 30 cases of PD cath migration, repositioning was successful 1 time in 9 cases, 3 times in 10 cases, 7 times in 7 cases, and failed in 4 cases. The overall success rate was 86.7%.
Conclusions: Manual repositioning of the PD cath is safe, painless, economic, and feasible, and may be attempted before referring for more invasive interventions.
Catheter Migration Incidence and Related Factors in Peritoneal Dialysis Patients
Objectives: In peritoneal dialysis (PD) keeping the dialysis catheter (cath) unblocked is important. Among 320 patients (pts) undergoing continuous ambulatory peritoneal dialysis (CAPD) since 2000 in our hospital, X-ray examination 2 weeks after PD start revealed cath migration in 26 of 204 pts (8.13%). This study reviews and analyzes treatment measures for cath migration.
Methods: In the 320 chronic renal failure pts (186 men, 134 women; mean age: 45 ± 13 years), there were 202 pts with chronic nephritis, 52 with hypertensive renal arteriolar sclerosis, 44 with diabetic nephropathy, 12 with chronic pyelonephritis, and 10 with other primary diseases. CAPD was performed using double-cuff permanent Tenckhoff caths, which were placed using a peritoneoscope to guide the cath into the abdominal cavity in 26 pts and using direct surgical vision and local anesthesia in 294 pts. Pts started with intermittent PD and switched gradually to continuous ambulatory PD. The incision was below the navel in 26 pts (a peritoneoscope was inserted into the peritoneal cavity 3 cm above the navel at the left lateral rectus abdominis), paramedian at the lower abdomen in 240 pts, median at the lower abdomen in 46 pts, and counter-McBurney at the lower abdomen in 8 pts. When placed under direct surgical vision, the cath exit was located at the right abdomen. Cath migrations were observed immediately to 7 days after PD start.
Results: By X-ray examination, caths placed under direct surgical vision migrated to the left upper abdomen in 12 cases, right upper abdomen in 5 cases, middle abdomen in 2 cases, below septum in 1 case, left iliac fossa in 3 cases, and right iliac fossa in 3 cases; caths placed under laparoscopic visualization migrated to the right iliac fossa in 1 pt. Cath migration was corrected from a subcutaneous tunnel using brass wires in 16 cases, through the exit of the subcutaneous tunnel to the median exit at the upper umbilicus using brass wires in 16 cases, and by cath replacement using brass wires in 1 case.
Conclusions: Cath migration, a key factor that influences PD, might be related to the method of cath placement, posture, buoyancy, and organs. Operators should be proficient in cath placement and should pay special notice to whether pts had awareness of defecation at cath placement. Cath migration is best corrected through a subcutaneous tunnel using brass wires. Routine abdominal X-ray in the front and lateral position should be taken within 2 weeks after PD start.