
Abstract

Body Composition, Plasma Adiponectin Level, and Mortality in Chinese Dialysis Patients
Objectives: Adiponectin (ADPN) is an anti-inflammatory adipocytokine. Previous studies have shown that body mass index (BMI) and visceral fat mass correlate negatively with plasma ADPN level. However, BMI in most Chinese dialysis patient is in general lower than 25 kg/m2 (non obese patients), which may be different from the situation in Western dialysis patients. We studied the relationship between body composition, plasma ADPN, and risk of all-cause mortality in Chinese dialysis patients.
Methods: Between January 1, 2005, and September 1, 2006, we recruited 122 patients (61 on hemodialysis, 61 on peritoneal dialysis) and 14 healthy volunteers (mean age: 54 ± 11 years; 7 men, 7 women). Plasma ADPN after an overnight fast was measured by ELISA. Plasma lipid profile and albumin were measured using standard methods. Every patient was followed prospectively, and outcomes were recorded until July 2008. Mean follow-up was 31 ± 11 months (range: 9 – 45 months). Body fat mass was measured using a body composition analyzer (Tanita Corp, Tokyo, Japan).
Results: ADPN was significantly higher in dialysis patients than in the healthy control group (2.90 ± 2.83 mg/L vs. 1.59 ± 0.82 mg/L, p = 0.003). The square root of plasma ADPN [SQRT (ADPN/mg/L)] correlated positively with BMI and visceral fat mass (r = 0.398, p < 0.001), total body fat mass (r = 0.248, p =0.039), and serum triglycerides (r = 0.282, p = 0.018). Age and sex did not correlate with ADPN in the dialysis patients. No correlation was found between BMI and ADPN in the healthy control group. Multiple stepwise regression analysis showed that BMI was the determining factor of ADPN. Comparison of baseline characteristics between patient who survived and patients who died on dialysis showed that deceased patients had a lower BMI, older age, higher prevalence of pre-existing cardiovascular disease, lower albumin, lower lean body mass, and lower ADPN. Cox regression analysis showed that independent risk factors for all-cause mortality were pre-existing cardiovascular disease, BMI (lower BMI), and age (older age), but not plasma ADPN.
Conclusions: Our study showed that, in contrast to previous findings, BMI, visceral fat mass and total body fat mass correlate positively with plasma ADPN in Chinese dialysis patients, and that patients with lower ADPN levels experienced higher mortality, which may reflect the impact of nutrition status on ADPN.
Epidemiology of Chronic Renal Failure in Mexican Patients on Peritoneal Dialysis—Preliminary Report
Introduction: Chronic renal failure is considered a catastrophic disease because of a rising incidence, high costs, limited resources, delayed detection, and rates of mortality in dialysis programs.
Objectives: To identify general the demographic characteristics of the population on peritoneal dialysis at the Instituto Mexicano del Seguro Social (IMSS).
Methods: Our retrospective cross-sectional study ran from 5 January to 30 April 2009 and collected data on dialysis type, age groups, causes of chronic renal failure, annual percentage growth by modality, frequency of peritonitis, causes of mortality, survival, and number patients from level 2 medical units of the IMSS.
Results: The study included 115 medical units (18 regional and 97 general hospitals) in 22 states of the Mexican Republic. Of 20 702 registered patients, 11 135 (54%) were male and 9 567 (46%) were female (ratio: 1.1:1); 19 439 (94%) were adult and 1 263 (6%) were pediatric cases; the 60 – 69 age group was the most prevalent. The causes of chronic renal failure were diabetes mellitus (43%), arterial hypertension (17%), chronic glomerulonephritis (14.4%), undetermined (9.2%), polycystic kidney disease (4.7%), congenital malformations of the urinary tract (a%), lupus nephropathy (3.3%), and others (4.4%). The annual peritonitis rate in continuous ambulatory peritoneal dialysis (PD) was 40.74% (range: 12.59% – 85.04%) and in automated PD, it was 46.07% (range: 5.13% – 87%). The causes of death were similar in both programs: cardiovascular diseases (42%), infection 31%, complications of metabolic alterations and acid–base balance (8%), respiratory failure (2%), hypovolemic shock (2%), and others (15%). Survival was 30.6 months on average (range: 16 – 60 months). The annual percentage growth of the continuous ambulatory PD program was 6.38%, while automated PD declined by 0.31%.
Conclusions: The IMSS provides the most dialysis coverage in Mexico and handles the most patients on dialysis. The general conditions of the study population are similar to those reported in the literature from other Latin American countries. Mexico does not have a national renal data registry. Opportunities exist to improve dialysis results.
Protocols for Change of Transfer Set in Continuous Ambulatory Peritoneal Dialysis: New versus Old
Introduction: The PD extension catheter (transfer set) is usually changed every 6 months (or earlier, if contaminated). The change of transfer set (COTS) must be performed with strict aseptic technique to avoid contamination and risk of peritonitis. Recently, we adopted a new COTS protocol which requires fewer steps and fewer disposables. We evaluated the effects of this new protocol on our patients’ care.
Objectives: To compare the cost of disposables, duration of procedure, exit-site cultures, and peritonitis rates up to 6 weeks post-procedure between the new and the former COTS protocols in our continuous ambulatory peritoneal dialysis (CAPD) patients.
Methods: This prospective randomized controlled study involved patients who had been on CAPD for ≥6 months, with their last COTS at ≥3 months earlier. Patients with an exit-site infection or peritonitis within ≤6 months were excluded. Exit-site swabs were taken for culture at baseline, 2 weeks, 4 weeks, and 6 weeks post-procedure. The peritonitis incidence was recorded.
Results: The study included 24 patients (13 new protocol, 11 former protocol; mean age: 41.7 ± 13.9 years). Disposables cost less with the new protocol (RM34.60 vs. RM47.60; ΔRM13.00). The new protocol also has fewer steps (13 vs. 16) and takes a shorter time to complete (20 min vs. 30 min; Δ 10 min). There were no differences in the rate of positive exit-site cultures between the groups (new protocol: 4 positive cultures; former protocol: 6 positive cultures; p = nonsignificant). Peritonitis unrelated to the procedure developed in 2 patients (1 from each protocol).
Conclusions: Compared with the former protocol, the new COTS protocol is more economical, has fewer steps, and requires a shorter time. More importantly, the new protocol does not increase the rate of positive exit-site cultures or peritonitis.
Comparison of Low-Dose Deferoxamine with Standard-Dose Deferoxamine for Treatment of Aluminum Overload in Dialysis Patients
Background: Dialysis patients (pts) are at high risk of Al overload. Deferoxamine (DFO) has potential dose-dependent adverse effects, but lower DFO dosages may afford good efficacy with fewer side effects. The standard weekly treatment dosage is 5 mg/kg for 2 months, as suggested by the Kidney Disease Outcomes Quality Initiative (K/DOQI) guidelines. We compared the therapeutic response to low-dose (2.5 mg/kg) and standard-dose DFO in dialysis pts with Al overload.
Methods: We used basal pre-dialysis serum Al levels of ≥20 μg/L with clinical suspicion of Al toxicity, or hyperparathyroidism indicating parathyroidectomy, and positive DFO tests to recruit hemodialysis (HD) and peritoneal dialysis (PD) pts for the study. The pts were randomly divided into standard-dose and low-dose groups. We compared mineral, biochemical, and hematologic parameters before and after 2 months of treatment with DFO. Successful treatment was defined as a serum Al increase of <50 μg/L by DFO test. Adverse events involving DFO were also compared.
Results: In total, 42 HD pts completed DFO treatment (21 in the standard-dose group, 21 in the low-dose group), but no PD pts fit the diagnostic criteria of Al overload. The demographic characteristics of the two groups did not differ. Serum corrected Ca and ferritin declined in both groups, and serum total alkaline phosphatase increased in both groups. Serum P increased in the low-dose group (p = 0.029), and plasma intact parathyroid hormone increased in the standard-dose group (p = 0.004). The successful treatment response rates did not differ between the two groups [12/21 (57%) in the standard-dose group, 13/21 (62%) in the low-dose group; p = 0.75). Total adverse events were fewer in the low-dose group, although the difference with the high-dose group was not significant.
Conclusions: Low-dose DFO may offer HD pts a similar therapeutic effect and a safer method of Al overload treatment. Although no PD pts completed DFO treatment in this study because of a relatively lower prevalence of Al overload, low-dose DFO may represent an alternative and safer treatment for PD pts with Al overload.
Evaluation of Factors Affecting Nephrologists’ Non Eligibility Criteria for Peritoneal Dialysis: A Conjoint Analysis
Background: In Japan, fewer than 5% of end-stage renal disease (ESRD) patients (pts) select peritoneal dialysis (PD) as their renal replacement therapy (RRT). In Kyushu University Hospital, fewer than 30% of ESRD pts chose PD although the clinical support system is prepared to receive them. We therefore suspected that some undetermined factors are subconsciously influencing the nephrologists when they make the decision about the RRT modality suitable for each pt.
Objectives: This study used a conjoint analysis method to investigate the factors that nephrologists regard s making a pt unsuited to PD.
Methods: We developed a series of 20 written hypothetical case simulations that varied with respect to 6 clinical characteristics: diabetes mellitus, anatomic concerns (adhesions, hernia, obesity), physical disabilities (visual disturbance, gait disturbance), pt preference for RRT modality, social factors, and self care. The questionnaire containing the 20 simulated cases was completed by 12 nephrologists working in our hospital. They were presented with the 20 profiles of hypothetical cases and were then asked in each case: “Is this case eligible for initiation of PD?” Each response was graded on a 3-point scale: “Certainly yes,” “Probably yes,” and “Probably no.”
Results: Of the 6 clinical characteristics, “patient preference” had the most impact on the nephrologists’ preference for PD. Among the three levels of “patient preference,” the most unsuitable choice was “Patient preference for hemodialysis (HD),” and the factor that nephrologists regarded as making a pt most unsuited for PD was “patient's sanitary control” in the characteristic of “patient's self care.” In contrast, poor dietary control did not discourage nephrologists from initiating PD. Of all the levels included in the 6 clinical characteristics, the levels that nephrologists recognized as making a pt unsuited to PD were “poorly-controlled diabetes mellitus,” “peritoneum with adhesion,” “gait disturbance,” “pt preference for HD,” “lack of family support,” and “inability to keep sanitary control.” We also calculated “ineligible scores for PD” by utility scoring of conjoint analysis.
Conclusions: Based on the hypothetical cases, our study clarified the factors affecting nephrologists’ determination of non eligibility for PD. In our next research project, we will apply “ineligible scores for PD” to actual pts to investigate whether the pts generally assessed as ineligible for PD are not really suited to PD.
What Influences Ability to Retain Knowledge or Skill in Performing Peritoneal Dialysis in Thai Patients?
Introduction: In Thailand, “peritoneal dialysis (PD) first” policy was implemented in January 2008. The objective of the policy is to expand health care coverage under the Universal Healthcare Coverage Scheme to patients (pts) with end-stage renal disease. PD needs a holistic approach and a chronic care model—key factors for successful therapy. Pt motivation, family or social support, and knowledge and skill for performing PD at home all need to be maintained along the course of therapy. Our study looked at factors that influence the ability to retain knowledge and skill for performing PD at home after the first training at the beginning of therapy.
Methods: This cross-sectional and descriptive study enrolled 152 pts from three separate centers. The pt data obtained were categorized into baseline characteristics and a general assessment of the pt's knowledge (paper tests, and a home-visit scorecard). After data collection, we looked for the factors that would influence ability to retain the knowledge and skill for performing PD.
Results: The score from the paper tests divided into two parts: on nutrition, the average score was 8.7 ± 0.017 out of 10, and on the exchange procedure and exit-site care, the average score was 9 ± 0.011 out of 10. On the home-visit scorecard, the average score for housing was 227 ± 22.44 out of 250. The average score for the exchange procedure was 232.7 ± 25.85 out of 250. Scores from the paper tests and the home-visit scorecard were comparable in male and female pts. In the age groups of under 15 and over 70 years of age, the score from the two paper tests was lower than in any other age group. In uneducated pts (as compared with a group of educated pts), the scores from paper test 2 and the home-visit exchange procedure were lower. But pts with an education at the primary level received scores from all parts of the evaluation that were comparable with scores from a group of pts with more education. If we consider the time elapsed from the first training (less or more than 90 days), scores were comparable in both groups. In patients with and without a history of peritonitis, we analyzed differences in the scores from paper tests and the home-visit scorecard, and we found that a history of peritonitis was associated with lower scores on both portions of the evaluation.
Conclusions: Many factors can influence the ability to retain knowledge and skill in performing PD. If PD centers can detect declining knowledge early, many PD complications can be prevented.
Evaluation of Health Education Effect in Peritoneal Dialysis Patients
Objectives: To uncover faulty concepts and weak peritoneal dialysis (PD) knowledge common in PD patients by examinations after health education, and to summarize the theoretical evidence for further training.
Methods: Examinations of PD knowledge were given to 42 PD patients making follow-up visits to our outpatient department in January 2009. The examination included 100 questions about basic PD knowledge, concepts of asepsis, safe PD exchanges, management of the catheter and exit site, body fluid balance and proper diet, medications being taken, purchase and storage of PD supplies, and problem-solving in daily life. Questions were scored as 1 point each. General information on the patients was also recorded.
Results: The 42 patients (20 men, 22 women) had a mean age of 61.2 years. Average PD duration in the group was 15 months. The data concerning highest educational background revealed 24 patients below senior high school (11 with primary school or less, 13 with junior high school or less),18 patients with senior high school and above (11 with senior high school, 9 patients with university or college). Primary kidney diseases included diabetic nephropathy (n = 7), hypertension-related nephropathy (n = 10), chronic glomerulonephritis (n = 10), hemolytic uremic syndrome (n = 1), obstructive nephropathy (n = 2), aristolochic acid nephropathy (n = 2), Alport syndrome (n = 1), and polycystic nephropathy (n = 1). Scores of better than 90 were recorded in 14 patients (33%), and scores between 60 and 90 in 26 patients (62%). Scores of less than 60 were recorded in 2 patients (5%). The highest error rates were 71.4% (questions about basic PD knowledge),69.1% (questions about asepsis concepts), and 66.7% (questions about medications being taken). Elderly patients (≥60 years of age), those with a longer PD duration (≥6 months), and more poorly educated patients scored lower in questions about basic PD knowledge and asepsis concepts (p < 0.05).
Conclusions: PD patients, especially elderly ones (≥60 years of age) and those on PD for more than 6 months should receive repeated training, after their initial training has been given.
Analysis of Clinical Status among End-Stage Renal Disease Patients at a Tertiary Care Centre in China: Role of Pre-dialysis Follow-Up
Objectives: Our retrospective study examined factors influencing the choice of dialysis modality among incident dialysis patients. Special efforts were made to assess clinical conditions at the initiation of peritoneal dialysis (PD) and the potential difference in the consequences of follow-up versus no follow-up in pre-dialysis patients.
Methods: From 1 January 2006 to 31 October 2008,233 incident dialysis patients entered the study. We established regression models to analyze the relationship between choice of dialysis modality and demographic, socioeconomic, clinical, and laboratory characteristics. Altogether, 206 PD patients were allocated to one of two groups depending on follow-up status. We then compared residual renal function (RRF), nutrition status, comorbidities, and the timing of dialysis initiation between the two groups.
Results: Hemodialysis was chosen by 38 patients, and PD by 195. Independent predictors for choosing PD over HD were residence in the outskirts of Beijing (p = 0.009), regular follow-up before the start of dialysis (p = 0.034), and non free medical care (p = 0.017). Compared with PD patients lacking pre-dialysis follow-up, patients who received such follow-up had significantly higher RRF, serum albumin, hemoglobin, rate of erythropoietin utilization, and rate of timely dialysis initiation (p < 0.01); conversely, nutrition status was worse in patients lacking pre-dialysis follow-up (p = 0.005).
Conclusions: Our study associated the selection of PD with several socioeconomic and pre–end-stage renal disease factors, and it underscored the importance of pre-dialysis follow-up in improving PD utilization. The clinical condition of patients starting dialysis without previous specialist follow-up was worse than that of patients receiving adequate nephrology follow-up. Such patients might miss the optimal timing of dialysis initiation.
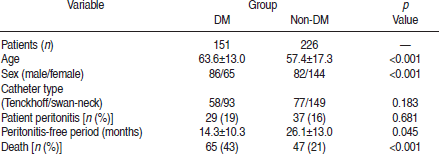
Predictors of Survival in End-Stage Renal Disease Patients on Continuous Ambulatory Peritoneal Dialysis: Diabetes versus Non Diabetes
Objectives: To analyze overall predictors of survival in end-stage renal disease (ESRD) patients on continuous ambulatory peritoneal dialysis (CAPD).
Methods: We evaluated 377 patients [151 (40.1%) with diabetes (86 men, 65 women); 226 (59.9%) without diabetes (82 men, 144 women)] who started CAPD between November 1996 and December 2008 at our institution (mean follow-up: 26.5 ± 15.3 patient–months). Data concerning sex, age, primary disease, comorbidities, follow-up duration, cause of death, and cause of technique failure were collected.
Results: Patients were prospectively followed to the end of the study or to death. Overall patient survival was 88%, 78%, 69%, 57%, 50%, and 23% at 1, 2, 3, 4, 5, and 10 years respectively. Patient survival rates for those with diabetes were 81%, 67%, 52%, 38%, 33%, and 13% respectively. Patient survival rates for those without diabetes were 93%, 85%, 81%, 71%, 62%, and 37% respectively. The relative risk of mortality for nondiabetic patients (47/226, 21%) was less than that for diabetic patients (65/151, 43%, p < 0.001). Using Cox regression analysis to analyze the overall predictors of mortality, diabetes status [odds ratio (OR): 2.327; 95% confidence interval (CI): 1.571 to 3.447; p < 0.001] and age (OR: 1.036; 95% CI: 1.008 to 1.054; p < 0.001) were significant predictors in our CAPD patients. Sex, peritonitis, serum albumin, and cardiovascular comorbidities were not significant risk factors.
Conclusions: Considering increases in the number of elderly patients and in the cases of ESRD caused by diabetes, patient survival has improved overall. Mortality in CAPD is still high among older diabetic patients. More-careful management of higher risk groups will be needed to improve the outcomes of CAPD patients in the future.
Clinical Outcomes of Systemic Lupus Erythematosus Patients Undergoing Continuous Ambulatory Peritoneal Dialysis or Hemodialysis
Objectives: To evaluate outcome in patients with systemic lupus erythematosus (SLE), who are being treated with continuous ambulatory peritoneal dialysis (CAPD) or hemodialysis (HD).
Methods: We compared 16 SLE patients who had been undergoing CAPD (n = 11) or HD (n = 5) for at least 3 months in our unit with 32 other age- and sex-matched nondiabetic CAPD patients with an underlying primary diagnosis of chronic glomerulonephritis (CGn). Clinical outcome, infectious complications, lupus activity, and biochemical parameters were reviewed.
Results: The duration of dialysis in the two study groups was not significantly different (mean: 26.4 ± 8.3 months in the SLE group, 28.7 ± 6.8 months in the CGn group). Before dialysis, SLE patients had a significantly lower albumin level (30.0 ± 3.6 g/dL vs. 37.4 ± 7.8 g/dL, p < 0.01); however, mean hemoglobin was similar in the two groups. The SLE group had a higher peritonitis rate (1 episode in 42 patient–months vs. 1 episode in 78 patient–months, p < 0.05). Cardiovascular diseases were more common in the SLE group (75% vs. 30%, p = 0.047). The number of patients who received a kidney graft was similar in both groups. During the follow-up period, 4 patients died, and the overall mortality rate was higher in the SLE group (2/16; 1 on PD, 1 on HD) than in the control group (2/32), but the difference was not statistically significant.
Conclusions: Patients with SLE who are being treated with CAPD or HD have a significantly lower pre-dialysis serum albumin level and a poorer prognosis in terms of infectious complications and mortality.
Serum Levels of Fibroblast Growth Factor 23 in Continuous Ambulatory Peritoneal Dialysis Patients
Objectives: To detect serum levels of fibroblast growth factor-23 (FGF23) and vitamin D in patients on continuous ambulatory peritoneal dialysis (CAPD) and to compare those data with data from patients on hemodialysis (HD).
Methods: Serum FGF23 was detected by enzyme-linked immunosorbent assay (ELISA) in a cohort of 54 end-stage renal disease patients on dialysis therapy [CAPD: n = 24; mean age: 69.8 ± 10.8 years; average dialysis duration: 22.4 ± 13.3 months; HD: n = 30; mean age: 54.8 ± 15.5 years; average dialysis duration: 52.4 ± 16.9 months] and in 20 healthy controls. Concentration of serum 1,25-(OH)2VitD3 was measured by enzymatic immunoassay (EIA). Serum levels of intact parathyroid hormone (iPTH), creatinine, albumin, Ca, and P were determined.
Results: Serum FGF23 was significantly higher in patients on CAPD (87.85 ± 33.65 ng/L) and HD (88.51 ± 35.0 ng/L) than in control subjects (11.76 ± 3.63 ng/L). Moreover, the concentration of serum 1,25-(OH)2VitD3 was lower in CAPD and HD patients than in the control group (24.31 ± 7.11 pmol/L vs. 48.37 ± 3.47 pmol/L; 19.82 ± 4.99 pmol/L vs. 48.37 ± 3.47 pmol/L), and the level of 1,25-(OH)2VitD3 was much lower in HD patients than in CAPD patients. By Pearson correlation analysis, serum FGF23 was positively correlated with serum creatinine, P, iPTH, and duration of dialysis. FGF23 was negatively correlated with 1,25-(OH)2VitD3.
Conclusions: Serum FGF23 is significantly upregulated in CAPD patients, and serum 1,25-(OH)2VitD3£¿ is downregulated. Serum creatinine, P, iPTH, and 1,25-(OH)2VitD3 are the major regulators that influence FGF23.
Onychomycosis in Patients Undergoing Peritoneal Dialysis
Objectives: Onychomycosis is highly prevalent in end-stage renal disease. Our study compared the prevalence of onychomycosis in patients on peritoneal dialysis (PD) with that in a healthy cohort, and evaluated the potential relationships between onychomycosis and various demographic, medical, and laboratory parameters in these subjects.
Methods: Our study included 96 patients with chronic renal failure undergoing PD over a period of 6 months, and 96 healthy control subjects of matched age and sex. Both groups underwent full history-taking and a thorough general and nail examination. In all patients, duration of PD, dialysis efficacy (Kt/V), residual renal function (RRF), peritoneal transport type, hemoglobin, neutrophil count, Ca, P, albumin, siderophilin, creatinine, urea, fasting blood glucose level, alkaline phosphatase, and parathyroid hormone (PTH) were determined, and compared by multivariate analysis.
Results: Onychomycosis was present in 18 patients in the PD group and in 12 healthy controls. The prevalence rate was significantly higher in the PD group (18.75%) than in the control group (12.5%). The prevalence of onychomycosis was not significantly influenced by duration of PD treatment [which ranged from 6 months to 132 months (mean: 52 ± 25 months)]. Peritoneal equilibration test revealed these peritoneal transport types: high (H), 31.25%, and low (L), 68.75%. Onychomycosis was more highly prevalent in H patients than in L patients, but the difference was nonsignificant. Dialysis efficacy (Kt/V) was not associated with onychomycosis. Multivariate analysis revealed that the presence of diabetes mellitus and lower levels of RRF and albumin were significantly associated with onychomycosis. There was no significant correlation between onychomycosis and hemoglobin or Ca.
Conclusions: Uremic patients undergoing PD therapy have higher rates of onychomycosis than do healthy people. Diabetes mellitus has been shown to be an independent risk factor for the development of onychomycosis. Efficient PD dose not improve onychomycosis. We hypothesize that uremia and associated comorbidities may play a causal role in the development of onychomycosis. By conserving RRF as far as possible in PD patients, it may be possible to slow the development of onychomycosis. In addition, improving nutrition in these patients is beneficial.
High Systolic Blood Pressure during Follow-Up Predicts Mortality in Peritoneal Dialysis Patients
Objectives: Systolic blood pressure (SBP) is an independent risk factor for mortality in the general population. Recent studies have demonstrated discrepant results for the relationship between blood pressure and mortality in peritoneal dialysis (PD) patients. This retrospective study investigated whether high SBP during follow-up is associated with increased mortality in PD patients.
Methods: Our study involved 128 PD patients who began PD treatment between 1 January 1999 and 31 December 2005 at the Nanjing University hospital in Nanjing, PR China. All patients were followed to the end of 31 December 2008 or death. Baseline demographic, clinical, biochemical, and dialysis data were collected. Patients were stratified into tertiles according to their averaged SBP during follow-up. The relationship between follow-up SBP and all-cause mortality was then evaluated using a Cox regression model.
Results: The overall 1-, 3-, and 5-year survival rates of our patients were 95%, 59%, and 33% respectively. Mean survival time was 38 ± 19 months. Of the 128 patients, 95 died during follow-up. The upper tertile experienced a significantly higher rate of mortality than did the middle and lower tertiles (p < 0.05); there were no differences between the middle and the lower tertiles. In the Cox model, with each 1-mmHg increase in SBP was associated with a significant 3.1% increase in all-cause mortality (p < 0.01).
Conclusions: SBP during follow-up is an independent predictor of mortality. More attention should be paid to hypertensive PD patients during follow-up.