
Abstract

Biochemical Markers of Osteoblast Activity, Clinical Variables, and Association with Arterial Calcification in Incident Peritoneal Dialysis Patients
Objective: Our aim was to know the association of biochemical markers of osteoblast activity and clinical variables with arterial calcification in incident patients on peritoneal dialysis.
Methods: We included 36 incident patients on peritoneal dialysis, of which 80% were on DPCA and 20% on DPA. Demographic and clinical data were recorded. Arterial calcification (AC) was evaluated in the abdominal aorta and pelvic vessels with simple phase using 4-cut computerized multi-detector tomography (MCST), Philips Mx 8000, and x ray in the abdominal aorta and pelvic. We measured in serum total Ca, phosphorus, albumin, globulin, glucose, and creatinine with immunoturbidimetric assay (Roche/Hitachi 902 Germany); osteocalcin (OT) osteoprotegerin (OPG), iPTH, IL-6, and IL-8 were measured by Milliplex™ kit.
Results: Mean age was 49±11, BMI 24±4, 70% male, 65% with diabetic nephropathy as a cause of disease, 65% with type 2 diabetes; time in dialysis was 1.5±1.2 months. We did not find calcifications in the lateral abdomen with x ray. The patients were classified in 2 groups according to calcification through tomography: without calcification, group 1=42% and group 2 with AC=58%. Group 1 was younger (44±13 vs 53±7 years; p<0.05), had significantly higher mean OT (29721±17919 vs 18494±6330, p<0.03); lower IL-8 (10.1±3.1 vs 13±5.3; p<0.05). Diabetes and diabetic nephropathy as a cause of disease were more frequent in group 2.
Conclusions: Osteocalcin, type 2 diabetes, and age were associated with calcification measurements through tomography in incident peritoneal dialysis patients.
Low Calcium Peritoneal Dialysis Solutions Improve Mineral Metabolism Parameters in Patients with Low PTH Levels
Objective: Low level of PTH is a common finding in peritoneal dialysis (PD) patients and is considered an important factor associated with higher risk of developing fractures and cardiovascular disease. A positive calcium balance occurs with the use of 3.5 mEq/L of calcium PD solutions and induces a blockage in PTH production. Current guidelines suggest that PTH-i levels in end-stage renal disease should be kept in the range of 150–300 pg/mL. The purpose of this study is to evaluate 6-month serum PTH-i response after PD solution conversion from 3.5 mEq/L of calcium to 2.5 mEq/L of calcium PD solution in patients with baseline PTH-i levels less than 150 pg/mL.
Methods: This prospective, observational study included all prevalent patients (at least 90 days on therapy) on PD in a single center from January 2008 to May 2009. The inclusion criteria were (1) at baseline be in use of a PD solution with 3.5 mEq/L of calcium for at least 90 days; (2) 2 repeated measures of PTH-i with 6 months of interval, and (3) baseline PTH level <150 pg/mL. The group that switched to low calcium was compared to the group maintained in 3.5 mEq/L solutions (control group).
Results: 35 patients (mean age 62±17 years) were included in the study. Diabetic nephropathy (36%) was the main underlying renal disease, followed by hypertensive nephrosclerosis (25%) and chronic glomerulonephritis (14%). Of these, 22 were converted to use 2.5 mEq/L of calcium PD solutions. Among patients switched to low calcium solution 40% reached the target values (PTH 150–300 pg/mL) compared to 14 in the control group (p<0.05). There were no significant differences between groups regarding calcium, phosphorus, and alkaline phosphatase at baseline as well as 6 months after conversion.
Conclusions: In patients with PTH <150 pg/mL conversion to low calcium solutions (2.5 mEq/L) appears to be a simple and effective strategy to bring PTH levels to the range determined by currently guidelines.
Oral Paricalcitol in Peritoneal Dialysis (PD): Treating Secondary Hyperparathyroidism
Objective: Oral paricalcitol is a vitamin D analogue which shows significant reduction in iPTH levels, causing less episodes of hypercalcemia than calcitriol in predialysis and hemodialysis (HD) patients (pts). Aims: Evaluate oral paricalcitol efficacy to reduce levels of iPTH in PD pts. Analyze the stability of calcium (Ca) and phosphorus (P) levels. Methods: Controlled prospective study, with therapeutic intervention. Pts were selected from a PD center with 50 pts, to whom it was previously difficult to achieve the control of iPTH, P, or Ca levels with sevelamer or cinacalcet. Pts were excluded if they had hyper-Ca or frequent and recent complications of PD technique. Pts were followed for 24 months in routine consultations, monitoring iPTH, Ca, and P. Medication was adjusted to reach the K/DOQI goals. Results: From 14 pts selected, 4 were excluded: 2 were transferred to HD and 2 were submitted to renal transplantation. 10 adult pts were followed for 24 months. 5 men; age 49±8.8 years. 50% APD. Time in PD 49±21.1 months. 20% anuric. CKD etiology: 4 chronic glomerulonephritis; 2 DM2; 1 DM1; 2 unknown; 1 ADPKD. Levels of iPTH were reduced from 670±333.8 to 534.28±477.1 pg/mL (p=0.01). There were occasional episodes of hyper-Ca (7/90 measurements) in 4/10 pts. Paricalcitol was stopped in 2 pts at 15 and 21 months of treatment and the levels of iPTH raised as the levels of Ca went down. Mean values of initial P were 5.2 mg/dL and kept stable during the study. At the end, 60% of the pts had levels of P between 3.5–5.5 mg/dL; 30% >5.5%. At the end of the period all the pts had Ca between 8.1–9.9 mg/dL. Ca×P kept stable (44±11.7). Mean given dose of paricalcitol was 1.1±0.32 at the beginning and 1±0.67 μg/day at the end of the study. There were no significant changes in cinacalcet or sevelamer dose. Conclusions: In the group studied, during 24 months, iPTH was effectively reduced and there was an adequate control of P and Ca levels, with cinacalcet and sevelamer plus oral paricalcitol. However, paricalcitol had to be stopped in 2 pts because of hyper-Ca. These results highlight the difficulty in controlling the bone metabolism in PD pts, showing, however, that, in this population, oral paricalcitol could be used to lower PTH.
Predictors of Bone Mineral Density (BMD) in Peritoneal Dialysis (PD) Patients
Objective: Mineral bone disease is frequent complication which increases morbidity and reduces quality of life in patients (pts) with chronic renal disease, especially those on maintenance dialysis treatment. The aim of our study was to assess predictors of BMD in PD pts. Methods: The study was performed in 26 pts treated with PD (15 women, 11 men; dialysis vintage 16.6, 6.3–45.5 months). BMD was measured in the femoral neck using dual-energy x-ray absorptiometry. Associations/correlations between BMD and demographic characteristics, anthropometric measurements assessing nutritional state, and laboratory parameters of examined pts were analyzed. Results: In the stepwise regression analysis, 2 very well-fitted models of independent variables predictive for the femoral neck BMD in PD pts (0.842±0.137 g/cm2) were obtained. The first model (corr. R2=0.988) included serum albumin level as the strongest predictor (3.50±0.45 mg/dL, beta=0.743, p=0.000), lean body mass (51.8±9.7 kg, β=0.504, p=0.000), serum total alkaline phosphatase activity (84.8±36.5 IU/L, β=–0.184, p=0.009), and treatment with acetylsalicylic acid (ASA; 10 treated, 16 non-treated, β=–0.130, p=0.000). The second model (corr. R2=0.982) included blood pH as the strongest predictor (7.37±0.04, β=1.207, p=0.000), serum phosphate concentration (5.37±1.39 mg/dL, β=–0.295, p=0.034), serum creatinine level (8.11±2.90 mg/dL, β=0.260, p=0.014), and metrical age (55.8±17.7 years, β=–0.188, p=0.046). Correlations between BMD and the strongest predictors were described by the equations: the femoral neck BMD (g/cm2) = 0.1807 × albumin (g/dL)2 – 0.0313 × albumin (g/dL)3, and the femoral neck BMD (g/cm2)=0.0021 × pH3. In the second model Hb (11.5±0.9 g/dL, β=0.788, p=0.000) or Hct (34.6±3.0%, β=0.760, p=0.000) could replace phosphates as a predictor of BMD. Conclusions: We expect better preservation of BMD in PD pts by more rigorous treatment of abnormalities in parameters of nutritional status, calcium–phosphate metabolism, acid–base balance, and blood count. PD pts treated with ASA need regular control of BMD.
Therapy for Tumoral Calcinosis in CAPD Patients
Objective: Diphosphonates, such as disodium ethane-1-hydroxy-1, 1-diphosphonate (EHDP) are known to reduce various types of experimentally induced soft-tissue calcification. Ectopic calcification as tumoral calcinosis and peritoneal calcification accompanied with encapsulated peritoneal sclerosis (EPS) may complicate CAPD patients. We administered EHDP for 2 CAPD cases with tumoral calcinosis and another EPS patient with peritoneal calcification. Sevelamer hydrochloride (SH) is the phosphate binder that contains no calcium elements. We experienced a case whose tumoral calcinosis disappeared after changed the phosphate binder from calcium carbonate to SH.
Methods: The first case was 18 year-old female with goose egg sized calcification in her left femoral area after treatment on CAPD for 7 years. She was administered EHDP 400 mg/day orally and had almost complete eradication of calcification after 6 months’ treatment. The second case was 34-year-old female with over-hen egg sized calcification in her left shoulder joint after CAPD treatment for 3 years. EHDP 600 mg/day oral administration for 6 months reduced this calcification. Another case was 41-year-old female with diffuse peritoneal calcification due to EPS after CAPD treatment for 10 years. She was switched to hemodialysis (HD) and was administered EHDP 200 mg/day orally without any change of calcification after treatment for 6 months. The last case was 54-year-old male with hen egg sized calcification in his right hip muscle after CAPD treatment for 4 years. He was switched to HD and SH 9.0 g/day oral administration without calcium carbonate for 8 months reduced this calcification.
Results: Our experience may suggest that the mechanism of calcification between the ordinary tumoral calcinosis in dialysis patients and the calcification accompanied with EPS is quite different. SH may be effective against the tumoral calcinosis due to calcium overload.
Conclusions: The tumoral calcification with no relation to EPS may be possible to be treated.
Calcium, Phosphorus, and Trace Elements in Hair of CAPD Patients: Is There Any Relation with the Bone Mineral Density and T-Score Measurements?
Objective: Disturbance of mineral status in patients with chronic renal failure (CRF) is one of many complications of this disease. Trace elements analysis in hair is sometimes used by clinicians for a diagnosis of mineral status. The aim of this study was to determine the distribution of calcium (Ca), phosphorus (P), and the trace elements in hair of CAPD patients and compare with control healthy group. The relation between those trace elements and the bone mineral density (BMD) and T-score measurements measured by dual-energy x-ray absorptiometry (DEXA) was conducted.
Methods: The cohort of 29 stable CAPD patents [M/F=13/16; median of age 53.0 (44.0–53.9) years; median of dialysis duration 20.6 (8.8–28.0) months], which used PD solution with 1.75 mmol/L Ca concentration and 21 healthy age- and sex-matched people were included as control group. The content of Ca, P, Mg, Al, Zn, Cu, Fe, Mn, and Sr in hair samples was determined using inductively coupled plasma nuclear spectrometry (spectrometer Vista PRO; Varian, USA). Measurements of BMD and T-scores (Ts) at the lumbar vertebrae, left (LF) and right femur (RF) were performed by using DEXA (Hologic QDR 4500 C).
Results: We did not find significant difference between concentration of trace elements in the hair health-control and CAPD patients except Al concentration 14.6 (4.5–14.6) in the hair of CAPD patients and 6.4 (4.3–7.5) in the control group (p=0.001). There were no significant correlations between trace elements concentration in hair and the parameters of DEXA measurements.
Conclusions: We revealed that Al concentration in the hair of the patients on CAPD was 46% higher than the upper normal range in healthy control (normal range 1–10), so high level of potential harmful trace metal would be explained by uncontrolled using of Al-containing medicines (e.g., phosphate-binders, antacids).
Phosphate-Induced Apoptosis in Human Peritoneal Mesothelial Cells in Vitro
Objective: Hyperphosphatemia was known to have significant predictive value of cardiovascular mortality in patients with chronic kidney disease and receiving hemodialysis and peritoneal dialysis (PD). Recently, it has been demonstrated that phosphate uptake through the type III sodium-dependent phosphate cotransporter Pit-1 induced apoptosis of aortic vascular smooth muscle cells and endothelial cells in vitro. The apoptotic effects of hyperphosphatemia will be herein evaluated on human peritoneal mesothelial cells (HPMCs).
Methods: HPMCs were isolated using the trypsin-EDTA method from omental tissue which was obtained from a patient undergoing abdominal surgery. We treated several different phosphate concentration, 1–5 mmol/L and calcium concentration, 1.8 and 2.8 mmol/L on HPMCs to assess the effects of concentration. 24 later after treatment of each concentration of phosphate and calcium, MTT and TUNEL assays were performed to identify cell death and apoptosis. Bax and Bcl-2 were measured by Western blot and caspase-3 activity by a colorimetric assay.
Results: (1) Pit-1 expression on HPMCs was demonstrated by RT-PCR. (2) Apoptosis in HPMCs significantly increased in high concentration of phosphate in a dose-dependent manner, and enhanced in the presence of 2.8 mmol/L calcium instead of 1.8 mmol/L according to TUNEL assay and MTT assay (p<0.001). (3) High phosphate concentrations significantly decreased anti-apoptotic Bcl-2 expression (p<0.05). (4) Caspase-3 activity increased in high concentrations of phosphate.
Conclusions: High concentration of phosphate induces apoptosis in HPMCs by a caspase-related mechanism.
Oral Paricalcitol Experience in Patients on Peritoneal Dialysis (PD)
Objective: Paricalcitol (paracal) is an activator of vitamin D receptors. Paracal's principal function is to selectively regulate concentration of parathormone (PTH). The aim of this study was to evaluate changes of mineral metabolism in patients on PD with secondary hyperparathyroidism (SHPT) after treatment with oral capsules of paracal. Methods: Observational, retrospective, multicenter study conducted in Spain on PD patients which began oral paracal as SHPT treatment. We evaluated demographics and biochemical data as well as paracal doses at baseline and 3 and 6 months. Results: 105 patients (63 men, 42 women) were included. Median age was 61±14 years; median time spent on PD: 24±21 months; Charlson index 6±2. ESRD etiology was chronic glomerulonephritis, 24%; vascular, 20%; diabetic nephropathy, 18%; undiagnosed, 18%; chronic interstitial nephritis 12%; polycystic disease, 8%; systemic diseases, 2%. 68.6% of patients were not treated previously with vitamin D; 29.5% were treated with oral calcitriol and 1.9% with alfa-calcidiol.
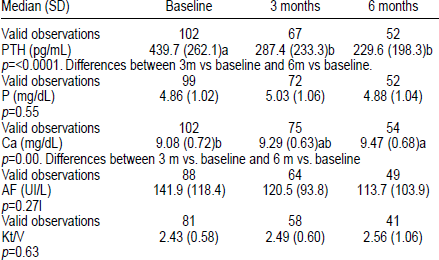
Conclusions: Oral paracal was safe and effective to treat SHPT in PD patients. PTH levels were reduced 51.8% at 6 months. Ca levels increased significantly after treatment with paracal but its levels remained within limits recommended by guidelines. Phosphorus and alkaline phosphatases remained stable after treatment with paracal. Dialysis doses had no influence in PTH control.
Evaluation of Aortic and Coronary Calcification in Peritoneal Dialysis (PD) Patients with Multislice Computed Tomography (MSCT). Correlation with Biochemical Data, Cardiovascular, and Survival Analysis after 12 Months
Objective: Vascular calcification (vasc calc'n) is perhaps the most important medical event regarding calcium–phosphorus metabolism. Aim: To evaluate by MSCT vascular calcification in 42 patients (pts) on PD, comparing the results to the survival parameters and the calcifications evolution at 12 months. Methods: We quantified calcifications (mg calcium) of the thoracic aorta and coronary arteries. 19/42 pts repeated MSCT after 12 months. At the time of MSCT were also determined serum levels of Ca and P, PTHi, alkaline phosphatase, vitamin D [25-(OH)D3], total plasma proteins, triglycerides (TG), cholesterol, CRP, echocardiogram, presence of vascular disease (peripheral or coronary), cardiovascular events, cardiac arrhythmias. Finally, we valuated the survival events (death and/or cardiovascular event) at 60 months according to calcification's index. Results: Mean age 60±14 years, average dialytic age 23.5±44.1 months. Significant correlation between Ca levels in aorta and coronary and age (p<0.01 and p<0.03), significant correlation between calcifications and dialytic age or diabetes only according to the aortic arch (p<0.001), significant correlation between cardiac calcification and coronary disease (p=0.004 and <0.001). Longitudinal study showed, after 12 months, a significant increase in both aortic (p<0.001) and coronary (p<0.001) calcification's index, and a significant decrease in the density of the 9th dorsal vertebra (p<0.001). Otherwise it did not show a difference according to Ca–P metabolism. Univariate survival at 60 months was significantly correlated with Ca values for both sites of vasc calc'n (aorta: p<0.01; coronary: p<0.001). Cox multivariate analysis was not significant for the other parameters analyzed. Conclusions: This work suggests that vasc calc'n has a significant impact on the survival of pts on PD It also suggests that vasc calc'n increases over time and is poorly correlated with biochemical parameters usually used to evaluate of Ca–P metabolism. It is therefore essential to evaluate, at least at the beginning, these calcifications.
Sottini L., Camerini C.,
Are Peritoneal Calcifications in Long-Term Peritoneal Dialysis (PD) Related to Aortic Calcifications and Disturbances in Mineral Metabolism?
Objective: Peritoneal calcifications are more often present in encapsulating peritoneal sclerosis (EPS) patients (pts) than in long-term PD pts without EPS. Case reports have suggested a relation with disturbances in mineral metabolism. Our aim was to investigate whether any relationships between peritoneal calcifications and aortic calcifications or disturbances in mineral metabolism were present. Methods: We included all EPS pts in our center (1996-2008) with a CT scan at the time of diagnosis, and all other long-term PD pts (PD >4 years) who underwent a CT scan for different reasons. The scans were reviewed by 2 radiologists. The presence or absence of peritoneal calcifications was scored and a scoring system for abdominal aortic calcifications was used: 1=none, 2=mild, 3=moderate, 4=severe, and 5=very severe. In each pt, laboratory data on calcium corrected for albumin, phosphorus, and PTH levels were retrieved every 6 months up to 5 years prior to the CT scan. Individual mean values over 5 years were calculated. Information on vitamin D use, possible parathyroidectomies and the total amount of peritonitis episodes were collected. Results: We included 31 pts: 15 EPS pts and 16 long-term PD pts without EPS. 8 EPS pts and 4 long-term PD pts without EPS had peritoneal calcifications. No difference was present between pts with (n=12) and without (n=19) peritoneal calcifications in aortic calcification scores (3 vs 3). Also mean±SD Ca 10.6±0.6 vs 10.4±0.6 mg/dL, P 5.2±1.1 vs 4.8±1.1 mg/dL, and PTH levels 345±254 vs 342±282 pg/mL were not different between pts with and without peritoneal calcifications. PD duration was significantly higher in pts with peritoneal calcifications (103 vs 64 months). Both groups had a similar percentage of vitamin D use and parathyroidectomies, and no difference in peritonitis rates. Conclusions: The presence of peritoneal calcifications in long-term PD pts with and without EPS could not be related to the presence of aortic calcifications or disturbances in mineral metabolism. Local peritoneal factors, such as poor biocompatibility of PD solutions, might be involved in the formation of peritoneal calcifications.
Related Factors Analysis of Serum Phosphorus Level in Continuous Ambulatory Peritoneal Dialysis Patients
Objective: Hyperphosphatemia may worsen hyperparathyroidism and renal osteodystrophy, promote vascular calcification and cardiovascular events, and increase mortality. We present here the related factors of serum phosphorus level in continuous ambulatory peritoneal dialysis (CAPD) patients.
Methods: Cross-sectional, descriptive study of CAPD patients from January to December 2009 in our center was performed. Demographic data, basic nephropathy, biochemical data, peritoneal transport function, and Kt/V were examined.
Results: 452 CAPD patients with 15 months of median PD duration (mean age 48±15.6 years; 245 men, 207 women) were analyzed. The basic nephropathy included glomerulonephritis (59.3%), diabetic nephropathy (21.2%), renal vascular disease (8%), and other renal diseases (12.2%). Average serum phosphorus level was 1.63±0.48 mmol/L, which was correlated with significantly positive correlations between serum phosphorus level and the PD duration, nitrogen (BUN), creatinine (Cr), pre-albumin, nPCR (r=0.264, 0.952, 0.639, 0.602, 0.265, 0.049, p<0.05). The negative correlations between serum phosphorus level and Kt/V, creatinine clearance (CrCl), hemoglobin, hematocrit, dialysate-to-plasma creatinine (D/PCr), residual renal function (r=–0.3, –0.426, –0.169, –0.18, – 0.237, – 0.219, p<0.05) were found.
Conclusions: Optimal serum phosphorus level depends not only on dialysis but also on dietary restriction. Excess protein intake and the longer PD duration might predict the increased serum phosphorus level. RRF was the important limitation of PD patients alone to achieve adequate phosphorus control.
Cao P., Wei J.L., Yi C.Y., Lin J.X., Zhang X.D., Yang X., Guo Q.Y.,
A Pregnant Patient with Chronic Allograft Nephropathy on CAPD
Objective: Infertility is a frequent finding in patients affected with chronic kidney diseases. Moreover, since abnormalities in menstruation are also common in this patient group, pregnancy is usually diagnosed with noticeable delay. On the other hand, β–HCG typically increases in chronic kidney disease patients; therefore, making it of lower diagnostic value in a suspected pregnancy. The definitive diagnosis of pregnancy in these patients is only made based on ultrasonographic detection of pregnancy sac. The prevalence of amenorrhea and non-ovulatory cycles increases in women with serum creatinine levels >3 mg/dL resulting in decreased possibility of pregnancy and reaching the term pregnancy age to a rather low extent. Moreover, prematurity in pregnancy is more prevalent in patients with serum creatinine levels >1.4 mg/dL. Meanwhile, the risk for premature births, spontaneous abortion, IUGR births is present in about 1/3 to 2/3 of these patients. Considering the catabolic status of the body in pregnant women, PD can improve the hypertension and metabolic consequences resulting from kidney failure. Our objective in the present case was to assist the patient to fulfill her pregnancy under PD treatment for her renal failure. Methods: The patient is a 32-year-old woman suffering from chronic renal failure due to unknown etiology who has been treated by hemodialysis since 9 years ago. She had also received a kidney transplant 6 years ago. Results: The golden baby was delivered through Cesarean section at week 36 of the pregnancy due to premature rupture of membrane. She was a baby girl weighing 2.6 kg. 2 months after delivery, the peritoneal catheter was removed and the patient lived without dialysis. Conclusions: Taking into account the better control of hypertension and fluid volume in peritoneal dialysis, peritoneal dialysis seems to be a better modality for controlling pregnant women suffering from chronic renal failure.