
Abstract
Oral Paricalcitol Effects from Hyperparathiroidism Treatment to Renoprotection
Background: The new understanding of vitamin D endocrine/intracrine system alters the view of renal disease and its treatment. VitD analogs are expanding because of its role on inflammation, fibrosis related to reninangiotensin-aldosterone axis (RAAS) with a renoprotective effect. The aim of this study is to assess the effect of oral paricalcitol on PTH and proteinuria in CKD stage 3–5ND patients on 6 months of follow-up.
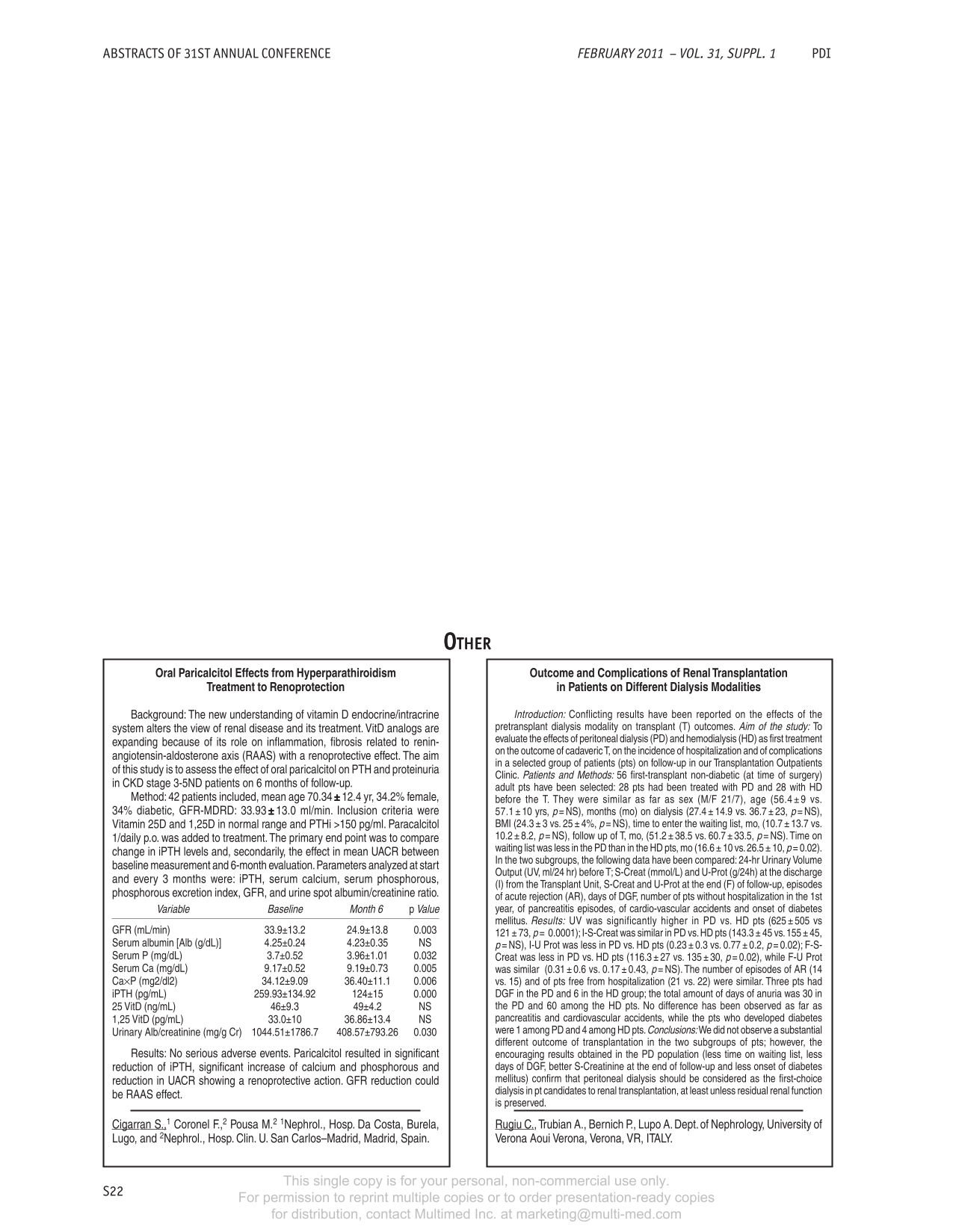
Method: 42 patients included, mean age 70.34 ± 12.4 yr, 34.2% female, 34% diabetic, GFR-MDRD: 33.93 ± 13.0 ml/min. Inclusion criteria were Vitamin 25D and 1,25D in normal range and PTHi >150 pg/ml. Paracalcitol 1/daily p.o. was added to treatment. The primary end point was to compare change in iPTH levels and, secondarily, the effect in mean UACR between baseline measurement and 6-month evaluation. Parameters analyzed at start and every 3 months were: iPTH, serum calcium, serum phosphorous, phosphorous excretion index, GFR, and urine spot albumin/creatinine ratio.
Results: No serious adverse events. Paricalcitol resulted in significant reduction of iPTH, significant increase of calcium and phosphorous and reduction in UACR showing a renoprotective action. GFR reduction could be RAAS effect.
Cigarran S.,1, Coronel F.,2, Pousa M.2, 1Nephrol., Hosp. Da Costa, Burela, Lugo, 2Nephrol., Hosp. Clin. U. San Carlos–Madrid, Madrid, Spain.
Outcome and Complications of Renal Transplantation in Patients on Different Dialysis Modalities
Introduction: Conflicting results have been reported on the effects of the pretransplant dialysis modality on transplant (T) outcomes. Aim of the study: To evaluate the effects of peritoneal dialysis (PD) and hemodialysis (HD) as first treatment on the outcome of cadaveric T, on the incidence of hospitalization and of complications in a selected group of patients (pts) on follow-up in our Transplantation Outpatients Clinic. Patients and Methods: 56 first-transplant non-diabetic (at time of surgery) adult pts have been selected: 28 pts had been treated with PD and 28 with HD before the T. They were similar as far as sex (M/F 21/7), age (56.4± 9 vs. 57.1 ± 10 yrs, p= NS), months (mo) on dialysis (27.4 ± 14.9 vs. 36.7 ± 23, p= NS), BMI (24.3 ± 3 vs. 25 ± 4%, p= NS), time to enter the waiting list, mo, (10.7 ± 13.7 vs. 10.1 ± 8.2, p= NS), follow up of T, mo, (51.2 ± 38.5 vs. 60.7 ± 33.5, p= NS). Time on waiting list was less in the PD than in the HD pts, mo (16.6 ± 10 vs. 26.5 ± 10, p= 0.02). In the two subgroups, the following data have been compared: 24-hr Urinary Volume Output (UV, ml/24 hr) before T; S-Creat (mmol/L) and U-Prot (g/24h) at the discharge (I) from the Transplant Unit, S-Creat and U-Prot at the end (F) of follow-up, episodes of acute rejection (AR), days of DGF, number of pts without hospitalization in the 1st year, of pancreatitis episodes, of cardio-vascular accidents and onset of diabetes mellitus. Results: UV was significantly higher in PD vs. HD pts (625 ± 505 vs 121 ± 73, p= 0.0001); I-S-Creat was similar in PD vs. HD pts (143.3 ± 45 vs. 155 ± 45, p= NS), I-U Prot was less in PD vs. HD pts (0.23 ± 0.3 vs. 0.77 ± 0.2, p= 0.02); F-S-Creat was less in PD vs. HD pts (116.3 ± 27 vs. 135 ± 30, p= 0.02), while F-U Prot was similar (0.31 ± 0.6 vs. 0.17 ± 0.43, p= NS). The number of episodes of AR (14 vs. 15) and of pts free from hospitalization (21 vs. 22) were similar. Three pts had DGF in the PD and 6 in the HD group; the total amount of days of anuria was 30 in the PD and 60 among the HD pts. No difference has been observed as far as pancreatitis and cardiovascular accidents, while the pts who developed diabetes were 1 among PD and 4 among HD pts. Conclusions: We did not observe a substantial different outcome of transplantation in the two subgroups of pts; however, the encouraging results obtained in the PD population (less time on waiting list, less days of DGF, better S-Creatinine at the end of follow-up and less onset of diabetes mellitus) confirm that peritoneal dialysis should be considered as the first-choice dialysis in pt candidates to renal transplantation, at least unless residual renal function is preserved.
Rugiu C., Trubian A., Bernich P., Lupo A., Dept. of Nephrology, University of Verona Aoui Verona, Verona, VR, ITALY.
How Renal Transplantation Induces Bias in Peritoneal Dialysis Survival Analysis
Background: Survival analyses on dialysis usually do not exclude patients for whom renal transplantation (RT) is planned. Some patients may have RT before death during PD is observed. This can lead to biased estimations in the total population.
Patients and Methods: (i) We first analyzed a cohort of 293 patients starting PD between 1992 and 2007 in a single center. (ii) We then verified our analysis on a cohort of 6610 PD patients from the ‘Registre de Dialyse Péritonéale de Langue Française’ (RDPLF). We estimated cumulative incidences for death and RT according to whether RT was planned or not. We explored risk factors for death and RT using the Cox proportional hazard model.
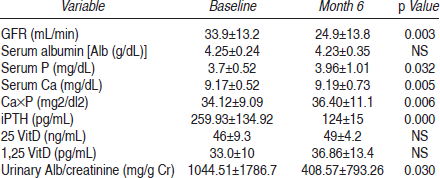
Results: (i) RT was planned for 114 (39%) patients, none of whom died. At 6 years, their estimated probability of RT was 72%. They were younger and had fewer comorbidities. In the total population, older age, diabetes, low albumin, and low residual renal function were significant risk factors for death and significant contra-indication factors for RT. Therefore, the death hazard ratio could not be estimated independently of RT. (ii) The RDPLF data confirmed these results. RT was planned for 2205 (33%) patients. Their probability of death was estimated at 5% at four 4, against 57% for the 4422 (67%) other patients. Age and diabetes were inversely related to death and RT.
Conclusion: Patients for whom RT is planned are much more likely to undergo renal transplantation than to die on PD. This competition between death and RT means that relative risks for death cannot be estimated independently of RT in the total population. This selection bias should be taken into account in PD survival analyzes.
Beuscart J-B.,1,2, Pagniez D.,1, Frimat L.,3, Evans D.,4, Lessore C.,1, Boulanger E.,1, Verger C.,4, Duhamel A.2, Nephrology Department,1 Huriez Hospital, Lille, France, Biostatistics Department,2 EA 2694, Lille, France, Nephrology Department,3 EA 4003, Nancy, France, Peritoneal Dialysis Registry (RDPLF),4 Pontoise, France.
Fluid Flow Stress Affects Peritoneal Cell Kinetics: Possible Pathogenesis of Peritoneal Fibrosis
Object: During PD, the dialysis solution streaming continuously generates fluid flow stress to the peritoneum under peristalsis and body motion. Fluid flow stress has been implicated as playing a critical role in the physiological responses of many cell types. Thus, we hypothesized that the fluid flow stress may affect peritoneal cell kinetics. Our study aims to clarify whether the flow stress is involved in the pathogenesis of peritoneal fibrosis.
Methods: To generate fluid flow stress, the culture container is placed on a rotatory shaker in a thermostatic chamber. In this system, the shaker rotates at a speed of 25 rpm with a radius of 1.5 cm. Mesothelial cells, either with or without the flow stress, were cultured in complete medium consisting of low-glucose (1000 mg/L) or high-glucose (4500 mg/L).
Results: The fluid flow stress promoted hyperplasia and epithelialmesenchymal transition (EMT) of mesothelial cells in a glucose concentration-independent way. Fluid flow stress inhibited the ERK- and p38-MAPK expression in mesothelial cells. Administration of ERK- and p38-MAPK inhibitors replicated the stress-induced morphology of mesothelial cells.
Conclusion: The data indicates that the fluid flow stress promotes hyperplasia and EMT of mesothelial cells via the MAPK axis, suggesting that fluid flow stress may be involved in the pathogenesis of peritoneal fibrosis.

Aoki S.,1, Makino J.,2, Yamasaki F.,1, Noguchi M.,3, Toda S.1, Department of Pathology,1 Saga University, Saga, Japan, Department of Urology,2 Makino Clinic, Saga, Japan, Department of Urology,3 Saga University, Saga, Japan.
Biocompatibility of Normal Saline During its Intraperitoneal Dwell
Background: Normal saline (0.9% NaCl) is commonly used for rinsing the abdominal cavity, and many surgeons claim that it is not harmful to peritoneum because it is instantly drained. However, significant volume of the instilled solution (up to 25% – our observations in patients undergoing laparoscopic surgery) is not drained and dwells in the peritoneal cavity until it is fully absorbed. We evaluated changes of normal saline properties and biocompatibility during its dwell in the rat's abdominal cavity.
Method: In 10 anesthetized rats, normal saline (30 mL) was instilled into the abdominal cavity and samples of the dwelling solution were collected every 30 min, for 4 hrs. Composition of normal saline, inflammatory parameters and effect of the collected samples on in vitro cultured rats’ mesothelial cells were studied. Low pH of normal saline was normalized after 3 hrs. After 4 hrs, number of cells in fluid was increased (+120%, p< 0.001) as well as % of eosinophils (+41%, p< 0.05). Activity of elastase was increased (+133%, p< 0.001), as well as conc. of MCP-1 (+208%, p< 0.001) and TGF-β (+239%, p< 0.01). Fluid samples tested ex-vivo suppressed proliferation of mesothelial cells, and the effect was proportional to the dwell time (-49%, p< 0.001, at 4 hrs) and induced transient stimulation of MCP-1 synthesis in these cells (+96%, p< 0.001 after 60 min), but fluid samples obtained after 4 hrs had similar suppressive effect on MCP-1 release as normal saline.
Conclusion: We conclude that during intraperitoneal dwell, chemical composition of normal saline gradually normalizes. However, biocompatibility of normal saline decreases during its dwell in the abdominal cavity as reflected by enhanced inflammatory response and cytotoxicity towards mesothelial cells. Our results suggest that normal saline should not be used for rinsing peritoneal cavity.
Cwalinski J.,1, Polubinska A.,2, Breborowicz A.,1, Oreopoulos D.2, Poznan University of Medical Sciences,1 Poznan, Poland, University of Toronto,2 Toronto, Canada.
Maintaining PD Patients’ Estimated Dry Weights Using Only 1.5% Dextrose Concentrations of Delflex PD Solution
Purpose: To determine if it is possible to maintain adequate fluid removal using strictly 1.5% Delflex PD solutions, and also help to decrease weight gain by receiving fewer calories through the use of the lowest dextrose concentration available.
Method: Beginning in 2010, we had approximately 20 patients using only 1.5% dextrose and found that patients were able to maintain their estimated dry weights very well. Whenever more fluid removal was needed, an additional exchange using another 1.5% solution was instilled and allowed to dwell for only 30 minutes. Using this sodium sieving principle generally resulted in an ultrafiltration of approximately 100ml – 500ml per exchange. This was performed PRN.
Results: It was found that 1.5% solutions together with short 30 minute dwells did allow sufficient fluid removal. Rarely were any 2.5% required and the use of 4.25% solutions was completely eliminated. Eighty percent of the patients have shown a decrease in their estimated dry weights, with 15% remaining the same.
Conclusion: After eight months of using this principle of fluid removal, patients demonstrated stable weights while tremendously decreasing their exposure to high concentrations of dextrose and calories.
Lavergne L., Fresenius Medical Care, New Iberia, LA, U.S.A.
If There's a Will, There's a Way!
Purpose: To design a photographical system that will assist our illiterate patients to perform efficient inventory and ordering of PD supplies.
Methods: Staff made a list of all patient supplies and created photographic images of each item patients used for their treatments. Photos were laminated and secured in a binder for easy patient access and reference. Each photo was labeled with a designated number that a patient can refer to when ordering with Customer Service. The staff and FMCNA Customer Service representative coordinated and collaboratively worked to enable the patient to perform the task by using this photographical system. The same photo images were attached via e-mail to Customer Service. When a patient places an order, any of the Customer Service representatives can refer to those images and accurately fill the order.
Results: Patients are able to independently perform inventory and ordering of PD supplies with ease and confidence when using a system such as this.
Conclusion: A stumbling block in a patient's ability to perform a task due to illiteracy no longer stops patients from being able to be on home PD therapy. Our staff's creative design of a system, together with the strong willingness of the FMCNA Customer Service representatives to team up, gives illiterate patients the independence and confidence to overcome these obstacles.
Delgado E., Fresenius Medical Services, Flemington, New Jersey, U.S.A.
Economic Analysis of the Impact of Local Manufacturing of Peritoneal Dialysis Fluid on Renal Replacement Therapy in a Developing Country
Peritoneal dialysis (PD) is being practiced in India for more than two decades and is now an established treatment modality for end stage renal disease. In the first decade, due to the need of importing of the PD fluids, the cost of PD was about twice that for hemodialysis (HD). Local manufacturing of PD fluids has reduced the cost of PD drastically, though most health professionals still have a perception that it is more expensive than HD. PD is therefore offered only to the more affluent patients, resulting in low utilization of this therapy. What has not being considered in this ‘comparison’ of the two modalities is the ‘hidden’ costs on HD that, in the ultimate analysis, could make PD the more cost-effective RRT. To our knowledge, no such study has been undertaken in our country and such a study would help implement health care policies in a cost-effective manner.
Global Hospitals is a tertiary care hospital in the City of Hyderabad, South India and has an active nephrology comprehensive care facility. Patients with ESRD who began RRT between October 1, 2008 and December 31, 2008 were considered for inclusion in the study. Patients undergoing APD were excluded, as it is not a common therapy in our Center. Patients were designated as PD or HD patients based on first noted treatment. Patients with less than 6 months of pretreatment data and those with less than 12 months of data following initiation of dialysis were dropped from the study sample. The PD patients were matched to HD patients using propensity scoring to control for differences in pretreatment attributes. Health care costs were then compared over 12 months between propensity-matched PD and HD patients using paired t-tests, depending on patient chart review, expense account, dairies, bill payments (cash or check) and a reliable history.
Various ‘hidden’ costs associated with treatments like the time lost in terms of ‘man hours’ due to the therapy and that of attendants (if applicable) were also analyzed by assigning a financial numerical value. A comparative cost analysis was done using paired t-tests. A total of 10 HD patients and 10 CAPD patients were eligible for the analysis. HD median healthcare costs over the 12-month follow-up period were US$4687 higher (US$12,465 vs. US$7778 for PD patients, p< 0.002) with 95% confidence interval being from US$2589 to US$6784 per year. The mean cost of treating complications were higher in HD vs. PD – the difference being US$709 (p< 0.04). The mean difference in cost between HD and PD for Erythropoietin treatment was expectedly higher in HD, being US$1455 per year (p< 0.01). The other significant drawback of patients on HD was a 42% reduction of personal income as compared to PD after the inception of local manufacturing of PD solutions in India.
PD is now a significantly more cost-effective therapy to maintain patients with ESRD on RRT. Due to limited health-care budgets, lack of HD facilities and better rehabilitation of patients on PD, it should be the therapy of ‘first choice’ in countries like India with facilities for local manufacturing.
Nayak A.,1, Antony S.2, Birla Institute of Technology and Science,1 Pilani, Rajasthan, India, Global Hospital,2 Hyderabad, Andhra Pradesh, India.
A Systemic Analysis of Gene Expressions with DNA Microarray and Metabolic Productions with Time-of-flight Mass Spectrometry in a Rat Model for Peritoneal Dialysis – a Mechanism of Peritoneal Injury
Objective: Chronic peritoneal dialysis causes the peritoneum to induce peritoneal hyperpermeability, and patients were forced to give up peritoneal dialysis. Glucose degradation products (GDPs), included in peritoneal dialysis fluids (PDFs), are probably one of the primary cause for peritoneal injuries. We examined clearing the mechanism of peritoneal injury by GDPs with transcriptome and metabolome analysis.
Methods: Rats (male, 6 weeks of age) were administered intraperitoneally 0 to 20 mM methylglyoxal (MGO) / PDFs for 21 days (100 ml/kg). Peritoneal permeability was analyzed by peritoneal equilibration test, and the thickness and fibrosis of the peritoneum was determined by haematoxylin-eosin and azan stain. Gene expressions of peritoneum were assessed using DNA microarray (approximately 24,000 genes). Metabolomics in PDFs was analyzed by CE-TOFMS.
Results: MGO-administered rats had an increase in peritoneal permeability, and in the thickness and fibrosis of the peritoneal membrane. In the surface of the peritoneum, mesenchymal-like mesothelial cells over-proliferated. DNA microarray analysis revealed that 35 genes increased more than 8 times, and 168 genes increased more than 4 times, especially extracellular matrix (such as type III, IV collagen, etc.), and antioxidant enzymes (such as glutathione peroxidase, glutathione synthetase, etc.) increased. CE-TOFMS analysis revealed that antioxidant materials (such as taurine, glutathione, etc.) increased.
Conclusions: Intraperitoneal GDPs increased antioxidant materials, and induced mesothelial cell to redifferentiate and proliferate, resulting in peritoneal fibrosis and remodeling. It was suggested that GDPs, which generated oxidative stress, injured the peritoneum and induced the hyperpermeability of peritoneum.
Imai T., Hirahara I., Morishita Y., Inoue M., Muto S., Kusano E., Jichi Medical University, Shimotsuke-shi, Tochigi-ken, Japan.
Use of Process Mapping to Improve the Pre-dialysis Patient Pathway
Background: The pathway of chronic kidney disease (CKD) patients towards dialysis can be complex. If the pathway is not well planned, patients may not receive appropriate information and may not be well prepared for dialysis. As a result, they may commence dialysis without making an informed modality choice and with no permanent dialysis access. Understanding the patient pathway enables appropriate pre-dialysis patient management to be planned.
Objective: This project was undertaken in two countries within our dialysis clinic network. It applied process mapping to investigate the patient pathway to dialysis. The aims of the study were: to identify potential areas for improvement in pre-dialysis patient management and to give more patients an informed choice of dialysis modality.
Method: A multidisciplinary workshop was held with clinical teams from dialysis clinics in both countries. Training was given in process mapping using methodology that has been employed across the UK National Health Service. Each clinical team was guided to produce a detailed process map of the patient pathway in their clinic. The scope was determined carefully and examined from outpatient referral to the first day of starting dialysis with a permanent access. Each clinic's process map was presented to the group and examined to identify areas of good practice and also areas where improvement was required. The maps were then combined into a common process mapped pathway which was reviewed by all of the clinical teams. After generation of the combined process map, there was discussion regarding potential changes in the CKD patient pathway.
Results: The teams were able to produce low-level process maps which defined the detailed patient pathway to dialysis in their clinics. They described the roles and responsibilities of the multidisciplinary team, and outlined clear steps in the process. Certain steps in the process map were examples of good clinical practice and some were identified as needing improvement. Functional bottlenecks in the pre-dialysis clinics were identified which meant that, in a busy clinic, it was difficult to ensure focused pre-dialysis management. Some steps were identified which potentially did not add value to the patient pathway.
Conclusions: Care of the patient as dialysis approaches is complex and involves many professionals working in a coordinated manner. Process mapping of the pre-dialysis pathway has enabled good practice to be shared and barriers to coordinated care to be identified. The final maps produced in both countries were very similar and identified the need for additional resources. They also identified where pre-dialysis clinics could be rearranged to better manage patients’ pre-dialysis experience.
Cowperthwaite J.,1, Rutherford P.,2, Hegbrant J.1, Diaverum Renal Serivces Group,1 Lund, Sweden, Baxter Healthcare SA,2 Zurich, Switzerland.
Longitudinal Analysis of Fluid Transport and its Determinants in PD Patients who Develop Encapsulating Peritoneal Sclerosis
Background: Encapsulating peritoneal sclerosis (EPS) is a severe complication of long-term peritoneal dialysis (PD). Almost all patients with EPS have severe decreased fluid transport (ultrafiltration failure). Fluid transport is determined by several factors, such as the ultrafiltration coefficient (LpA) and the glucose induced osmotic conductance (GOC). The latter is the product of LpA and the reflection coefficient (sigma). Decreased GOC is an important cause of ultrafiltration failure in long-term PD patients. It remains unclear whether a decreased GOC causes ultrafiltration failure in patients who develop EPS. The aim of this study was to longitudinally analyze the determinants of fluid transport during the time course of the development of EPS.
Methods: Twelve PD patients who developed EPS were included for this study. The last 4 peritoneal function tests available were analyzed. The peritoneal function was assessed annually with 3.86% glucose dwell/4 hours with the addition of a volume marker. Sigma was estimated from pore size modeling and LpA from Starlings equation. The determinants of fluid transport were analyzed with a linear mixed model test.
Results: During the last 4 years prior to EPS, the net ultrafiltration showed a linear decrease. This trend was determined by both a decrease in LpA and a decrease in GOC. Sigma showed an initial decrease; however, a slight increase was present in the last year prior to the diagnosis of EPS.
Conclusion: A decrease of fluid transport prior to the development of EPS was present. The increase of sigma one year prior to EPS may be due to thickening of the interstitium or interstitial fibrosis. A follow-up study should compare these results with long-term PD patients with ultrafiltration failure.
Sampimon D., Coester A., Struijk D., Krediet R., Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands.
The Seasons of Dialysis: In-center versus Home Therapy
It has been hypothesized that patients who dialyze in a home based environment appear to thrive better than the patients who dialyze in an in-center limited care facility. This premise raises the question of why our In-center Limited Care Facility (ILCF) is so large and our Home Therapy (HT) programs are so small. We conducted a small study to access the reasons why the majority of our patients are dialyzing in ILTC. Following the questioning of patients from various in-center facilities, reasons cited for dialyzing are as follows: 1) No other options were available at the time of dialysis initiation; 2) Patient was emergently placed on dialysis due to procrastination, even if options were offered; 3) Fear of dialysis itself; 4) Lack of education of the benefits of H T.
Due to the growing demand for dialysis, we further researched this issue with the patients who were offered Treatment Options (TOPS) and discovered that 76% of all the patients that were offered TOPS chose a home-based therapy. We again questioned the validity of our study due to the size of our ILCF and came to this conclusion. Although home patients appear to have a better quality of life and more active lifestyle than our in-center patients, the best type of dialysis is the treatment that best fits the patient.
We have summed our conclusion with this acronym: Season
Support—Always support the pt in adjusting to whichever TOP they choose.
Educate—Educate the pt, not the group. Focus teaching on the individual and the process.
Aspire—Aspire to deliver all the knowledge, compassion, and empathy possible.
Seek—Seek to be the best health care provider possible by imparting compassion, love, and empathy.
Ongoing—Know that dialysis is a dynamic, ongoing process that requires heart and a positive attitude. Continually encourage the pt.
Never—Never forget that the only thing separating you from dialysis is God's grace and mercy.
Spiritual guidance—Know that there will be days when it will require seeking a higher power to make a difference in a pt's life.
Adams R., Brookhaven Home Therapy, Brookhaven, MS, U.S.A.
What Is Good About PD+HD Combined Therapy
Objectives: It is known that β2-microglobulin (β2-MG) concentration in peritoneal dialysis (PD) patients is inversely correlated to the residual renal function (RRF). With decreasing RRF, some PD patients may necessarily be treated with hemodialysis (HD) once a week, not only for removing excess water and small solutes but also for removing much larger solutes such as β2-MG. In this study, a kinetic model allowed us to show what is good about PD+HD combined therapy in long-term PD patients.
Methods: A mathematical model was established, based on a classic compartment theory for clinical use. Model validations were made by comparing calculated results with clinical data in order to specify what was good about PD+HD combined therapy (5-day PD + 1-HD/wk).
Results and Discussion: Time-averaged concentration (TAC) for creatinine decreased by 10% on average by introducing PD+HD combined therapy regardless of which dialyzers were used. TAC for β2-MG in PD+HD combined therapy, however, was strongly dependent upon the dialyzer clearance. Therefore when low or middle flux dialyzers (clearance for β2-MG < 20 mL/min under QB = 200, QD = 500 mL/min) were used, β2-MG concentration may increase from 20 to 30 mg/L. Use of super high-flux dialyzers (clearance for β2-MG > 60 mL/min under the same conditions) should keep the β2-MG concentration stable at around 20 mg/L. When PD+HD combined therapy is introduced to a PD patient with diminishing RRF, use of super high-flux dialyzers may be necessary in order not to increase concentrations of β2-MG and/or even greater solutes.
Conclusions: Using super high-flux dialyzers may prevent concentrations of large solutes from increasing, a key to the success of PD+HD combined therapy.
Yamashita A., Tomisawa N., Shonan Institute of Technology, Fujisawa, Kanagawa, Japan.
Bioimpedance Spectroscopy for the Detection of Hypervolemia in Peritoneal Dialysis Patients
Introduction: A practical, inexpensive and reliable method is needed for assessment of volume status in peritoneal dialysis (PD) patients. In this study, the efficiency of bioimpedance spectroscopy (BIS) for detection of hypervolemia was investigated.
Method: From a center, 79 prevalent PD patients were enrolled. Echocardiography and body composition analysis using BIS technique (50 frequencies) (Body Composition Monitor) were performed. Overhydration (OH) and extracellular water (ECW) in liters and OH/ECW ratio were used as volume indices.
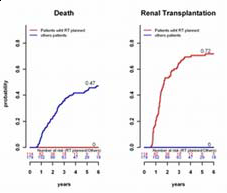
Results: Mean age was 47±14 years, PD duration was 30±17 months; of cases 55% were male, 19% were diabetic. Mean left ventricular mass index (LVMi) was 117 ± 37 gr/m2 and 46% of patients had left ventricular hypertrophy (LVH). Mean OH and OH/ECW ratio were 1.3 ± 1.7 L and 7.6±9.3%, respectively. OH/ECW ratio was correlated with LVMi (r:0.237, p< 0.036) and left atrium index (LAi) (r:0.354, p< 0.001). Patients with LV H had higher OH values than patients without LV H (1.79±1.82 L and 0.93 ± 1.62 L, p= 0.003) (Table). In linear regression analysis, OH/ECW ratio was an independent risk factor for LV H (t:2.558, p:0.01).
LVH = left ventricular hypertrophy; TBW = total body water; BP = blood pressure.
Conclusion: BIS is a reliable method to evaluate volume status in PD patients. OH/ ECW measured by BIS is a major determinant of left ventricular mass. Control of hypervolemia and blood pressure is associated with better cardiac condition.
Hur E.,1, Musayev O.,2, Usta M.,3, Gungor O.,1, Toz H.,1, Asci G.,1, Ozkahya M.,1, Ok E.1,4, Nephrology Department,1 Ege University Medical School, Izmir, Turkey, Cardiology Department,2 Ege University Medical School, Izmir, Turkey, Bursa State Hospital,3 Bursa, Turkey, Fresenius Medical Care,4 Izmir, Turkey.
Reduction in the Annual Cost of a Dialysis Patient As Peritoneal Dialysis Utilization Increases
Background: Dialysis therapy, which is driven by in-center hemodialysis (ICHD) is expensive. Dialysis patient populations in many regions may outgrow the availability of staff to provide care in the near future. Home dialysis is less expensive than ICHD and requires fewer staff resources. We investigated the association between greater use of home dialysis and the annualized per-patient cost of dialysis among states.
Method: Using 2008 data by state, we calculated from Medicare's perspective the percent of prevalent dialysis patients using PD and the annual cost of a dialysis patient (the weighted average of all dialysis modalities) from the USRDS's 2010 Annual Report. Total costs for dialysis included inpatient, outpatient, physician supplier, skilled nursing facility, home health agency, and hospice. We grouped states into three categories based on the percent of dialysis patients using PD: G1 (< 6%); G2 (≥ 6 and < 9%); G3 (≥ 9%). The mean annual cost of a dialysis patient for each state was adjusted by that state's health care cost of living index. Group means were then calculated by weighting by the number of dialysis patients in each state. Tukey's multiple comparison test was used to evaluate differences in the mean annual costs between groups. A p-value < 0.05 was considered significant.
Results: The adjusted means for the three categories were G1: $81,736 (n = 12); G2: $74,088 (n = 28); and G3: $70,459 (n = 11). G1 was significantly higher than either G2 or G3. There was no difference between G2 and G3. A weighted linear regression (where the dependent variable was the state's mean annual cost for a dialysis patient and the independent variable was the percent of dialysis patients on PD in the state) found that, for every 1% increase in patients on PD, the mean annual cost per dialysis patient dropped by nearly $1,800.
Conclusion: There was a strong association at the state level that states with greater use of home PD had lower annual total dialysis costs per patient.
Walker D., Just P., Inglese G., Baxter Healthcare Corporation, McGaw Park, IL, U.S.A.
Hyperglycemia and Mortality in Chronic Peritoneal Dialysis Patients with Diabetes Mellitus
Background: It is not clear whether hyperglycemia has a bearing on mortality in diabetic dialysis patients. In chronic peritoneal dialysis (CPD) patients, the association may be confounded by glucose loading in PD fluid.
Methods: We examined a large and contemporary cohort of all diabetic CPD patients who underwent peritoneal dialysis treatment by Day 90 in any DaVita dialysis clinic from July 2001 through June 2006 and who were followed up to June 2007.
Results: We identified 2798 diabetic CPD patients with A1c measurements (58±12.8 yrs old, 44% women, 20% African Americans, 16% Hispanics). Random serum glucose that was measured in DaVita Laboratories (Deland, FL), was then categorized into 6 a priori selected groups of <100, 100<150 (ref), 150<200, 200<250, 250<300 and ≥300 mg/dL. Glucose ≥300 mg/dL had a 6-yr death HR (95% confidence interval) of 1.22 (1.04–1.52) after adjusting for case-mix (gender, age, race, ethnicity, vintage, insurance, comorbid conditions, smoking, residual renal function, Kt/V) and measures of malnutrition-inflammation-cachexia syndrome (MICS) (BMI, serum albumin, ferritin, creatinine, phos, calcium, bicarbonate, TIBC, WBC, lymphocyte%, hemoglobin) (see Fig.).
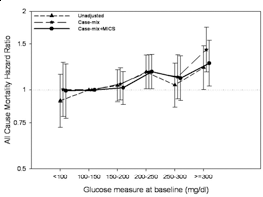
Conclusions: In this large national cohort of diabetic CPD patients, marked hyperglycemia ≥300 mg/dL appears associated with 22% increased mortality compared to 100 to 150 mg/dL range. Clinical trials to examine the benefit of glycemic control are indicated.
Molnar M.Z.,1, Mehrotra R.,1, Duong U.,1, Lukowski L.R.,1, Moran J.,2, Kovesdy C.P.,3, Kalantar-Zadeh K.1, LABioMed at Harbor-UCLA,1 Torrance, CA USA, DaVita,2 Lakewood, CO, USA, Salem VA,3 Salem, VA USA.
Regeneration of Mesothelial Cell in the Damaged Peritoneum by Tissue-engineered Mesothelial Cell Sheet
Background: Peritoneal fibrosis with denuded of mesothelial cells resulting from peritoneal sclerosis is one of the most serious complications in peritoneal dialysis (PD) patients. Regenerative therapies using the cell sheet engineering techniques have been examined to repair the damaged peritoneum. We already have developed the human mesothelial cell sheets. In this study, we have evaluated transplantation of human mesothelial cell sheets using a mice model with the damaged peritoneum.
Method: Human mesothelial cell sheets were made using temperature-responsive surfaces. To establish the model, a daily intraperitoneal injection of 0.1% chlorhexidine gluconate was given to male nude mice for 7 days. Human mesothelial cell sheets using temperature-responsive surfaces were transplanted onto mice parietal peritoneum without support. Thereafter, pathological changes to the peritoneal membrane were observed, and the existence of cell sheet was examined.
Results: In the model, microscopic examination revealed a progressive thickening of the submesothelial layer. The cell sheets remained on parietal peritoneum for a week after the transplantation. Thickening of the submesothelial layer was decreased by the cell sheets. The sheets were observed to cover the host tissue at one week and stay as mesothelial lining on the parietal peritoneum.
Conclusion: These results indicate that the developed human mesothelial cell sheets can be applied for repairing damaged peritoneum.
Sakiyama R.,1,2, Sekine H.,2, Honda K.,3, Akiyama Y.,2, Yamato M.,2, Okano T.,2, Mineshima M.1,2, Department of Clinical Engineering,1 Tokyo Women's Medical University, Shinjyuku-ku, Tokyo, Japan, Institute of Advanced Biomedical Engineering and Science,2 Tokyo Women's Medical University, Shinjyuku-ku, Tokyo, Japan, Department of Pathology,3 Tokyo Women's Medical University, Shinjyuku-ku, Tokyo, Japan.