
Abstract
Hybrid dialysis involves combining peritoneal and hemodialysis (HD) in patients with end-stage renal disease. Its reported use is quite limited outside of Japan. We present a retrospective review of 18 patients at our center that received this therapy and describe their ultimate disposition. We observed that 39% of the population on hybrid dialysis ultimately transitioned to full in center HD, 28% continue until death, and 33% either transition to home HD or received a transplant. In our center, hybrid dialysis was successful as a bridging therapy or in balancing continuation of dialysis with quality of life among those with a limited prognosis.
Keywords
Hybrid dialysis involves combining peritoneal dialysis (PD) with hemodialysis (HD) to achieve better solute and volume control in a subset of patients with end-stage renal disease. It typically involves adding one or two HD sessions a week to a 5- to 7-day per week PD regimen. It facilitates continuation of PD in certain patients who would otherwise require a complete transition to three times per week HD.
The majority of the published reports on hybrid dialysis come from Japan. 1 –3 Only one study, a cross-sectional survey, has been reported in North America, and there is a single study from the United Kingdom. 4,5 In Ontario, Canada, hybrid dialysis is funded through the Ontario Renal Network and patients on home PD can receive one HD treatment per week as part of “dual modality” therapy. To date, there has been no attempt to review the outcomes of patients on hybrid therapy in Ontario. The purpose of this article is to describe the patterns, indications, and outcomes of hybrid dialysis in a single center in Ontario, Canada.
Patients and methods
This is a retrospective study from the Ottawa Hospital, a tertiary care hospital in Ontario, Canada, from the time period between January 2009 and December 2017. The Ottawa Hospital serves a catchment area of approximately one million people and follows approximately 700 patients on in-center HD and 200 patients on home PD.
We primarily sought to perform a descriptive analysis with a focus on the longer term outcomes of patients who are treated with hybrid therapy. Specifically, we were interested to determine if hybrid therapy was acting as a bridge to home hemodialysis (HHD) or kidney transplant, or whether it ultimately resulted in permanent transfer to in-center HD. We followed patients from their first hybrid HD session until they permanently transferred to in-center HD, transferred back to PD, transferred to HHD, were transplanted, or died. The first of these events was recorded as their disposition.
All data were obtained from Nephrocare (Fresenius Medical Care, Bad Homburg Germany) which is an electronic medical record for all dialysis patients at our center. Dialysis modality is tracked in Nephrocare, and patients were identified as hybrid patients if they received HD and PD treatments concurrently.
Data are presented and analyzed in terms of mean and standard deviation.
The study protocol was approved by the Ottawa Hospital Research Ethics Board.
Results
During the period from 2009 to 2017, 694 patients initiated PD and 18 of these patients were ultimately treated with hybrid dialysis. The baseline demographics of this population in comparison to the overall PD population are presented in Table 1. There were no statistically significant differences between the two populations. The mean duration of time on PD was relatively short prior to initiation of hybrid therapy at just 8.5 ± 14.3 months. Nine patients (50%) initiated hybrid due to poor solute clearance, six due to volume overload (33%), and the remaining patients for a combination of both fluid overload and inadequate solute clearance (17%).
Baseline demographics and comorbidities of patients on hybrid dialysis compared with the overall PD population.
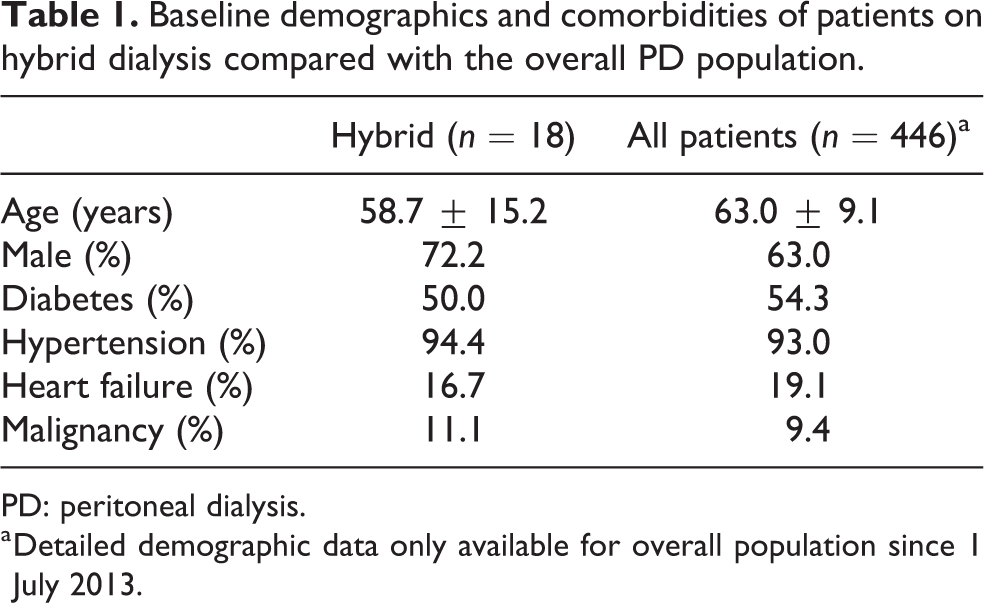
PD: peritoneal dialysis.
a Detailed demographic data only available for overall population since 1 July 2013.
Mean time on hybrid dialysis was 13.9 ± 15.5 months. All patients received between one and three treatments of HD per week in addition to 4–7 days of PD. Five performed continuous ambulatory peritoneal dialysis and the remaining 13 automated peritoneal dialysis. Actual prescriptions varied over the time course of the hybrid therapy. Four patients increased the frequency of their HD sessions over time. Table 2 shows the residual urine volumes at the time of conversion to hybrid therapy as well as the pre-conversion PD prescriptions and hybrid prescriptions at last follow-up.
Hybrid prescriptions.
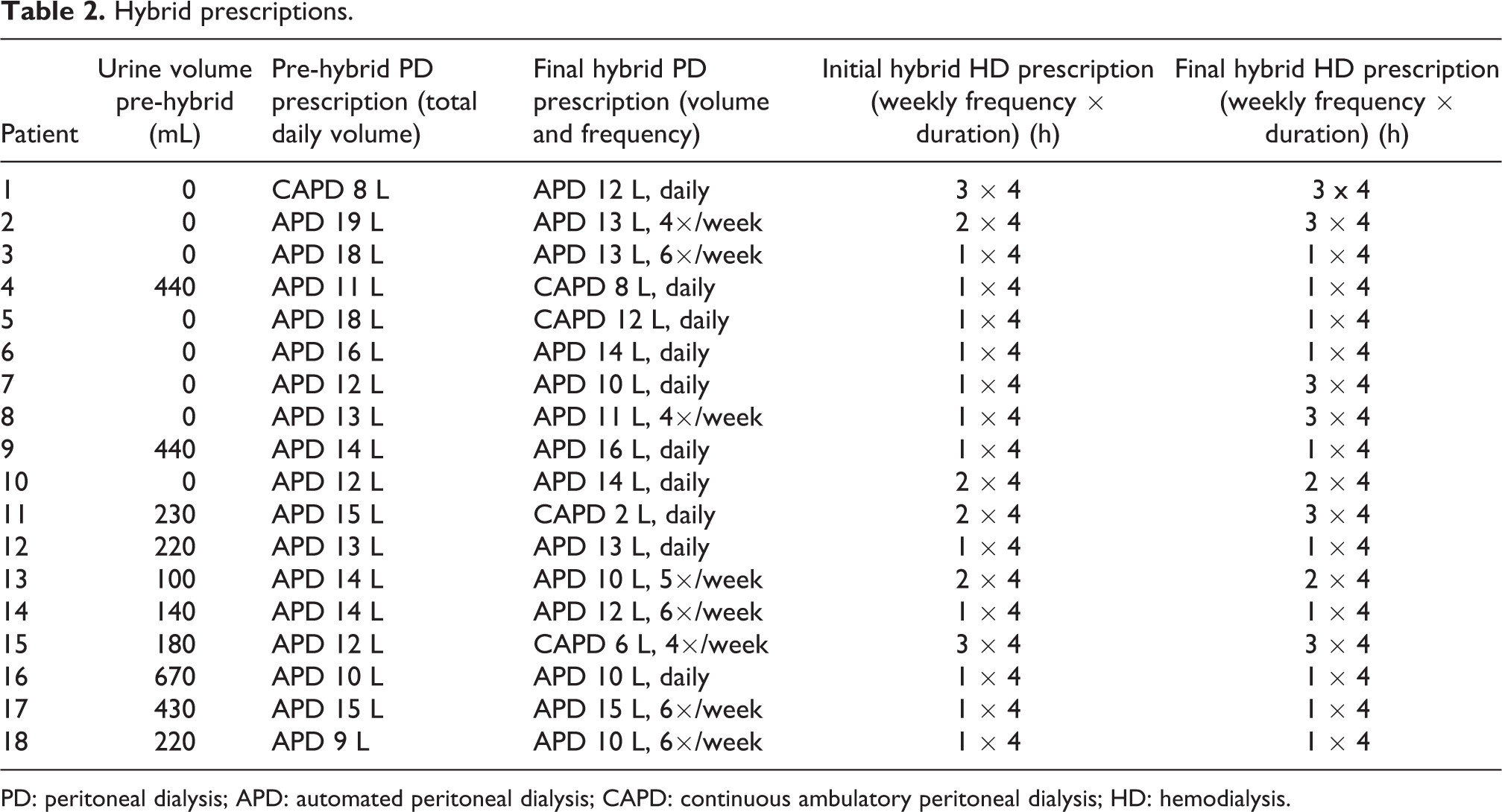
PD: peritoneal dialysis; APD: automated peritoneal dialysis; CAPD: continuous ambulatory peritoneal dialysis; HD: hemodialysis.
There were four episodes of PD peritonitis during the 250 patient-months of follow-up for a rate of one episode for every 62 patient-months. Seventeen of the 18 patients had central lines for HD access at initiation of hybrid dialysis, one had a fistula. There were no episodes of bacteremia.
With respect to disposition, 7 (39%) were permanently transferred to in-center HD after a mean time of 6.1 ± 4.1 months on hybrid therapy. This group had a mean age of 61.0 ± 14.8 years. Hybrid therapy served as a bridge to HHD for 3 (17%) patients with a mean age of 53.3 ± 6.7 years. These patients spent a mean time of 6.7 ± 1.5 months on hybrid. It served as a bridge to transplant for another 3 (17%) patients with a mean age of 44.7 ± 20.1 years who spend a mean of 25.3 ± 27 months on hybrid. Five patients (28%) continued hybrid until they died, and none returned exclusively to PD. The mean age of these patients was 67.2 ± 12.8 years and they stayed on hybrid therapy for significantly longer than those who transferred to full in-center HD (22.4 ± 17.1 vs. 6.1 ± 4.1 months, p = 0.033).
Discussion
Hybrid dialysis therapy occupies an important clinical niche at our center. While only 1–2% of our prevalent PD population receives hybrid therapy at any given time, some patients are able to delay or completely avoid a full transfer to three times per week HD. Our data and experience suggests that there are four distinct populations who may benefit from hybrid therapy.
The first group is those patients who are failing PD and are reluctant to switch to in-center HD for lifestyle reasons. Often these patients can be convinced to do a single HD session per week and then quickly realize that they feel much better on HD and elect to transfer to three times per week HD. Our data suggest that approximately 40% of our hybrid patients may fall into this category and they have a relatively short period of time on hybrid therapy at just 6 months.
Secondly, hybrid therapy is an excellent bridge to HHD for those patients who are interested continuing on a home modality but are unable to transfer directly due to the need for home modifications or delays in access maturity or training. These patients spent an average of 7 months on hybrid before transferring to HHD. Home to home transitions are encouraged in our center. 6
For approximately 17% of our hybrid patients, the dual modality serves as a bridge to transplant. These patients tend to be younger and have issues with inadequate solute clearance and fluid overload. This group of three patients spent between 4 months and 44 months on hybrid therapy prior to transplant.
The fourth group comprises those patients for whom hybrid dialysis serves to maintain a better quality of life during their final period of time on dialysis. We found that almost 30% of patients continued hybrid therapy until their demise. These patients were older and spent on average 22 months on hybrid therapy. There is increasing interest in the role of palliative dialysis and we feel that hybrid therapy may have an important role to play for this subgroup of patients. 7
The potential downsides to hybrid dialysis are important to acknowledge. Two accesses are required, a PD catheter and either a fistula or more often a central venous catheter. Needless to say, this increases the risk for access-related complication. A single run of HD per week significantly adds to the cost of therapy as typically the cost of PD supplies only declines marginally with hybrid therapy. In centers where there are separate PD and HD care teams, there can be confusion at times who is most responsible for the patient. Finally, some argue that hybrid therapy only delays the inevitable switch to three times per week HD and incur costs and risks along the way.
Despite these potential downsides, we feel that hybrid therapy is an underutilized therapy in North America. We have identified four potential PD populations who may benefit from this approach and encourage PD practitioners to consider hybrid therapy when faced with a patient failing PD who is refusing to switch to HD, or as a bridge to HHD or transplant, or a part of an approach to palliative dialysis. We recognize that our single-center descriptive report does not provide high-quality evidence to support our recommendations but feel that prospective studies would be helpful in further understanding what patient populations may benefit from this approach.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.