
Abstract
Background:
The International Society for Peritoneal Dialysis guidelines for small solute clearance and fluid removal in peritoneal dialysis (PD) were published in 2005. The aim of this article is to update those guidelines by reviewing the literature that supported those guidelines and examining publications since then.
Methods:
An extensive search of publications was performed through electronic databases and a hand search through reference lists from the existing guideline and selected articles.
Results:
There have been no prospective intervention trials to inform the area of small solute clearance in PD since the publication of the original guideline in 2005. The trials to date are largely limited to a few prospective cohort studies and retrospective studies. These have, however, consistently demonstrated that residual renal function (RRF) is more often associated with patient outcome than peritoneal clearance. One of the few randomised controlled trials performed in this area does suggest that a weekly Kt/V of 2.27 ± 0.02 provides no statistically significant survival advantage over a weekly Kt/V of 1.80 ± 0.02. The lower limit of Kt/V is unknown but there is weak evidence to suggest that anuric people doing PD should have a weekly Kt/V of at least 1.7.
Conclusions:
There continues to be very poor evidence in the area of small solute clearance and fluid removal in PD. The evidence that exists suggests that RRF is more important than peritoneal clearance and that there appears to be no survival advantage in aiming for a weekly Kt/V >1.70.
Summary statements
Residual renal function (RRF) has been consistently demonstrated to be associated with mortality in people doing peritoneal dialysis (PD) and therefore should be maintained Peritoneal clearance has not been consistently associated with mortality in people doing PD. Total weekly clearances (i.e. the mathematical sum of residual clearance with peritoneal clearance) have never been shown to be based on evidence though the convenience of this measure is recognised There is no evidence that increasing weekly Kt/V >1.7–1.8 provides survival advantage There is evidence that a weekly Kt/V <1.7 is associated with increased morbidity In anuric people doing PD, a weekly Kt/V of at least 1.7 is recommended to prolong survival Ultrafiltration (UF) is associated with overall and technique survival but no numerical target can be recommended Icodextrin is recommended to improve UF independent of the Dialysate/Plasma (D/P) creatinine. There is no apparent risk of adverse side effects or impact on RRF In regions where icodextrin is not easily accessible, a manual daytime exchange may reduce negative UF in people doing continuous cycling peritoneal dialysis (CCPD), particularly high transporters
Recommendations for research
Randomised controlled trial (RCT) investigating an intervention that will preserve RRF and examine if this then translates to improved survival. RCT investigating the effect of incremental PD versus a traditional PD prescription on RRF and peritoneal membrane preservation. Studies to investigate whether the clearance of middle molecules could provide better information to guide adequate dialysis, especially in the light of the limitations of the Kt/V urea. Impact of the increase in the dialysis dose to improve small solute removal and/or UF on quality of life.
Recommendations for audit
Measure RRF at baseline and at least once every 6 months. Measure residual renal clearance and peritoneal clearance at least once every 6 months if a person doing PD appears under-dialysed or if anuric.
Introduction
The 2005 International Society for Peritoneal Dialysis (ISPD) guideline on targets for solute and fluid removal in adults doing chronic peritoneal dialysis (PD) was released at a time where there was a lot of focus on the areas of small solute clearance. 1 It was released soon after some landmark randomised controlled trials (RCTs) were published in this area of small solute clearance and outcomes in people doing haemodialysis and PD. 2 –4 Interestingly, all of these trials concluded that increased small solute clearance above standard practice at the time had no effect on mortality.
Since the guideline was published, there has been a notable paucity of further high-quality evidence to inform the area of small solute clearance and fluid removal. Similarly, there has been an increased awareness that the adequacy of dialysis is far more than just small solute clearance and fluid removal. The aim of this chapter is to review the evidence that supported the 2005 guideline and examine the literature since it was published to see if this can inform an update on these guidelines.
Methods
The literature search for the update of the guidelines was performed using PubMed, maintained at the National Institutes of Health. The search terms used for small solute clearance components of this article included the Medical Subheadings of ‘Peritoneal Dialysis’ OR ‘Peritoneal Dialysis, Continuous Ambulatory’ AND the keywords ‘Clearance’ OR ‘Adequacy’. The search was limited to clinical trial, clinical trial phase I–IV, comparative study, controlled clinical trial, meta-analysis, observational study, pragmatic clinical trial and limited to 1 January 2005 onward. The reference lists from the original guideline and selected articles were also reviewed for any other relevant studies. Finally, although carefully performed, this is a narrative rather than a systematic review.
For the part related to ultrafiltration (UF), we used the terms ‘ultrafiltration’ AND ‘Peritoneal dialysis’ AND ‘survival’ AND ‘mortality’. We retrieved 167 papers published after January 2005, when the first version of this guideline was published. For the estimation of total body water, we searched for ‘Peritoneal dialysis’ AND ‘volume’ AND ‘estimation’ and 16 papers were found.
Results
Importance of residual renal function over peritoneal clearance
Evidence prior to 2005
The original guideline highlighted that residual renal function (RRF) appeared to be more predictive of survival of people doing PD. This was largely based around five studies all published between 1999 and 2003. The ADEMEX study was a multicentre prospective, randomised, controlled clinical trial performed in 24 dialysis centres in Mexico that recruited 965 people on PD and randomised them to two different levels of small solute clearance (residual and peritoneal clearance combined). 2 This study demonstrated that while RRF was associated with mortality, peritoneal Kt/V was not; however, this was not the primary outcome of the study. In addition, there was a large observational cohort study in the United States (US) on 1603 people doing PD and demonstrated that RRF but not peritoneal clearance was associated with survival. 5 The relationship was confirmed in a single-centre prospective study on 270 prevalent and incident Chinese PD patients. 6 However, an extended follow-up study (mean follow-up of 35 months) on this 270 Chinese doing PD did demonstrate that peritoneal Kt/V was significantly associated with mortality, for each 0.1 increase in peritoneal Kt/V, there was a relative risk of death of 0.94 (95% confidence interval (CI): 0.89, 0.99). 7 A reanalysis of the CANUSA study (a prospective cohort study performed in 14 centres in Canada and the United States that recruited 680 people doing PD) demonstrated that for every 5 L/week/1.73 m2 of increased glomerular filtration rate (GFR), there was an associated 12% reduction in the relative risk of death (95% CI 0.83, 0.94) plus once again showing no relationship between peritoneal clearance and mortality. 8 Finally, a prospective study on 413 people doing PD from the Netherlands demonstrated a significant 12% reduction in mortality for each 1 mL/min/1.73 m2 increase in residual GFR but no relationship between peritoneal clearance on survival. 9
There was an additional study published prior to 2005 that was not included in the previous guidelines. This US study is based on 54 PD units that randomly selected people from each unit to include 1446 people doing PD. 10 After 7 months of follow-up, there was a statistically significant association between RRF and mortality, each 10 L/week/1.73 m2 increase in creatinine clearance was associated with a 40% decreased risk of death and for each 0.1 increase in Kt/V with a 12% decreased risk of death. No association between peritoneal clearance and mortality was noted.
Evidence since 2005
There have been no RCTs since the original guideline to help inform this area. Seven additional observational cohort studies have been identified, with the first one examining 540 out of a total of 620 incident people doing PD in a single centre in Korea. This study demonstrated that for every 1 mL increase in residual GFR, there was a 7% reduction in mortality (95% CI 0.88, 0.98), with peritoneal clearance not being significantly associated with mortality. 11 Guan et al. described a Chinese retrospective cohort study of 102 people doing PD and demonstrated that RRF but not peritoneal clearance was associated with mortality and death-censored technique failure. 12 This study was performed within a single centre but had restrictive inclusion/exclusion criteria (including only having people with diabetic nephropathy from type 2 diabetes mellitus), leading to recruitment of 102 out of a total of 1115 people doing PD within the recruitment period at that centre.
The rate of decline of RRF has also been shown to be prognostic of the outcome of people on PD. A Taiwanese prospective cohort study divided 255 incident people on PD into three groups – anuric, ‘fast decliner’ and ‘slow decliner’ groups. 13 They demonstrated similar peritoneal clearances between these three groups but increased mortality in the anuric and ‘fast decliner’ groups compared to the ‘slow decliner’ group. Similar findings of an increased risk of mortality with a more rapid decline in RRF were seen in a retrospective US study of 581 people doing PD but the effect of peritoneal clearance was not examined. 14 In a retrospective study of 493 people doing PD from four renal units in Spain, they demonstrated a significant association between baseline RRF and the rate of its decline with mortality, in addition to an interaction between these two variables, though peritoneal clearances were not included in their analysis. 15
A retrospective analysis of the Australia and New Zealand Dialysis and Transplant Registry did, however, demonstrate that RRF and peritoneal urea clearances were independently associated with mortality. 16 In this study of 2434 (out of a total of 3841) people doing PD, RRF was associated with improved survival, with every 10 L/week/1.73 m2 of residual creatinine clearance associated with a hazard ratio of death of 0.93 (95% CI 0.98, 0.99). This multivariate model also demonstrated that compared to a baseline peritoneal Kt/V of 1.70–2.00, those with a peritoneal Kt/V < 1.45 had a hazard ratio of death of 1.87 (95% CI 1.24, 2.84). An additional retrospective study was published from a single centre in Taiwan, which demonstrated that a more rapid decline in RRF was associated with an increased risk of death. 17 However, no assessment was made of the association of peritoneal clearance and death. Notably, 270 out of a total of 421 people doing PD were included in this study with 70 anuric people on PD being excluded from the analysis.
Recommendations
The evidence since the 2005 guidelines do not sufficiently add anything to strengthen or alter the previous recommendations: RRF has been consistently demonstrated to be associated with mortality in people doing PD and therefore should be maintained (practice point). Peritoneal clearance has not been consistently associated with mortality in people doing PD. Table 1 summarises the studies that support the importance of RRF over peritoneal clearance.
Summary of studies: Importance of RRF over peritoneal clearance.
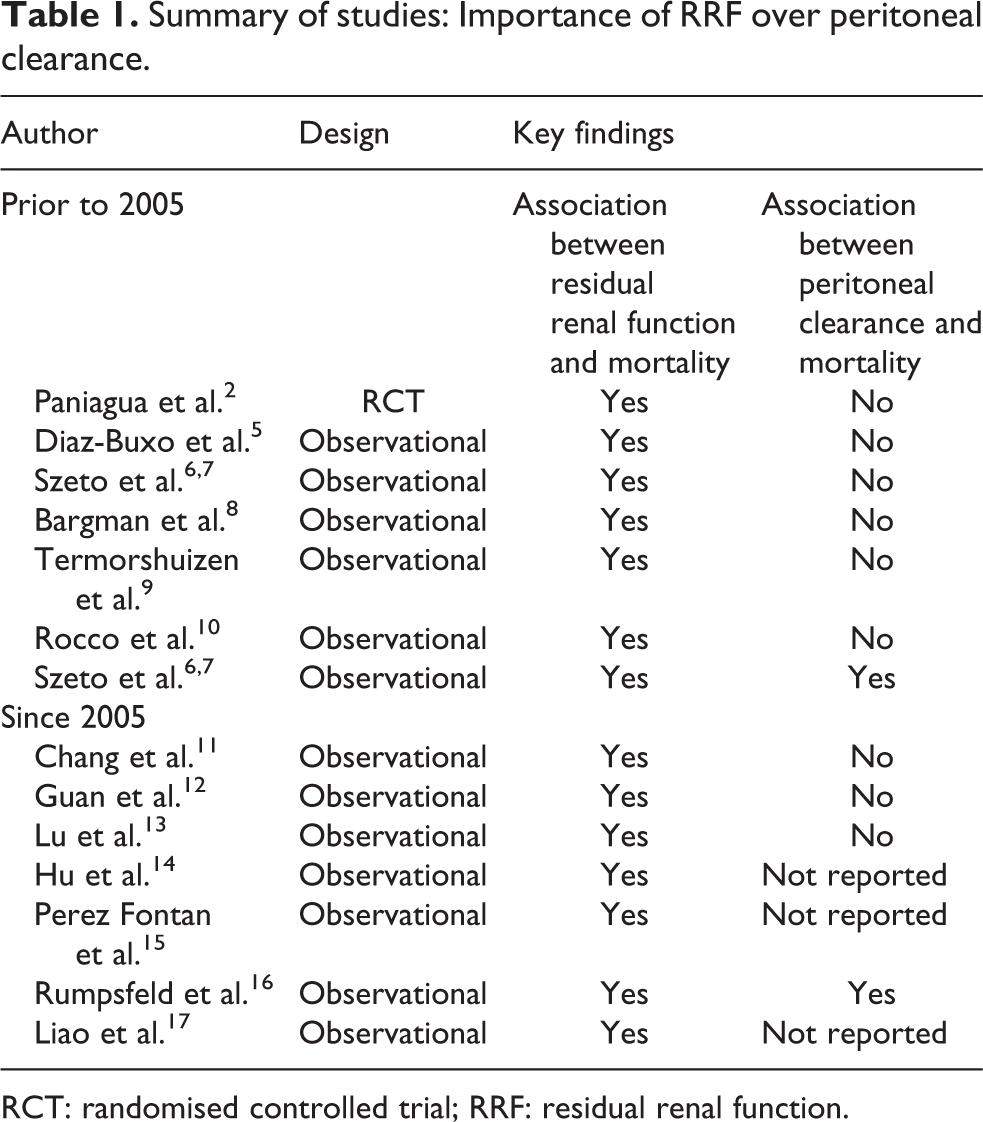
RCT: randomised controlled trial; RRF: residual renal function.
Combination of RRF and peritoneal clearance is not based on any evidence
There is, in fact, no evidence on the mathematical summation of RRF and peritoneal clearance though this has become common practice. 7,9 A retrospective study from Thailand that included 1177 people doing PD between January 2008 and April 2011 and had required laboratory data examined this area. 18 They described a statistically significant association between a residual renal Kt/V <0.25 and a total (residual plus peritoneal) Kt/V <1.75 to be associated with an increased risk of mortality, though it was difficult to discern if the majority of the association with total Kt/V was due to RRF.
Recommendation
Despite the lack of evidence in the summation of residual and peritoneal clearances, we recognise the convenience in doing this (practice point).
Total Kt/V targets – Upper limit
Evidence prior to 2005
There have been two key RCTs to inform us on the upper limit targets for total Kt/V. 2,4 The first was the ADEMEX study on 965 people doing continuous ambulatory peritoneal dialysis (CAPD) that were randomised to either standard care of 4 × 2 L PD bags per day or to achieve a peritoneal creatinine clearance of 60 L/week/1.73 m2. 2 After a minimum follow-up of 2 years, survival was equivalent in the two groups with a relative risk of 1.0 (95% CI 0.80, 1.24). The average total Kt/V in the intervention group in the ADEMEX study was 2.27 ± 0.02 versus the standard care group of 1.80 ± 0.02. When the investigators assessed for risk factors associated with mortality for the entire study population, RRF but not peritoneal clearances were statistically significant. In addition, ADEMEX found no difference in the quality of life between the two groups. In another open-labelled RCT in Hong Kong, 320 incident people doing CAPD from six dialysis units were randomised to one of three total Kt/V targets: 1.5–1.7, 1.7–2.0 and >2.0. 4 Survival after 2 years was similar in all three groups.
Evidence since 2005
There have been no further studies that add evidence to this area.
Recommendations
Combined, the two previous studies described suggest that there do not appear to be much advantage in achieving a total Kt/V above 1.7–1.8 (grade level 1B).
Total Kt/V targets – Lower limit
Evidence prior to 2005
In the RCT from Hong Kong, they did demonstrate that the lowest total Kt/V target group (1.5–1.7) did record significantly more adverse events and anaemia; however, these were secondary end points and predisposed to subjectivity within an open-labelled trial. 4 The prospective multicentre Netherlands Cooperative Study on the Adequacy of Dialysis (NECOSAD) started in January 1997 and included 542 people doing PD of which they published on 130 that developed anuria by the first of September 2002. 19 They demonstrated that in this anuric group, a Kt/V <1.5 and a creatinine clearance <40 L/week/1.73 m2 were associated with an increased relative risk of mortality after 2 years of 3.28 (95% CI 1.25, 8.60). The Hong Kong group published a retrospective study of 150 anuric people doing PD and demonstrated increased mortality in those with a baseline Kt/V <1.67. 20
Evidence since 2005
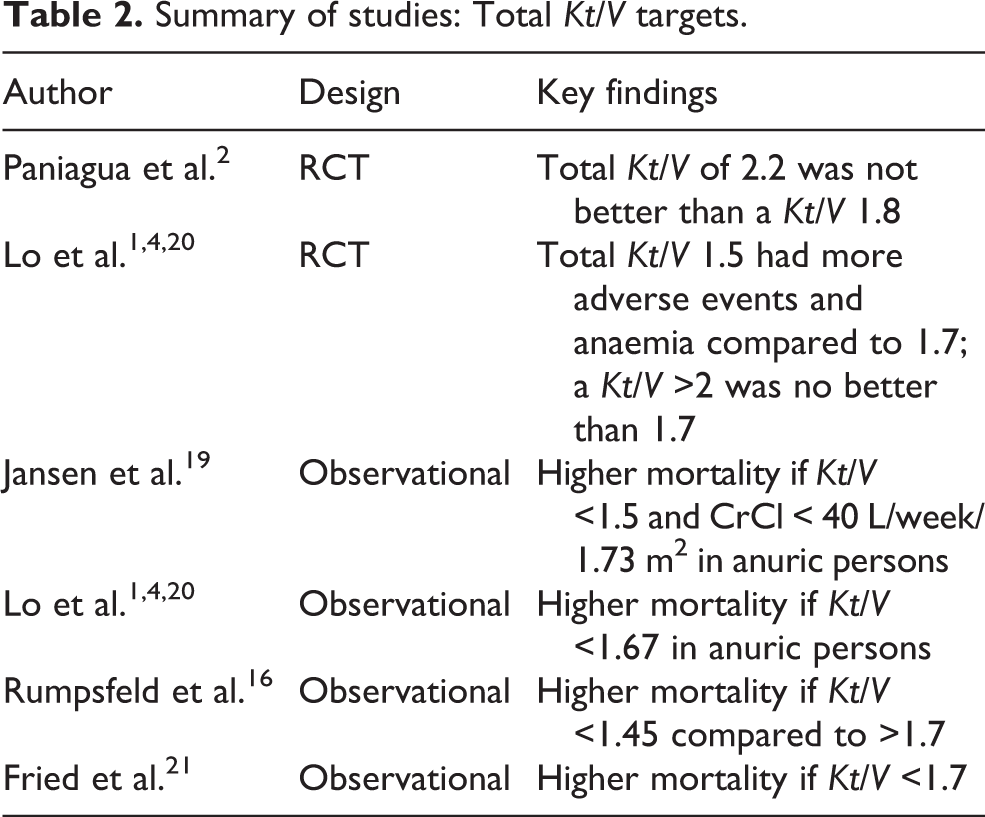
No high-quality studies have been published since 2005. The retrospective, registry study by Rumpsfeld et al. suggested that a peritoneal Kt/V <1.45 was associated with increased mortality compared to a peritoneal Kt/V of 1.70–2.0. 16 A retrospective study in the US examined 1432 anuric people doing PD from 1 January 1994 to 31 January 2005 and demonstrated that a Kt/V <1.7 was associated with a significantly increased risk of mortality, p = 0.03. 21 A summary of studies looking at Kt/V targets is presented in Table 2.
Summary of studies: Total Kt/V targets.
Summary of studies: Ultrafiltration and outcomes.
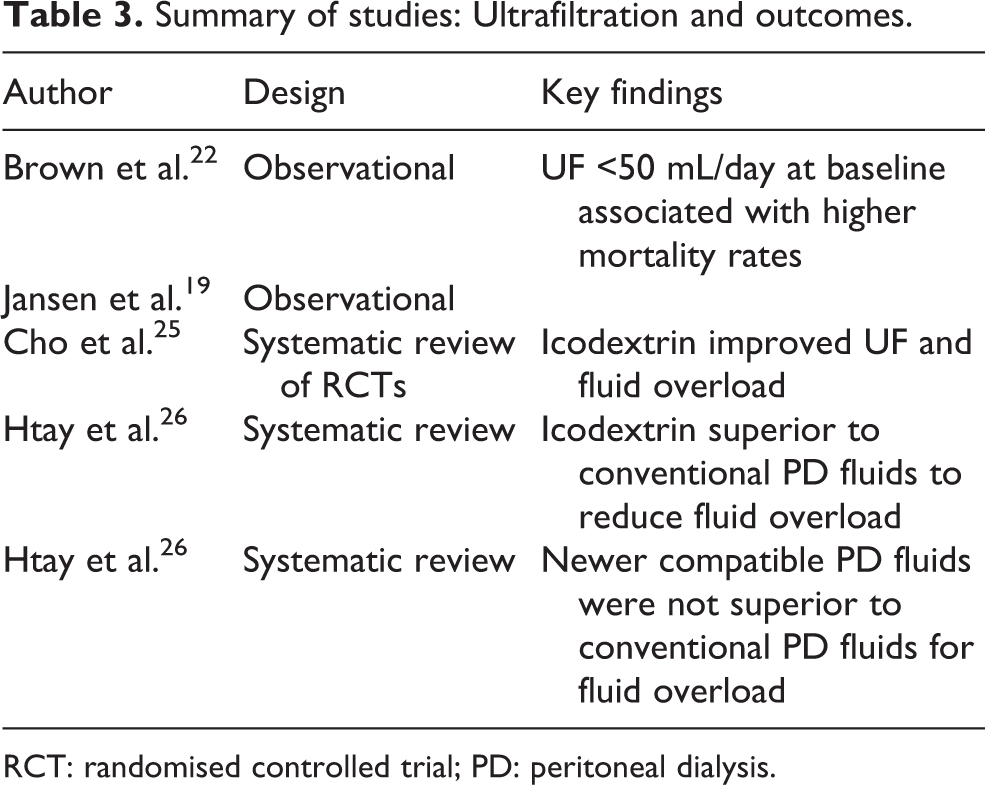
RCT: randomised controlled trial; PD: peritoneal dialysis.
Recommendations
These studies suggest a Kt/V of at least 1.7, especially if the person on PD is anuric, but the level of evidence for this recommendation is low (practice point).
Ultrafiltration and outcomes
Evidence prior to 2005
UF is essential for the control of hypervolemia, a known risk factor for overall and technique survival of people on PD and people without residual function are the subgroup at higher risk. 22 Prior to the recommendations of 2005, the European APD Outcome Study (EAPOS) demonstrated that UF was predictive of survival in anuric people on APD: a baseline UF below 750 mL/day was associated with poorer survival, although the time-averaged UF was not analysed time dependently and some controversy exists due to an association between UF and malnutrition in people with anuria. 22 Similar findings were found in the NECOSAD study, where UF was analysed as a continuous variable and was also identified as a risk factor for survival in the time-dependent analysis of anuric people. 19 All these studies were observational in nature and important confounders were not always adjusted for. At the time, it was not possible to establish a numerical target for UF, and the recommendations were to individualise treatment taking into account clinical signs of volume overload and quality of life. 23,24
Evidence since 2005
There was no significant change in this topic since 2005 in terms of definition of targets for daily UF aiming to reduce hard outcomes. However, since 2005, several studies were published analysing the impact of icodextrin and the newer biocompatible PD solutions on UF and in the control of hypervolaemia. The superiority of icodextrin compared to glucose as osmotic agent to increase UF was demonstrated in two large meta-analyses. In the meta-analysis of 2013, combining data from 11 studies and 1222 people on PD, icodextrin improved peritoneal UF and reduced episodes of fluid overload without any impact on RRF. 25 More recently, a Cochrane systematic review and meta-analysis confirmed icodextrin as superior to conventional PD solutions to reduce episodes of uncontrolled fluid overload and increase peritoneal UF. 26
In terms of the newer PD biocompatible solutions, their effect on UF is more controversial. The 2018 Cochrane systematic review considered these solutions to have little if any effect on UF (4-h peritoneal UF) compared to conventional PD solution. 26 Table 3 summarises the studies of UF and outcomes cited in this review and their key findings.
Recommendations
The UF goal should always be individualised aiming euvolaemia. In the presence of signs of hypervolaemia, one should always investigate potential contributing factors, such as excessive liquid ingestion, loss of RRF and changes in the membrane permeability through the peritoneal equilibration test (practice point).
Discussion
At the time of publication of the 2005 ISPD guideline on targets for solute and fluid removal in adults on chronic PD, there still remained a focus on small solute clearance as a key measure of the adequacy of dialysis. 1 Since the publication of the last guidelines on this topic, there has been a distinct paucity of high-level evidence to inform this area of clinical practice. Most of the evidence have been from observational cohort studies or retrospective studies, which at the most provides grade level C evidence. These findings really question the previous focus on small solute clearance in the management of people doing PD.
A consistent finding in the literature has been the association between RRF and mortality. 5 –9 While this has been published in multiple prospective cohort studies and a number of retrospective studies, there have been no RCTs in this area to inform its clinical application. Despite the consistency of the results in multiple regions of the world, all with a similar magnitude of effect (2.4–12% risk reduction in mortality with each 1 mL/min/1.73 m2 of RRF) do support the suggestion that the relationship is real. In addition, there is clear biological plausibility for this to be a causal relationship.
It, therefore, makes intuitive sense to recommend that every effort should be made to maintain RRF, though the methods to achieve this are outside of the scope of this article except to state that the evidence is poor for most of this area too. The potential interventions would include avoiding nephrotoxins; ensuring adequate intravascular volume; antagonists to the activation of the renin–angiotensin system, good diabetic control and the use of biocompatible PD solutions. 26 Ideally, therefore, it would be prudent to have an RCT with an intervention that preserves RRF and then to examine whether this then leads to a significant reduction in mortality.
Unlike RRF, peritoneal clearances have not consistently been shown to be associated with poor outcomes. 7,9 Despite this, it is a common place to calculate total weekly clearance as the sum of residual renal clearances and peritoneal clearances. The arithmetic sum of these two variables is not based up any evidence and clearly does not reflect clearance of all uraemic toxins. However, it is recognised the convenience of this calculation and its widespread practice.
The two RCTs in the area of small solute clearance showed similar results with no difference in mortality after 2 years of follow-up between groups with a range of targets of small solute clearance, aimed at testing the hypothesis that increasing small solute clearance above standards at that time would reduce mortality. 2,4 These findings suggest that increasing small solute clearance, to the limits of currently available technology, does not translate to improved survival of people doing PD.
One of these RCTs included a group with weekly Kt/V targets of 1.5–1.7, and while mortality was no different with the higher Kt/V groups, there was increased morbidity. 4 There has otherwise been limited evidence to inform us on the preferred lower limit of weekly Kt/V. If we focussed on anuric people doing PD, then there is some low-level evidence for a lower limit for weekly Kt/V. 16,19 –21 These studies have been limited to a subgroup analysis of a multicentre prospective cohort study and a series of retrospective studies. These studies have identified that there is a lower limit for weekly Kt/V below which there is an association with increased mortality, with the threshold varying between 1.45 and 1.70. The consistency and geographically widespread nature of these findings suggests that at least in anuric people doing PD, there may be a threshold Kt/V above which it is desirable for them to achieve.
It also needs to be recognised that there is considerable potential confounding in the calculation of Kt/V due to the method used in the calculation of body composition. We would refer the reader to the chapter that specifically covers this topic. 23
Hypervolaemia is a risk factor for overall and technique survival of people doing PD 27 and those without residual function are the subgroup at higher risk. 28 UF is essential for a good fluid balance and it was predictive of survival in anuric people doing APD in the prospective observational EAPOS: baseline UF below 750 mL/day was associated with poorer survival, but the time-averaged UF was not analysed time dependently. 22 Similar findings were found in the NECOSAD study, where UF was analysed as a continuous variable and was also a risk factor for survival in the time-dependent analysis of anuric people doing PD. 19 Given the impossibility to establish a numerical target for UF, the treatment should be individualised taking into account clinical signs of volume overload and quality of life.
Since the publication of the 2005 guideline, several studies evaluated the impact of different osmotic agents on UF. Icodextrin used in the long dwell was the most effective osmotic agent and a systematic review of 11 trials and 1222 people on PD demonstrated the superiority of this osmotic agent on UF with no adverse effects or impact on RRF. 25
Finally, it is important to emphasise other measures that may reduce the need to obtain higher UF volumes as fluid intake restriction. However, data on the effectivity of strategies to improve adherence to fluid restriction are scarce on literature. The only RCT available found that weekly group therapy significantly changes oedematous status of people classified as non-adherent to diet at baseline. 29 Furthermore, for all topics covered in this manuscript, the majority of studies were observational rather than randomised and the presence of confounders is common and should be taken into consideration when analysing the information.
In conclusion, the lack of high-level evidence on the prescription of PD with respect to small solute clearance and UF volume targets suggests that these should not be a major focus in the management of people doing PD.
Footnotes
Acknowledgement
We would like to thank the reviewers of this manuscript and all colleagues from ISPD for their suggestion to improve the manuscript.
Author contributions
TM and NB researched literature and conceived the study. TM and NB wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TPM has received speaker honoraria from AstraZeneca, Lilly-Boehringer and Baxter Healthcare. NB received a travel grant and honorarium from Baxter; travel grants from Amgen and Roche.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.