
Abstract
Background:
Immune cell dysfunction is listed among complications resulting from chronic kidney disease (CKD). It could be associated with T-cells, which play a role in the lymphocytic migration and infiltration. However, the data on chemokine receptors expression on T-cells in patients with CKD particularly treated with peritoneal dialysis (PD) are still limited.
Methods:
The study aimed at multiparameter flow-cytometric analysis of the absolute numbers and percentage of T-cell subsets with surface chemokine receptors (CCR4, CCR5, CCR7, CXCR3, and CXCR4) or receptors’ combinations in 47 children treated with PD.
Results:
We found lower absolute numbers of total T lymphocytes, lymphocytes with surface CCR5, CXCR4+CCR5, CXCR3+CCR5 antigens and T-cells with CCR4, CCR4+CD4, CXCR3, CXCR3+CD4, and CD8 receptors. Lymphocytes T with CD4, CCR7, CD28+CCR7, CXCR3+CD8 antigens showed higher percentage in children on PD as compared to healthy children and opposite percentage values of CCR4+, CCR4+CD4+, CXCR3+ T lymphocytes were diminished. Mean fluorescent intensity for CCR7+, CCR7+CD45RO+, CCR7+CD28+, CXCR4+CD4+, CCR5+CD4+, CCR4+, CCR4+CD4+ T-cells was lower in the PD group than in healthy children. The analysis of correlation between T lymphocyte subpopulations with chemokine receptors and other parameters revealed positive correlation of CCR7+ and CCR7+CD28+ T-cells and weekly creatinine clearance, negative correlation between the percentage of CD45RO+CCR7 antigen positive T-cells and KT/Vurea.
Summary:
In conclusion, we could not confirm the phenomenon of earlier senescence of T-cells in children with CKD on PD treatment. This still requires further investigation. The higher percentage of T-cells with CCR7 surface receptor could be responsible for the increase of proliferation activity in this group of children.
Introduction
The chemokine-receptor system plays the crucial role in the regulation of both innate and adaptive immunity, therefore it provides appropriate immune response in healthy individuals. Chemokines, described as low molecular-weight proteins, are responsible for chemoattraction. Binding to the corresponding receptors, chemokines activate signaling pathways, that results in cell migration, differentiation, and proliferation, in physiological, as well as in pathological conditions. 1 Chemokine receptors are structurally seven-transmembrane proteins, also known as G protein-coupled receptors. 2 These molecules have been divided into subfamilies such as CCR, CXCR, CX3CR, or XCR, numbered in accordance with an order of their discovery. 3 –5
Human CC chemokine receptor type 5 (CCR5) has been identified as the receptor for chemokines such as macrophage inflammatory protein 1α (CCL3), macrophage inflammatory protein-1β (CCL4), and regulated on activation, normal T-cell expressed and secreted (RANTES; CCL5), 6 which also acts as a co-receptor that allows R5-HIV-1 entry into cells, when co-expressed with CD4. 7
Immune cell dysfunction is listed among complications resulting from chronic kidney disease (CKD). It is believed that the process might be associated with T-cells, due to CCR7 receptor expression on their surface and an influence on the lymphocyte migration and infiltration. It was previously documented that the uremic milieu induces premature aging of T-cells. 8 However, the data on chemokine receptors expression on T-cells in patients with CKD particularly treated with peritoneal dialysis (PD) are still limited 6,7
Miao et al. demonstrated that AMG487 (small-molecule CXCR3 antagonist) combined with cyclosporine A has effectively reduced the prevalence of graft versus host disease (GvHD) and increased the survival time. This compound has also remarkably inhibited the infiltration of inflammatory cells in GvHD target tissues in a murine aGvHD model, as well as inhibited the production and differentiation of splenic donor-derived T-cells. 9 Paust et al. suggested that specific targeting of CXCR3 on TH1 cells might be effective in TH1-driven inflammatory diseases including crescentic glomerulonephritis. 10
The CXCR4 protein (chemokine CXC motif receptor 4, also called the CD184 antigen or LESTR antigen, a leukocyte-derived seven-transmembrane domain receptor) is a receptor for stromal 1 cell factor (SDF-1; chemokine CXC motif ligand 12 (CXCL12)). CXCR4 performs its main functions together with its ligand both in the mobilization of the stem cells into the bloodstream and during homing, hence the colonization of the marrow niches after the cells transplantation. 11 Increased expression of the CXCR4 receptor is a vital element in the diagnosis and prognostic assessment of the rhabdomyosarcoma. 12
A significant therapeutic potential of these co-receptors is also described in several other processes, such as tissue repair or regeneration and inflammation. 13 Maluf et al. showed that CXCR4 has been upregulated in fibrotic lesions in renal biopsy samples. 14 During experimental study on animals, Zou et al. found out that blocking the CXCR4 resulted in improvement of the renal interstitial fibrosis in surviving allografts by downregulation of transforming growth factor β1 concentration. 15
In the inflammatory process, there is a high concentration of chemokines that cause the attraction of multiple chemokine receptor-expressing lymphocytes. The studies on animal models in lupus nephritis highlighted the role of chemokines in autoimmune systemic reactions in various tissues, including renal tissues, and proved their responsibility for local renal inflammation with direct effects and subsequent damage eventually leading to irreversible CKD. 16 Current investigations target their efforts to design treatment limiting inflammation. Such agents, presumably consisting of small molecules alongside with monoclonal antibodies, would aim to block the interactions between chemokines and chemokine receptors by neutralizing either one of them. Therefore, the research on chemokine receptors in children undergoing PD might bring to light some new strategies in preventing an enhanced inflammatory response during stage 5D CKD and after kidney transplantation.
Aims
The study aims at multiparameter flow-cytometric analysis of the absolute numbers and percentage of T-cell subsets with selected surface chemokine receptors or receptors’ combinations in children treated with PD.
Materials and methods
The study involved 47 children and young adults with CKD (22 girls and 25 boys) treated with PD at the Department of Dialysis of Children at the Chair and Clinic of Pediatrics in Zabrze, Medical University of Silesia in Katowice. The characteristics of the group are presented in Table 1. In the PD group, the study was performed during routine checkups. There were no signs of infection in the examined group of children. Determination of hemoglobin, erythrocytes, leukocytosis, and lymphocytosis was performed with the MicroDiffII hematology analyzer (Becton Coulter, Fullerton, CA, USA). The concentration of hemoglobin was expressed in g/dl, the number of erythrocytes was expressed as 1 × 1012/l, the number of leukocytes and platelets as 1 × 109/l, hematocrit was expressed as a percentage. The concentration of creatinine and urea in the blood serum (Kodak Ektachem 700; Kodak, Rochester, NY, USA) were evaluated in the biochemical laboratory tests. Creatinine concentration was expressed in µmol/l, urea concentration in mmol/l.
Baseline clinical characteristics and selected laboratory tests result in studied children.a
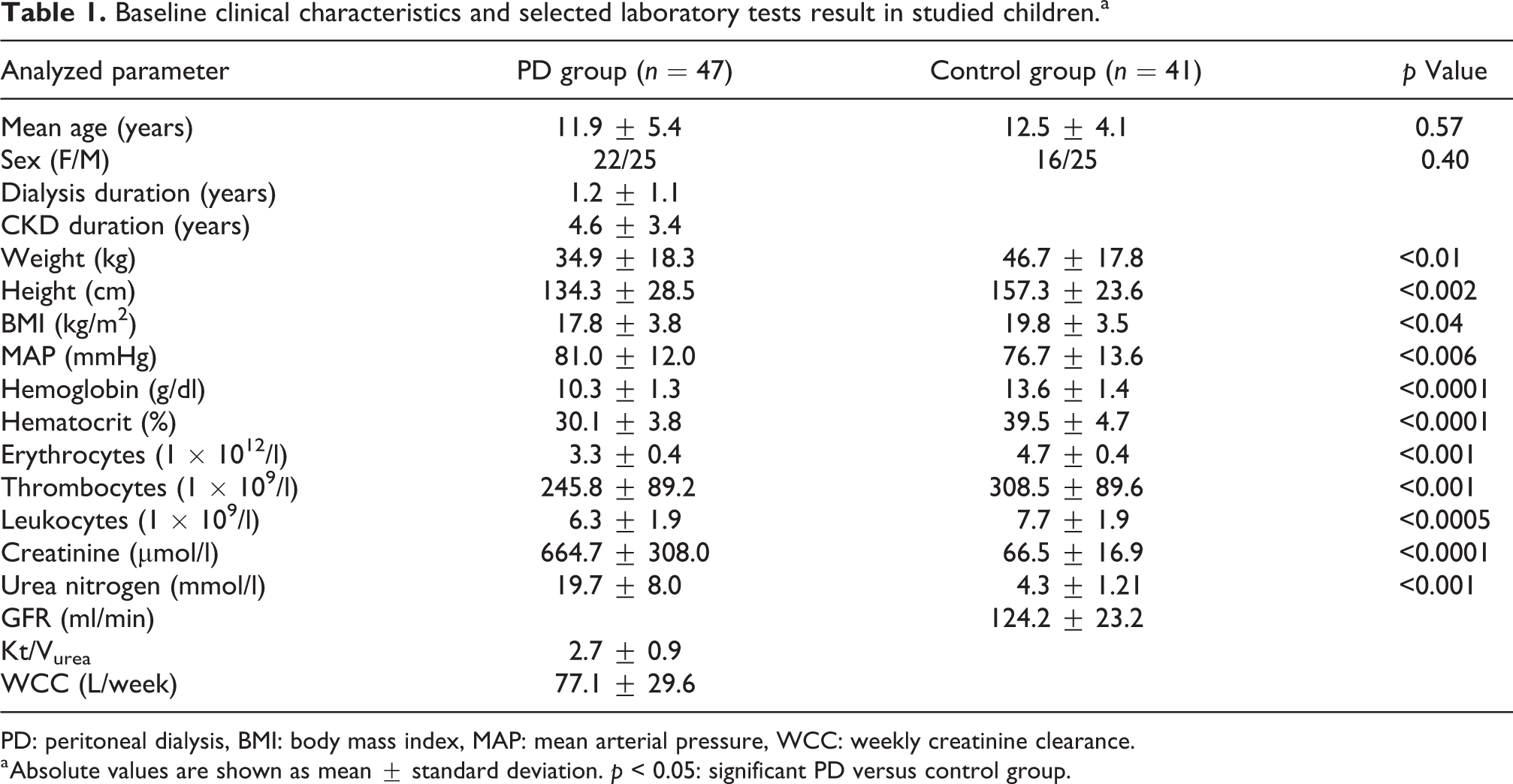
PD: peritoneal dialysis, BMI: body mass index, MAP: mean arterial pressure, WCC: weekly creatinine clearance.
a Absolute values are shown as mean
The mean duration of dialysis was estimated, and the Kt/Vurea dialysis ratio and weekly creatinine clearance (WCC) were calculated in children on PD. WCC in automatic PD was considered adequate for values ≥70 l. Kt/Vurea, as for children with PD values ≥2.1, indicated an adequate dialysis.
All children underwent blood pressure (BP) measurement and mean arterial pressure was calculated (MAP = 1/3 difference in systolic and diastolic pressures + diastolic pressure), body surface area and body mass index (BMI; body mass divided by the square of the body height, kg/m2) were also estimated (Table 1). BP values, expressed in mmHg, were considered abnormal if they exceeded the 95th percentile for age, sex, and height. BMI values were adjusted for sex and classified as lower than 5 percentile: malnutrition; 5–85: normal weight; above 85 percentile: —overweight; and above 95 percentile: obesity.
The control group (ZD) was represented by 41 healthy children (16 girls, 25 boys). These patients were admitted to the hospital due to nocturnal enuresis or for elective surgery (day surgery). BP values and renal function indices in this group were within the normal range for sex and age. Estimated glomerular filtration rate was calculated using the Schwartz formula [ml/min/1.73 m2]. 17
Methods of the cytometric parameters determination
Each patient had 2 ml of blood withdrew by puncture of a peripheral vein in order to perform flow cytometry. Blood samples were collected using anticoagulant (unfractionated heparin) and then analyzed within 4 h. Immunophenotyping of each sample was performed by six-color flow cytometry on a BD FACSCanto II flow cytometer (Becton Dickinson, Biosciences, San Jose, California, USA). The whole blood labeling method followed by the lysis of erythrocytes was used. A panel of 11 combinations of monoclonal antibodies was chosen to determine individual lymphocyte populations in accordance with a standard staining protocol. Combinations of antibodies from the diagnostic panel are presented in Table 2.
The panel of monoclonal antibodies for lymphocyte subpopulations flow cytometry.
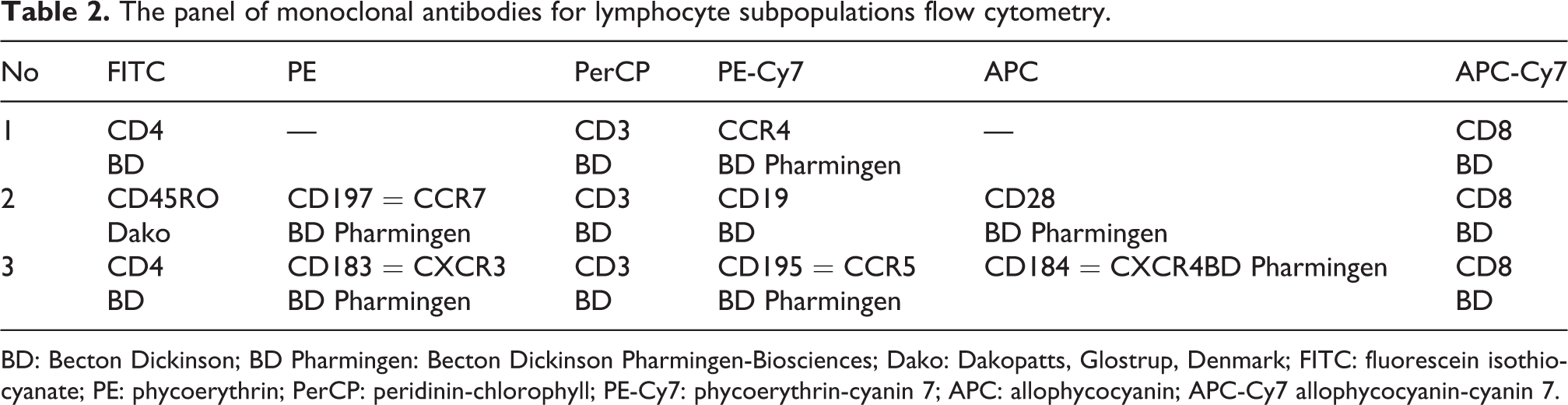
BD: Becton Dickinson; BD Pharmingen: Becton Dickinson Pharmingen-Biosciences; Dako: Dakopatts, Glostrup, Denmark; FITC: fluorescein isothiocyanate; PE: phycoerythrin; PerCP: peridinin-chlorophyll; PE-Cy7: phycoerythrin-cyanin 7; APC: allophycocyanin; APC-Cy7 allophycocyanin-cyanin 7.
After the proper time of incubation, the erythrocytes were lysed with FACS Lysing Solution (Becton Dickinson Biosciences). Subsequently, the samples were rinsed in PBS (NaCl, Na2HPO4, NaH2PO4, NaN3, pH (25°C) 7.2 ± 0.1) and then loaded into the flow cytometer.
Data were recorded and then analyzed using a Diva computer program (Becton Dickinson, Immunocytometry Systems, San Jose, California, USA). The FACSCanto II flow cytometer was subjected to daily quality control using the Rainbow Beads microspheres (Spherotech Inc., Greek Oaks, Illinois, USA).
Statistical analysis of the results
The data were analyzed using the STATISTICA 12.0 PL program (StatSoft, Inc. 2014). For the parameters tested, basic descriptive statistics were made and the mean value, median, minimum, and maximum values were determined. For all parameters, their distribution was checked for compatibility with the normal distribution using the Shapiro–Wilk test. The homogeneity of variance was tested using the Levene test. For a comparison of variables with a normal distribution, parametric tests with a separate variance assessment were performed. For comparative analysis of variables with distribution deviated from the normal distribution, nonparametric Mann–Whitney U test was used. The Pearson linear correlation test or Spearman rank correlation enabled to determine the correlation between parameters. The test results were presented graphically in the form of tables. The values fulfilling the condition p < 0.05 were considered statistically significant.
Results
Table 1 summarizes the baseline characteristics of the studied population. Children on PD were described with lower body weight, height, BMI, and higher MAP values. Regarding complete blood count in this group, the red blood cell count, white blood cell count, and platelet count, hemoglobin concentration and hematocrit values were significantly lower in comparison with the control group. Serum creatinine level and blood urea concentration were increased as in stage 5D CKD.
Tables 3 and 4 present the comparison of absolute values and percentage of T lymphocytes with selected chemokine receptors in the group of children on PD and healthy controls. The outcome revealed decreased absolute numbers of total T lymphocytes, lymphocytes with surface CCR5, CXCR4+CCR5, CXCR3+CCR5 antigens and T-cells with CCR4, CCR4+CD4, CXCR3, CXCR3+CD4 and CD8 receptors. Lymphocytes T with CD4, CCR7, CD28+CCR7, CXCR3+CD8 antigens percentage was more numerous in children on PD as compared to healthy children and opposite percentage values of CCR4+, CCR4+CD4+, CXCR3+ T lymphocytes were diminished. Mean fluorescent intensity for CCR7+, CCR7+CD45RO+, CCR7+CD28+, CXCR4+CD4+, CCR5+CD4+, CCR4+, CCR4+CD4+ T-cells was lower in the PD group than in healthy children (Table 5).
Absolute values of T-cell subpopulations, including populations with expression of receptors for selected chemokines in examined children and healthy controls.a
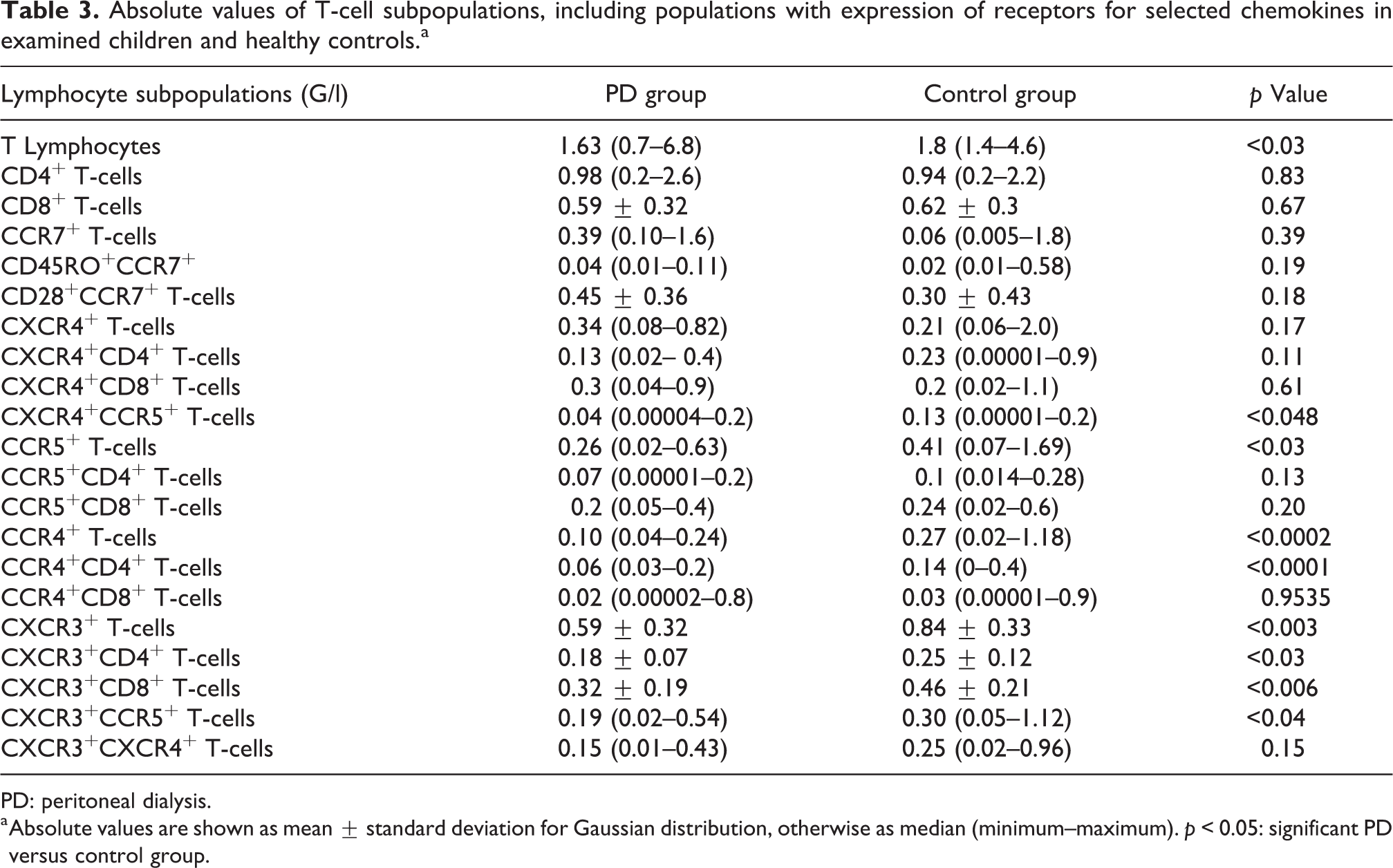
PD: peritoneal dialysis.
a Absolute values are shown as mean
Percentage values of T-cell subpopulations, including populations with expression of receptors for selected chemokines in examined children and healthy controls.a

PD: peritoneal dialysis.
a Percentage values are shown as median value (minimum–maximum). p < 0.05: significant PD versus control group.
Significant differences of MFI values of T-cell subpopulations with expression of receptors for selected chemokines between examined children and healthy controls.a
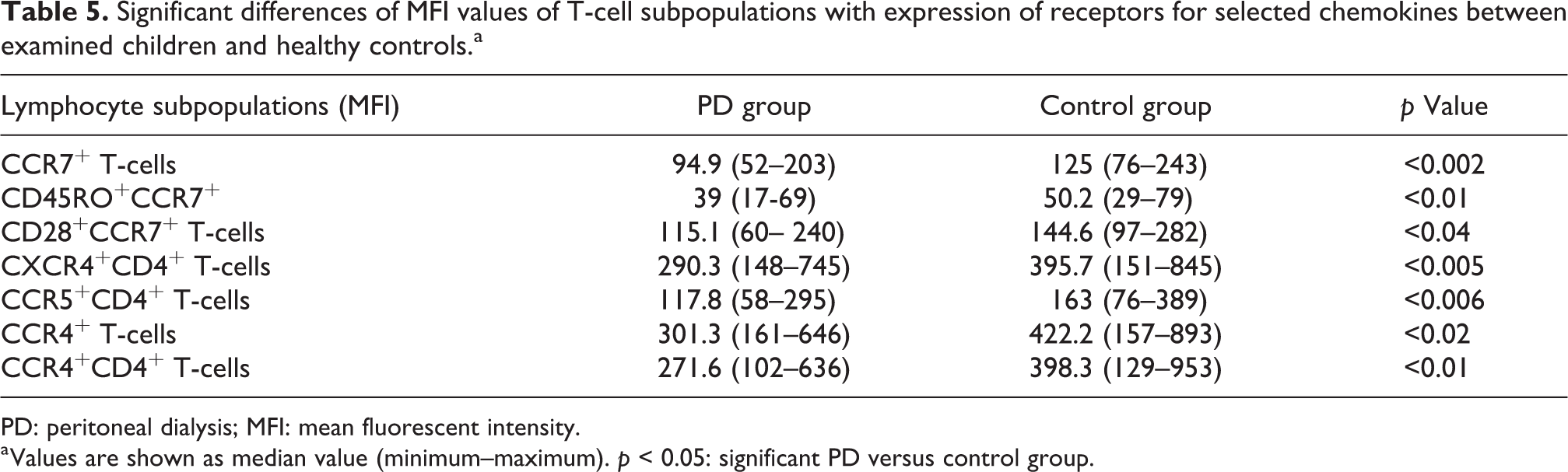
PD: peritoneal dialysis; MFI: mean fluorescent intensity.
a Values are shown as median value (minimum–maximum). p < 0.05: significant PD versus control group.
The results of the analysis of correlation between T lymphocyte subpopulations with chemokine receptors and other parameters, presented in Table 6, revealed positive correlation of CCR7+ and CCR7+CD28+ T-cells and WCC, negative correlation between the percentage of CD45RO+CCR7 antigens positive T-cells and KT/Vurea. Total number of CD45RO+CD28 antigens positive T-cells correlated positively with CKD duration (R = 0.4474, p < 0.05).
Significant correlations between T lymphocyte subpopulations with chemokine receptors and other parameters in children with chronic kidney disease on peritoneal dialysis.
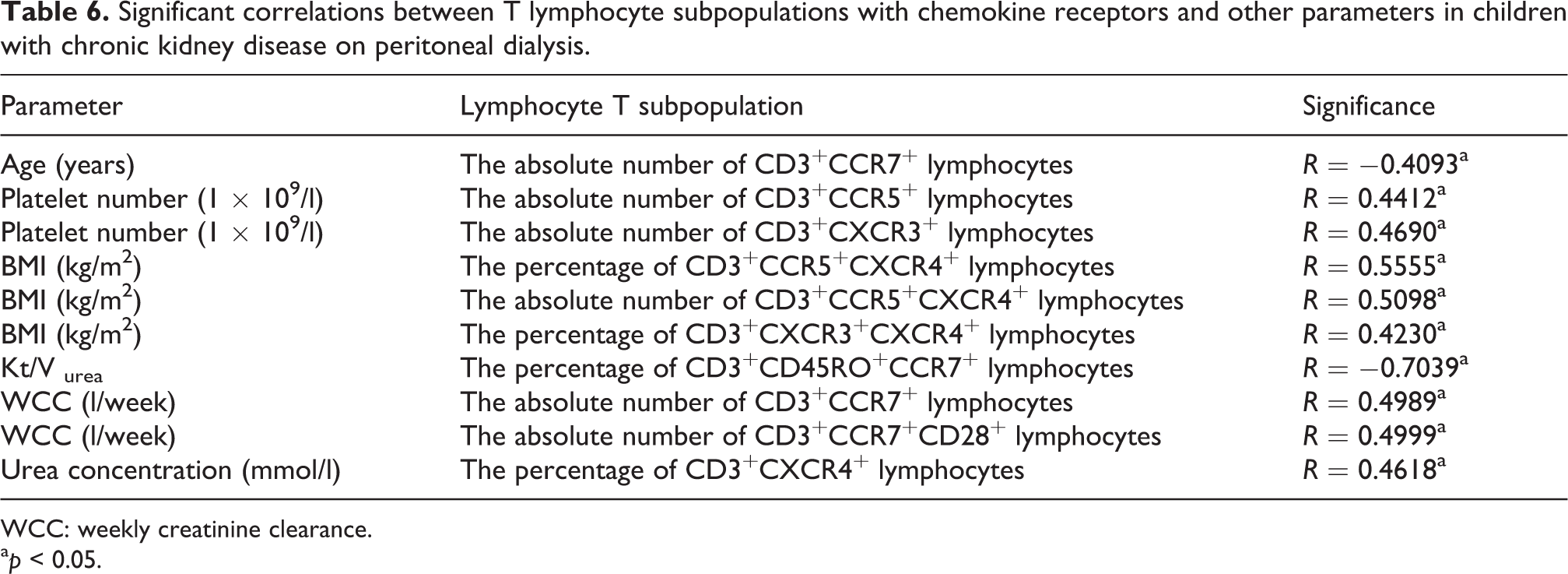
WCC: weekly creatinine clearance.
a p < 0.05.
Discussion
The magnitude of the immune response dependent on T lymphocytes, its potential and phenotype cannot be assessed on the basis of a single parameter. Hence the great significance of multicolor flow cytometry. This method allows to assess the proliferation of lymphocytes and the induction of other cells’ proliferation, as well as the mechanisms of the immune response and the evaluation of the effectors’ functions. The more the specific markers are discovered, the better the assessment of disorders in individual cell subpopulations can be performed. 18 This study has documented a significantly higher percentage of T-cell bearing surface CCR7 receptor in children with CKD undergoing PD, although the MFI of this receptor was lowered. Moreover, it presents the influence of PD on their percentage value showing negative correlation with Kt/Vurea (CD45RO+CCR7 T-cells) and on the other hand, positive correlation of CCR7+CD28+ T-cells and WCC. The additional effect of PD on cellular immunity, apart from conservatively managed CKD, was acknowledged. According to Freitas et al., aging alongside with CKD have an additive effect on decreasing T- and B-cells number. 19 Study by Betjes et al. suggested that CKD adult patients’ T-cells are 20–30 years older than healthy individuals. Such correlation was more prominent in older patient. 20 Chung et al. documented that peripheral blood central memory and effector memory T-cells count was increased in patients with uremia comparing to healthy adults. 21 Wurm et al. conducted a research on animal models, which concluded, that extra- and intraglomerular mesangial cells in healthy rats were CCR7-negative and furthermore, significant CCR7 expression during mesangial proliferation in the course of glomerulonephritis was revealed. 22 CCR7+CD8+ T-cells are believed to regulate the effector T-cells, involved in T-cell-mediated rejection in an in vitro and an ex vivo transplant model. 23 It is likely to assume that the configuration we reported displays action promoting proliferation in children on PD. Crépin et al. observed an early replicative aging in young patients with CKD linked to reduced thymic output. 24
Among the CD45RO+ memory T-cells, two subpopulations can be distinguished: first, central lymphocytes (TCMs, CM T-cells) expressing the CCR7 molecule, taking part in lymphoid tissue colonization, but not directly fulfilling the effector functions and second, effector memory cells (TEMs) that do not express this receptor. The co-receptor CD28 was often applied to define fractions of memory cells. Historically, downregulation of CD28 was usually associated with loss of functionality, especially described as weakened proliferative ability and loss of telomeres. 25,26 George et al. proved CD28 negative T-cells and CD57 positive T-cells increase, suggesting that it might take part in premature senescence. 27 However, in this research such T-cells phenomenon in children on PD could not be estimated, as higher percentage of CM T-cells, with CD28 and CCR7 receptors bearing on their surface, were detected and similar absolute number of such cells occurred in healthy controls. Therefore, it should be clarified in further investigations.
In the literature, there is no consensus on frequency of memory cells in CKD patients. Such ambiguities might originate from the fact that researchers tend to analyze various, selected subpopulations of lymphocytes which are structurally and functionally distinct. Moreover, in pediatric studies, the number of patients is usually limited. One should also take into account that CKD duration in children is shorter than in adults, uremia is acting on developing immune system and children have less comorbidities than older patients.
Biology of the receptors for chemokines is a wide field of study and many discoveries are yet to be unraveled, as the chemokines are known for 25 years so far. Interestingly, it was proved that there may be a parallel expression of several receptors for chemokines on the same cell, which activated would bring different results. Some cells of the lymphoid system appearing at the site of infection tend to present the receptors for chemokines with opposite action, that is why the accurate assessment of their function might be difficult. 6
The literature underlines the role of CCR5 in various diseases such as rheumatoid arthritis, multiple sclerosis, transplant rejection processes, diabetes mellitus, myeloma, and gastrointestinal disorders. CCR5 facilitates the intracellular migration of HIV-1. Szalai et al. pointed out that CCR5 dysfunction (gene polymorphism), due to the 32 base-pair deletion mutation (CCR5Δ32), is usually associated with better prognosis in atherosclerotic disease. 28 The CCR5Δ32 genotype is also correlated with longer survival in type 2 diabetes mellitus. 29 The relevance of CCR5 and CXCR4 receptors in allergic disorders in the lungs and remodeling (fibrosis) of lung tissue has been described. 30 Moreover, CCR5 affects proteinuria-related renal injury, as albumin and other filtered urinary proteins upregulate its ligand RANTES. Its expression was associated with the presence of interstitial CCR5-positive mononuclear cells including T lymphocytes and fibrosis in patients with acute interstitial nephritis. 31 Still, Moreno et al. concluded that anti-chemokines or anti-chemokine receptors compounds administering needs to be explored more and their interactions with conventional anti-inflammatory or anti-proteinuric treatment ought to be investigated. 32 According to Yuan et al., CXCR4 present in the tubular cell compartment in CKDs, particularly obstructive uropathy, promotes the secretion of cytokines, and influences macrophage trafficking and activation state, resulting in kidney fibrosis. 33
In all clinical areas, including inflammatory diseases (together with acute and CKD), the use of chemokine receptor antagonists is currently being explored. Blocking chemokine receptors might induce selective inhibition of monocyte pro-inflammatory phenotype and not affect immunoregulatory or anti-inflammatory monocytes. Studies on the efficacy of the CCR5 receptor antagonist in the treatment of AIDS remain in the phase of clinical trials. As for kidney diseases, the role of chemokines in the interaction between cytokines, vasoactive substances, and the corresponding target cells in the progression of chronic interstitial fibrosis has been underlined. Studies, based on kidney biopsy materials, showed that blocking pro-inflammatory cells with the CCR5 chemokine receptor would inhibit inflammatory processes and prevent organ transplant rejection. 34
PD is the modality widely used in children with CKD. This research reveals that children on PD present lower expression of chemokine receptors, reflected by diminished MFI values, specially connected with CD4+, which might contribute to an increased hazard of inflammatory complications. Various inflammatory mediators have been extensively studied in patients on PD. It was confirmed that PD takes part in the inflammatory response by activating IL-6 with its soluble IL-6 receptor, which eventually results in the stimulation of T-cells proliferation and differentiation. 35 Musiał et al. claimed that the monocyte chemoattractant protein and macrophage colony-stimulating factor concentrations in children on PD are decreased in comparison with subjects on hemodialysis and healthy controls. This finding introduces PD as a weaker trigger of systemic cell migratory activity, whereas similar neopterin concentrations suggest comparable status of chronic inflammatory stimulation. 36
In conclusion, the presence of the phenomenon of earlier T-cells senescence in children with CKD on PD treatment could not be confirmed. Consequently, such research still requires further investigation. The higher percentage of T-cells with CCR7 surface receptor could be responsible for the increase of proliferation activity in this group of children.
Footnotes
Acknowledgements
None
Author contributions
MS was involved in protocol development, gaining ethical approval, patient recruitment and data analysis, drafted the article. ŁS and JB were involved in performing cytometric analysis and interpretation of data. BM was involved in literature search and protocol development. DZ and MT were involved in protocol development, patient recruitment, and data analysis. JK performed statistical analysis and was involved in data analysis. TS evaluated cytometric analysis and critically reviewed the content. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The approval of the SUM Bioethical Committee in Katowice NN-6501-131/06 from 20 September 2006 was obtained.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Polish Ministry of Science and Higher Education grant no. N407 008 32/0179.
Informed consent to participate
Parents and children over the age of 13 years have signed written informed consent for research.
Informed consent to publish
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article
Trial registration
Not applicable according to Polish guidelines.