
Abstract
Exit-site infections (ESIs) increase the risk of developing peritoneal dialysis (PD) peritonitis and PD technique failure. There are no clear guidelines on how to monitor exit site (ES) after ESI with Staphylococcus aureus or Pseudomonas. We report on a 1-year observational study of 23 patients who developed an ESI with one of these serious pathogens. After completing initial antibiotic treatment, swabs were taken every month for 3 months. Primary treatment cure occurred in 19/23 (83%). Colonization of ES after primary cure occurred in 8/19 (42%) patients. In the eight colonized patients, five had subsequent PD technique failure due to infections. By contrast, during an average follow-up period of 7.2 months, none of the 11 patients who were proven noncolonized developed PD technique failure from infections; HR (colonized vs. noncolonized) = 10.89, 95% CI 2.6–45.43, p < 0.05. In conclusion, colonization significantly increased the risk of catheter loss. Increased surveillance and aggressive treatment may ameliorate this risk.
Introduction
Peritoneal dialysis (PD) technique failure often occurs due to recurrent exit-site infections (ESIs) or peritonitis. 1,2
The International Society of Peritoneal Dialysis (ISPD) publishes guidelines on the management of ESI. 3 Although it suggests “repeating wound swab for bacterial culture 1 to 2 weeks after discontinuation of antibiotic has been advocated”, this is not part of ISPD guideline. We recently reported that colonization of exit site (ES) by Staphylococcus aureus or Pseudomonas (P) was associated with subsequent ESI 4 and introduced a policy to follow-up patients who developed ESI from these virulent pathogens.
We now report the outcome of this policy following patients with ESI caused by methicillin-sensitive Staphylococcus aureus (MSSA), methicillin-resistant Staphylococcus aureus (MRSA), or P. These patients had repeat swabs monthly (×3) and were followed up for long-term recurrence rate and PD technique failure.
Methods
This was an observational study between March 2019 and March 2020. All patients are taught to clean their ES every other day using sterile sachets of saline before applying mupirocin 2% ointment (supplied with their PD fluid delivery to ensure adherence).
Patients who presented with clinical signs of ESI within the study period (diagnostic criteria followed ISPD guidelines) were swabbed and started on empirical antibiotics (Intraperitoneal [IP] gentamicin and ceftazidime). Patients who had ESI prior to the study were not excluded. Patients with ESI caused by MSSA, MRSA, or P were entered in the study and antibiotic treatment was continued for 21 days (IP vancomycin for MSSA and MRSA, and IP ceftazidime for P) in keeping with ISPD guidelines. In all cases, good ES dressing technique in keeping with ISPD guidelines 5 was reinforced with retraining under nursing supervision. For the duration of antibiotic treatment, patients were asked to perform ES care daily. If infection was caused by P, mupirocin ointment (routinely prescribed for all PD patients) was changed to Naseptin™ cream and continued for the duration of the study period.
After the course of antibiotics, patients were reminded both in person and by letter to continue daily ES care using either mupirocin ointment or Naseptin cream. Patients who were infected with P were reminded to clean their shower head with bleach monthly and to run the shower water hot for 3 min before mixing with cold water to a comfortable temperature. All patients were encouraged to shower daily with dressing removed, so the ES would be cleaned during the shower although they were not to apply soap directly onto ES. Patients and family were reminded about this protocol at subsequent clinic follow-up although active monitoring of compliance was not felt to be appropriate. Prescriptions for mupirocin or Naseptin were supplied directly to patients by the PD unit.
Repeat swabs of ES were taken monthly (×3) even if there was no clinical evidence of an infection. Further antibiotic therapy was commenced only if there was a clinical diagnosis based on ISPD guidelines. Antibiotics were not started based on swab result if the clinical examination of ES was considered normal.
We report on: Clinical response: Primary cure; if no evidence of ESI within in 4 weeks of completing antibiotics. Repeat infection rate; if there was clinical evidence of ESI during the 3-month surveillance period. Colonization of ES defined if any of the surveillance ES swabs grew the putative organism without clinical evidence of infection. Long-term outcome (PD technique failure due to infection).
Chi-squared test was used to compare categorical variables and a Student’s t-test was used to compare continuous variables. The p value < 0.05 was deemed to be statistically significant. GraphPad Prism 8 (GraphPad Software Inc.) was used to perform a log rank Kaplan–Meier PD catheter survival analysis.
Results
There were 373 patients on our PD program during the 12-month study period. In total, 23 patients had an ESI growing P, MSSA, or MRSA. There were two patients who did not complete three consecutive screening ES swabs for colonization due to onset of the coronavirus (COVID-19) pandemic (it was not thought to be ethical to ask patients to break shielding to have repeat ES swabs taken of ESs that looked normal). Eighteen of the patients never had previous ESI. All patients were followed up until 1 June 2020.
Patient demographics
The mean (SD) age of patients was 59 (15) years, 60% were males, 49% were diabetic, and PD vintage was 31 (34) months. Diabetic nephropathy (40%) was the commonest cause of renal failure. There were no significant differences in demographics between the patients with ESI caused by MRSA, MSSA, or P and the full cohort (Table 1).
Baseline characteristics and demographic of patients.
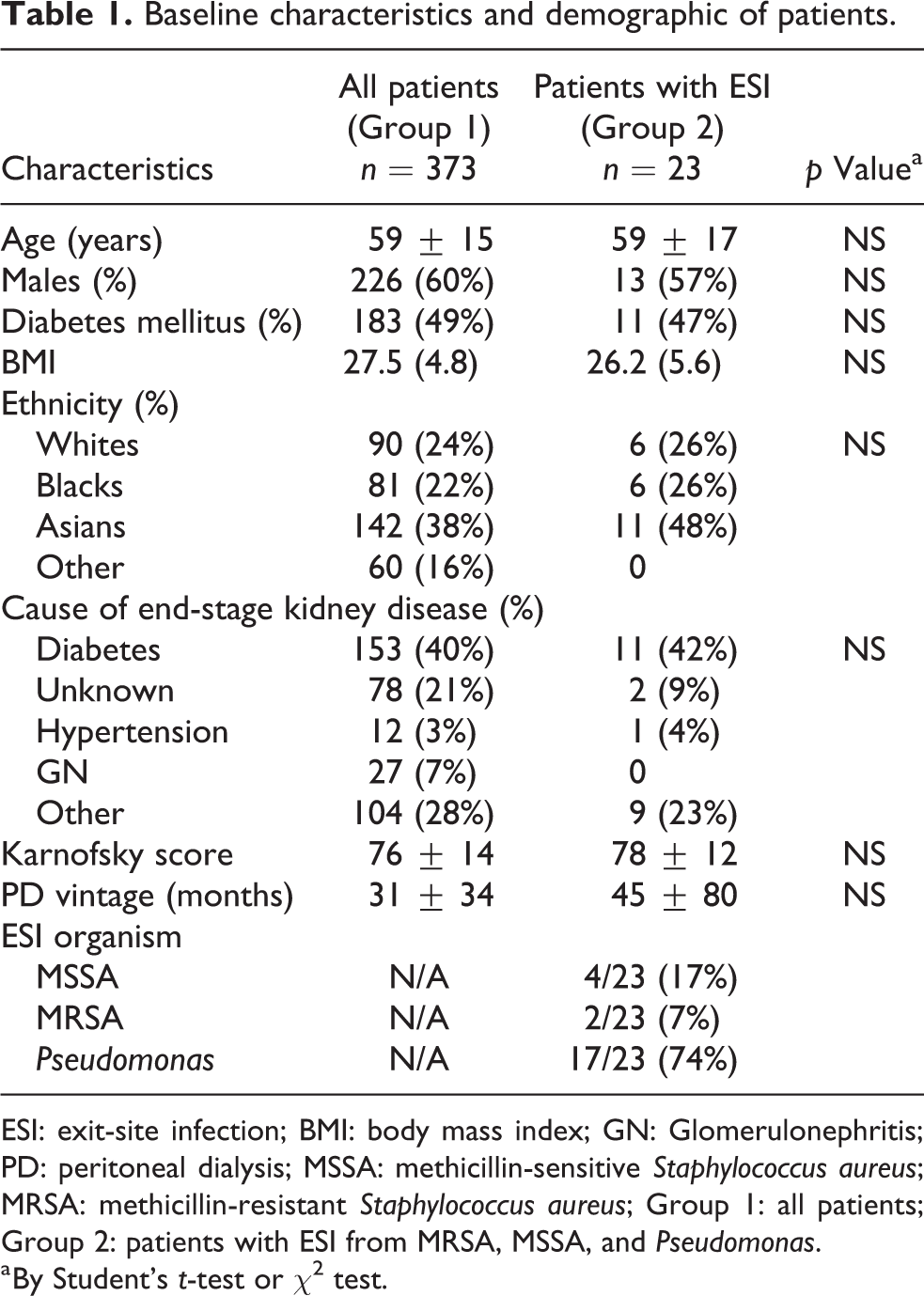
ESI: exit-site infection; BMI: body mass index; GN: Glomerulonephritis; PD: peritoneal dialysis; MSSA: methicillin-sensitive Staphylococcus aureus; MRSA: methicillin-resistant Staphylococcus aureus; Group 1: all patients; Group 2: patients with ESI from MRSA, MSSA, and Pseudomonas.
a By Student’s t-test or χ 2 test.
Outcomes
Primary cure of ESI occurred in 19 of 23 patients (83%) defined as no clinical signs of ESI was found on clinical examination within 1 month. Of the four patients who did not achieve primary cure, two patients grew Pseudomonas aeruginosa and two grew Staphylococcus aureus (MSSA). All had PD catheters removed and patients transitioned to hemodialysis (HD).
The 19 patients who had primary cure underwent surveillance screening to determine colonization and long-term follow-up to determine risk of PD technique failure from infections. Colonization was defined as growing the same organism from ES swab at least once during the surveillance period without clinical signs of infection. Mean (SD) follow-up of these patients was 6 (4) months.
We found 8/19 (42%) patients were colonized. Long-term follow-up of these eight patients revealed that five patients (three P and two MSSA) switched to HD due to infection; two patients developed PD peritonitis with associated tunnel infection while the remaining three developed a repeat ESI from the same organism which led to the decision to remove the PD catheter and switch modality to HD. Two of the eight colonized patients remained on PD and one patient was successfully transplanted.
Surveillance swabs were persistently negative in 11 patients (noncolonized). There were no PD technique failures due to infections during their follow-up although one switched to HD due to patient preference and one developed another ESI which responded to antibiotic treatment. The risk of PD technique failure due to infection was significantly increased if patients were colonized compared to those who were not colonized (HR 10.89; 95% CI 2.6–45.43, p < 0.05, Figure 1).
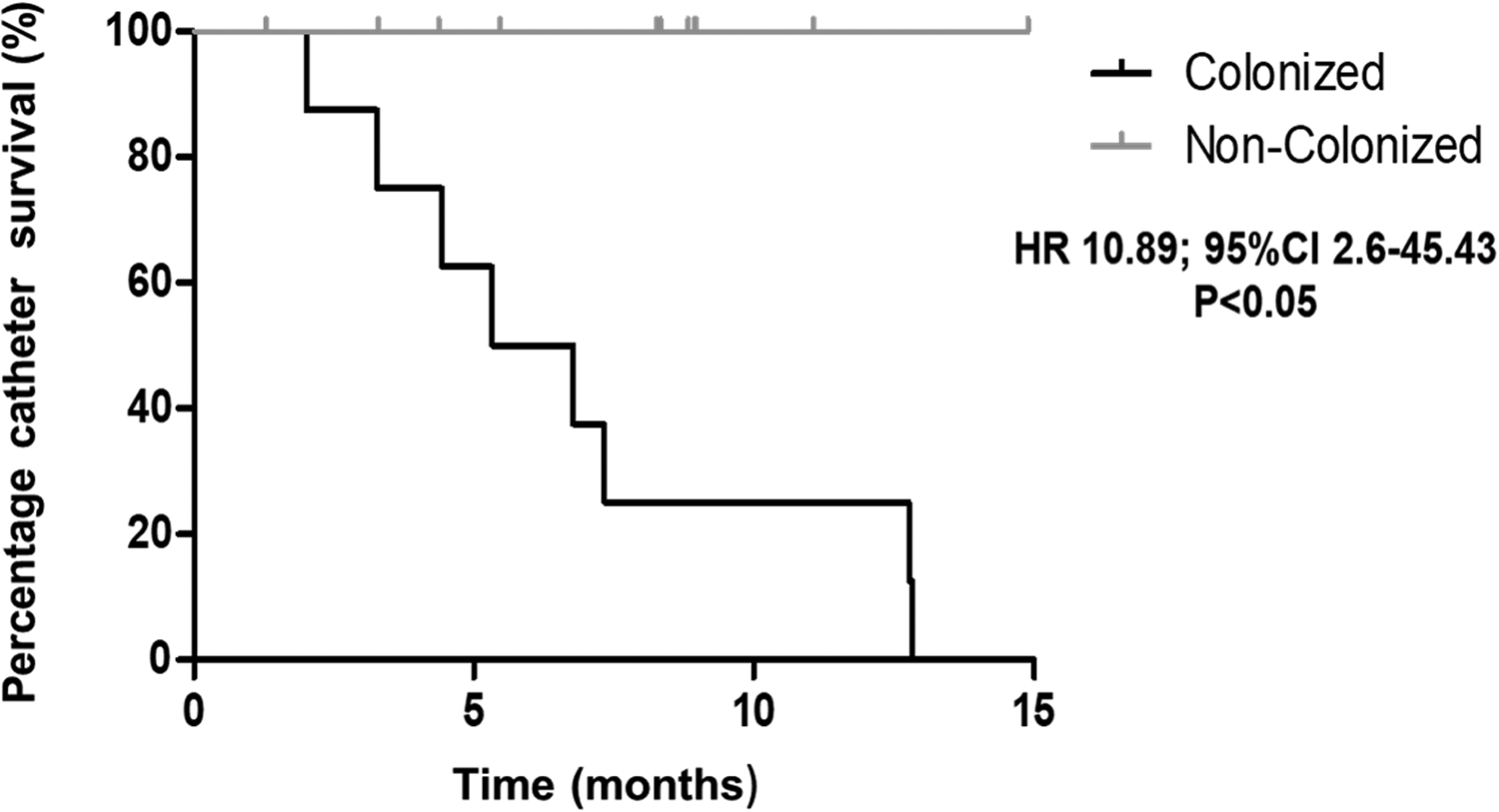
PD technique survival after ESI from Staphylococcus aureus or Pseudomonas based on patients’ colonization status. PD: peritoneal dialysis; ESI: exit-site infection; HR: hazard ratio; CI: confidence interval.
Discussion
Our results suggest that it is important to identify patients whose ES are colonized as they are at a significant risk of catheter loss. Although the value of repeat swabs after an ESI has been mentioned by ISPD, this is not currently recommended.
We showed that despite an aggressive treatment policy of treating patients with ESI from P, MSSA, or MRSA, colonization is frequent and can lead to repeat infections. It may be necessary for the PD community to consider alternative treatments that may involve more rigorous ES cleaning protocols. In common with many units, we clean ES with sterile saline but National Institute for Health and Care Excellence (NICE) recommends use of 2% chlorhexidine (CHG) in 70% alcohol to reduce rates of bacterial colonization in relation to venous and arterial catheters. Moreover, use of CE-marked devices such as Biopatch (Johnson & Johnson), 3M Tegadem CHG IV Dressing (3M Healthcare), and Algidex Ag IV Patch (deRoyal) are supported by NICE. 6 As a last resort, persistent colonization can also be treated by PD catheter exchange with creation of a new ES. Obviously such a decision should not be taken lightly and competing risk analysis is important; young patients whose transplant status may be at risk if colonization turns to tunnel infection and peritonitis may warrant a lower threshold for intervention.
Our study is small and data collection in two patients is disrupted by the COVID-19 pandemic. Nevertheless, the marked increased risk of colonization illustrated in Figure 1 supports policies to identify MRSA, MSSA, and P colonization after ESI. We also acknowledge that due to time constraints we have defined repeat infection if reinfection occurred within 3 months which is different to the 12 months proposed by Beckwith et al. 7
We chose to prescribe IP gentamicin and ceftazidime as our empiric antibiotic for ESI. This was based on the historic antibiotic resistance of organisms identified to cause ESI in our unit. We routinely used mupirocin ointment to ES (daily or alternate days according to how frequently patients preferred to bathe). We found high proportion of ESI organisms to be Gram negative (especially P) and therefore opted to empirically prescribe gentamicin and ceftazidime. Dosing of antibiotics (including IP vancomycin used for MSSA or MRSA) followed the ISPD guidelines 3 ; we confirmed in the previous study that plasma levels achieved by our dosing protocol was high. 8 We decided to use this IP protocol to minimize adherence issues. However, agree that in light of high colonization rate, perhaps identification of MRSA or MSSA may warrant introduce a second antibiotic according to sensitivity.
In summary, we have found that after primary cure of ESI from pathogenic organisms, colonization is common. These patients were at high risk of PD technique failure from recurrence of infection. We suggest that routine screening after ESI should be adopted and aggressive measures instituted if colonization confirmed.
Footnotes
Acknowledgements
None.
Author contributions
LN, MMY, and SF contributed equally. They all made a substantial contribution to the concept or design of the work, or acquisition, analysis, or interpretation of data; drafted the article or revised it critically for important intellectual content; and approved the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Not applicable.
Trial registration
Not applicable.