
Abstract

In this issue of Peritoneal Dialysis International, a multicentre randomized controlled trial from Malaysia 1 found locally made peritoneal dialysis (PD) sets containing polyvinyl chloride (PVC) had similar peritonitis rates, Kt/V, and creatinine clearance to overseas-made sets that were non-PVC. Many meta-insights are worth making in the wake of this large and well-performed trial.
Before doing so, it is worth repeating the context and rationale for the trial. In 2017, Fresenius Medical Care (Asia Pacific) opened a PD manufacturing plant in Malaysia to provide products for the region. In the process, they changed the specifications of the locally available transfer sets in Malaysia to include (1) minor differences in the dimensions of tubing without substantial modification of flow path design and (2) a change from non-PVC to PVC tubing. Both the old and new PD fluid containers were non-PVC, two-compartment in design, and the dialysis fluids bicarbonate-based. In response, the Ministry of Health in Malaysia sponsored a trial comparing the old and new sets to ensure non-inferiority of clinical effectiveness. 2 The rationale for the trial included concerns around the impact of PVC on the clinical effectiveness of PD, and the possibility of manufacturing defects arising from differences in quality control between the new local plant and the previous one in Europe.
What is the concern regarding the use of PVC? As background, PVC is a polymer of vinyl chloride, derived from mineral oil, natural gas, and salt (universal recycling symbol  ). Unplasticized PVC is hard and brittle, and used for products such as PVC pipes. To be flexible, PVC requires a plasticizer. There are around about 300 different plasticizers available with the most common being esters of phthalate (e.g. bis(2-ethylhexyl) phthalate (DEHP), diisobutyl phthalate, dibutyl phthalate, benzyl butyl phthalate). These are embedded between the chains of polymers of vinyl chloride, spacing them apart, and thus making PVC significantly softer. Up to 20–40% of flexible PVC in industrial and household devices is plasticizer by weight, and this applies to PVC-based PD sets as well.
3
–8
). Unplasticized PVC is hard and brittle, and used for products such as PVC pipes. To be flexible, PVC requires a plasticizer. There are around about 300 different plasticizers available with the most common being esters of phthalate (e.g. bis(2-ethylhexyl) phthalate (DEHP), diisobutyl phthalate, dibutyl phthalate, benzyl butyl phthalate). These are embedded between the chains of polymers of vinyl chloride, spacing them apart, and thus making PVC significantly softer. Up to 20–40% of flexible PVC in industrial and household devices is plasticizer by weight, and this applies to PVC-based PD sets as well.
3
–8
The combination of DEHP-PVC is used for the Stay•Safe® device in the study of Mak et al. However, it is also included in garden hoses, inflatable toys, and some personal-care products (shampoos, hair sprays, and nail polishes). Negligible amounts of phthalates such as DEHP are present in non-PVC plastics. The manufacturing of polyethylene (PE) and polypropylene (PP) (universal recycling symbols  /
/ and
and  , respectively) does actually require phthalates as (Ziegler–Natta) catalysts, but products only contain trace residues. For instance, coffee capsules (made of PE and PP) were reported to be 0.0003–0.0013% phthalates by weight, and water bottles (made of PE) were stored for 10 weeks 0.00003% by weight.
9
, respectively) does actually require phthalates as (Ziegler–Natta) catalysts, but products only contain trace residues. For instance, coffee capsules (made of PE and PP) were reported to be 0.0003–0.0013% phthalates by weight, and water bottles (made of PE) were stored for 10 weeks 0.00003% by weight.
9
What, then, is the health issue with DEHP-PVC? It is actually to do with the DEHP, not the PVC. A full review of the toxicology of this phthalate is out of scope for this editorial. However, it is worth noting the considerable variation in opinions about the presence and extent of toxicity. The most unbiased sources of opinion are position documents from government regulators and the reports from their commissioned scientific committees. 3,4,7,9 –13 Selected findings are reported in Online Supplemental Table S1 but can be summarized as follows. Animal studies show hepatorenal toxicity and tumour promotion above exposure levels of 3.7 mg/kg/day but with questionable interspecies relevance to humans. In vitro studies using human foetal testis tissue show no effect of DEHP on testosterone production, whereas studies using human adult testis tissue indicate that DEHP suppresses testosterone production. Clinical studies show very little in the way of toxicity, only a weak association between childhood exposure to DEHP and increased risk of allergic diseases including asthma and eczema, 14 and an association of adult exposure with decreased free testosterone levels. This latter effect is small and unlikely to be clinically significant. For instance, in those exposed to up to 100-fold higher levels of DEHP than the general population, a 13% decrease in free testosterone levels was found. 15,16
Before moving to DEHP exposure from PD sets, it is important to consider exposure from the environment. DEHP can come from a variety of sources, mainly being inhaled, eaten, and transdermally (especially from such items as plastic sandals). DEHP tends to leach from DEHP-PVC due to the loose clinical bonds to PVC. Due to its highly lipophilic nature, it is poorly soluble in water, however, achieving a maximum concentration of 25–50 µg/L in crystalloid. This can get much higher in lipid-containing fluids. For instance, the exposure to phthalates from sex toys was approximately 1000-fold greater in the presence of oil-based lubricant. 3
As given in Table 1, the largest source of DEHP exposure is from diet. Oral absorption of DEHP in humans is estimated to be (at least) 50–75%. 10,17 –19 However, the estimates in Table 1 do not adequately reflect the variation that can occur between communities and age groups (see Online Supplemental Table S2). Eating a fast-food diet is associated with higher DEHP exposure, 20 and DEHP exposure decreases importantly with age. 7 In addition, one would expect that communities with less regulated use of DEHP-PVC might also have higher risk of exposure. Perhaps, as a result of all of these factors, a recent analysis of dietary intake in urban Mexican children showed a median dietary DEHP intake of 17.42 µg/kg/day. 21 The quantification of background exposure to DEHP for any given environment must therefore account for community-specific characteristics.
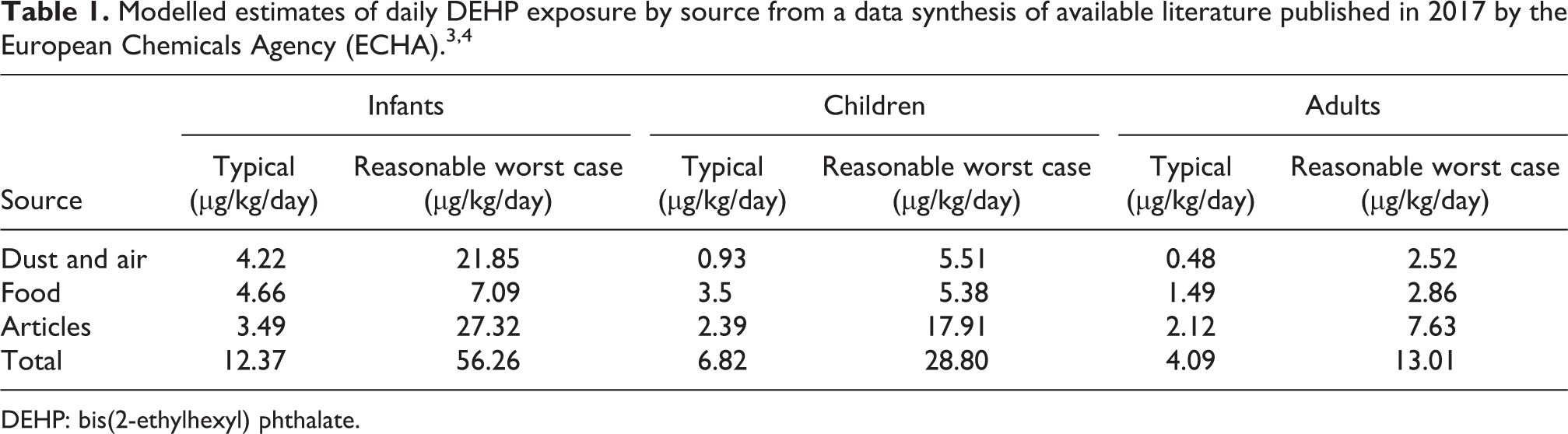
DEHP: bis(2-ethylhexyl) phthalate.
What does the literature tell us about DEHP exposure in PD? Once absorbed, DEHP is rapidly metabolized to non-toxic conjugates, which are then exerted in urine and bile. 10 Given this situation, the assessment of toxicity from DEHP in PD is a simple exercise of comparing the contribution from PD devices to a patient’s total DEHP exposure. There are several helpful studies in the literature, and they are summarized in Table 2. It has been known for some time from animal models that the majority of an intraperitoneally injected DEHP is not absorbed, 22 and it can be seen from these studies that a considerable amount of infused DEHP is returned upon drainage. Even the ‘realistic’ calculated DEHP exposure in Table 2 is therefore likely to be an overestimate. This explains the results of Mettang et al, 23 who studied five patients as they changed from a plasticizer-containing PVC PD system (A.N.D.Y. Plus®, Fresenius Medical Care, Bad Homburg, Germany) to a polyolefin-made plasticizer-free system from the same manufacturer (Stay•Safe®). Surprisingly (at the time), there was no significant change in serum DEHP concentrations in blood or spent dialysate between baseline (PVC) and 42 days (non-PVC) (Figure 1). This likely reflects the small contribution of PD fluids to DEHP burden, relative to background exposure. Overall then, it can be concluded that exposure to DEHP through PD is low, and several log orders less that required for any of the toxicity described earlier.
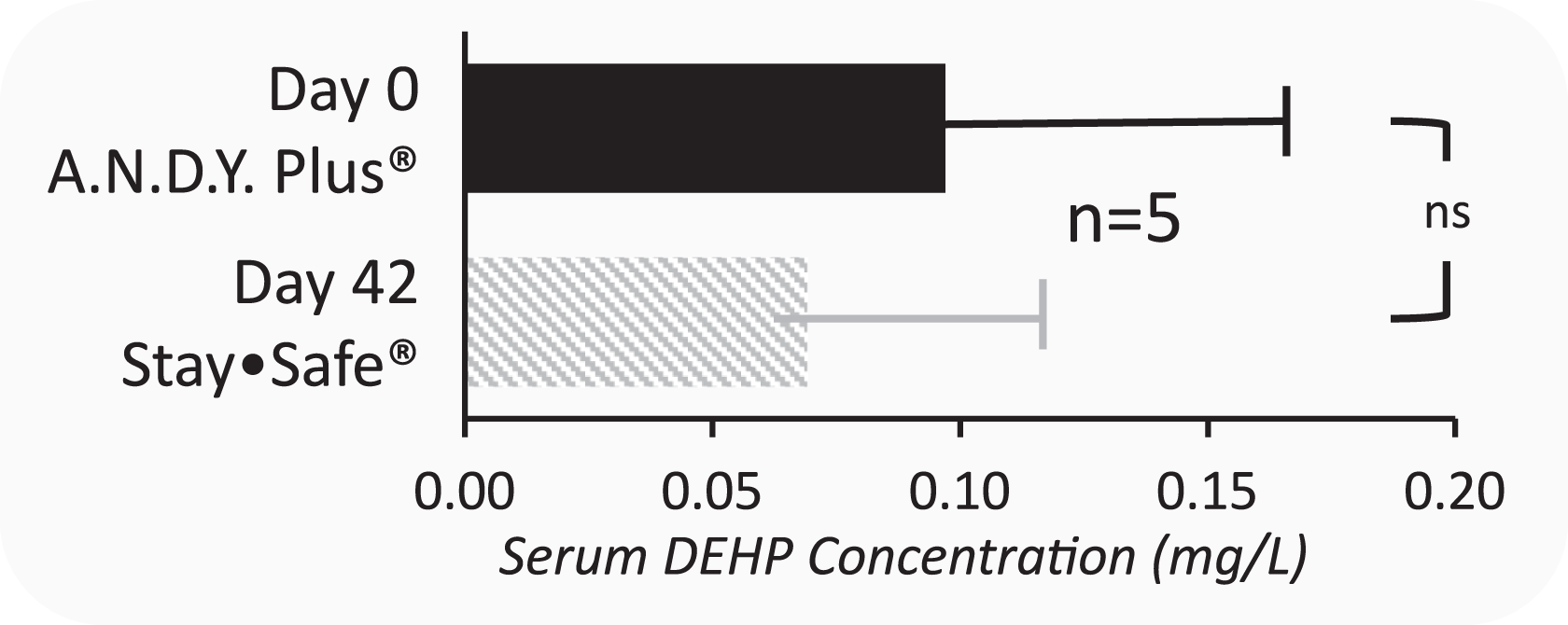
Comparison of serum DEHP levels between polyvinyl chloride and non-polyvinyl chloride peritoneal dialysis sets. 23 DEHP: bis(2-ethylhexyl) phthalate.
Available estimates of daily DEHP exposure from peritoneal dialysis.
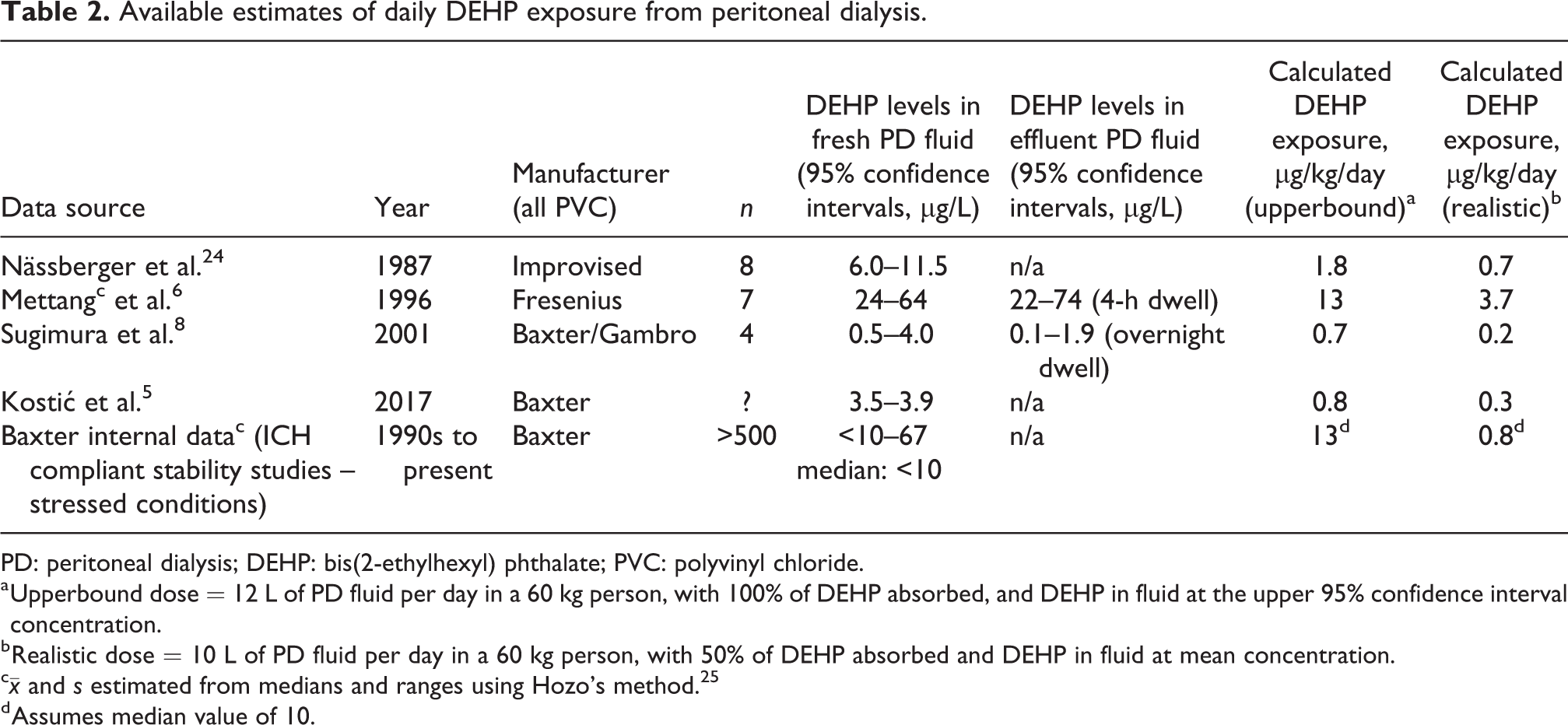
PD: peritoneal dialysis; DEHP: bis(2-ethylhexyl) phthalate; PVC: polyvinyl chloride.
a Upperbound dose = 12 L of PD fluid per day in a 60 kg person, with 100% of DEHP absorbed, and DEHP in fluid at the upper 95% confidence interval concentration.
b Realistic dose = 10 L of PD fluid per day in a 60 kg person, with 50% of DEHP absorbed and DEHP in fluid at mean concentration.
c
d Assumes median value of 10.
Previous to Mak et al., there had been only a handful of studies to clinical outcomes between PVC and non-PVC PD dialysis products. Most recently, there have been two large randomized controlled trials in China that have compared Baxter (PVC) PD sets with locally manufactured non-PVC products: Changfu (Changzen Fumin Jinshan, Shanghai, China) and Huaren (Qingdao Huaren Pharmaceutical Co., Ltd, Qingdao, China) PD sets. 26,27,28 In these medium- to long-term studies, there was no signal or even hint of clinical benefit with the non-PVC products, although an effect may have been obscured by an impressively higher incidence of infectious complications with both local Chinese products, especially in the early phases of the trials. In terms of local effects, it has been postulated that DEHP is directly harmful to the peritoneal membrane. However, these hypotheses have been hard to test, and available animal studies have debatable relevance to the clinical situation: DEHP often used “neat” with concentrations showing effects at >1000–20,000 times that in PD solutions, with confounding via significant interspecies differences in metabolism and toxicity. 29,30
Given the reassuring study from Mak et al., the issue of PVC in PD seems a ‘non-issue’, at least from a clinical perspective. It is unsurprising, then, that every regulatory report that has addressed the issue of PVC in PD products has identified little or no risk (of concern). 10 –12 Admittedly, there are other issues at play such as the increasing regulatory hostility to DEHP-PVC, driven by a focus on the environment. This is an important issue in itself, given that medical waste in general contributes around 3% of total societal PVC waste – certainly non-PVC PD sets are a socially responsible initiative. However, there are other ways of handling PVC waste from PD device sets. For example, in Australia, all of these sorts of sets are retrieved and up/downcycled at the manufacturer’s cost.
So, why might the development of well-intentioned non-PVC products have potential to hinder rather than help? Escalation of costs. Non-PVC PD products are several folds more expensive to manufacture than PVC products and naturally are sold at a higher price. However, there is no reason for corresponding manufacturers of PVC products to sell at a much lower price than their competitors. The upshot is that non-PVC PD products increase the selling price of all PD products, including those made of PVC. In this age of cost constraints, it seems unreasonable to have more expensive PD products with little or no clinical benefit. This is particularly relevant for low- and middle-income countries, where it is critical to maximize the availability of dialysis within a small envelope of funds. From a broader perspective, there is also an opportunity cost from high costs of dialysis in general, insofar as there is less to spend on other pressing medical needs, even within the nephrology discipline. Deprioritization of device development for important outcomes. Unlike ‘Big Pharma’, device manufacturers are generally constrained in research and development (R&D) spending due to the high costs of manufacturing. So, what areas of research should the industry be spending their sparse resources on? Mak et al. chose an important primary outcome of PD-related peritonitis. It is the very top patient-centered priority for care
31,32
and also a leading modifiable cause of therapy-related death.
33
–37
Despite improvements in PD peritonitis rates over the last few decades,
16
it can be argued that the majority of research investment should arguably still focus on modifications to existing flow path design and connectology, which are literally decades old.
38
–40
It would behoove the PD community to revisit the issue PD connection-assist and sterilizing devices, implementing improvements that might actually make a meaningful difference to patients’ lives. A first step is suggested by a recent scoping systematic review by industry, where the relative risk for peritonitis with external clamp systems was 0.52 (0.44, 0.81) relative to disc systems.
41
Further studies may very well confirm that certain PD devices have benefit in terms of clinical outcomes compared to others and is critically important information. These studies are lacking and would provide the impetus for manufacturers to prioritize their resources to more clinically appropriate areas.
One might be tempted to relegate the issue of PD fluid containers to history, in view of ‘bagless systems’ that might seem to be on the horizon. These include various systems over 50 years that have utilized PD fluid generated from reverse osmosis units 42 –45 and also more recent systems that utilize regenerated PD fluid through the use of sorbents. 46 –49 In general, however, these innovations have been difficult to bring to market in a cost-effective manner. For the next few year (at least!) fluid containers are going to be the standard of care for PD, and the issue of materials and their adverse effects an ongoing concern.
In general, PD is under-researched. Figure 2 is a little out of date but still spells a compelling call for action. It is important for us all to remember that many (or even most) major advances in PD devices have not come through industry but through the innovation and ingenuity of healthcare workers and researchers. The Y-set, 50 –53,51,52,54 flush before fill connectology 55,56 and icodextrin 57 –59 are all examples of ‘game changers’ brought to light from independent scientists and clinicians, before being handed to industry for large-scale manufacture. It is timely to remind ourselves that improving PD devices is far from being the sole provenance of industry R&D, which at this current time is more focused on quality manufacturing, rather than basic product innovation. History shows us that true technical innovation in PD will always originate from the coal face in response to unmet needs.
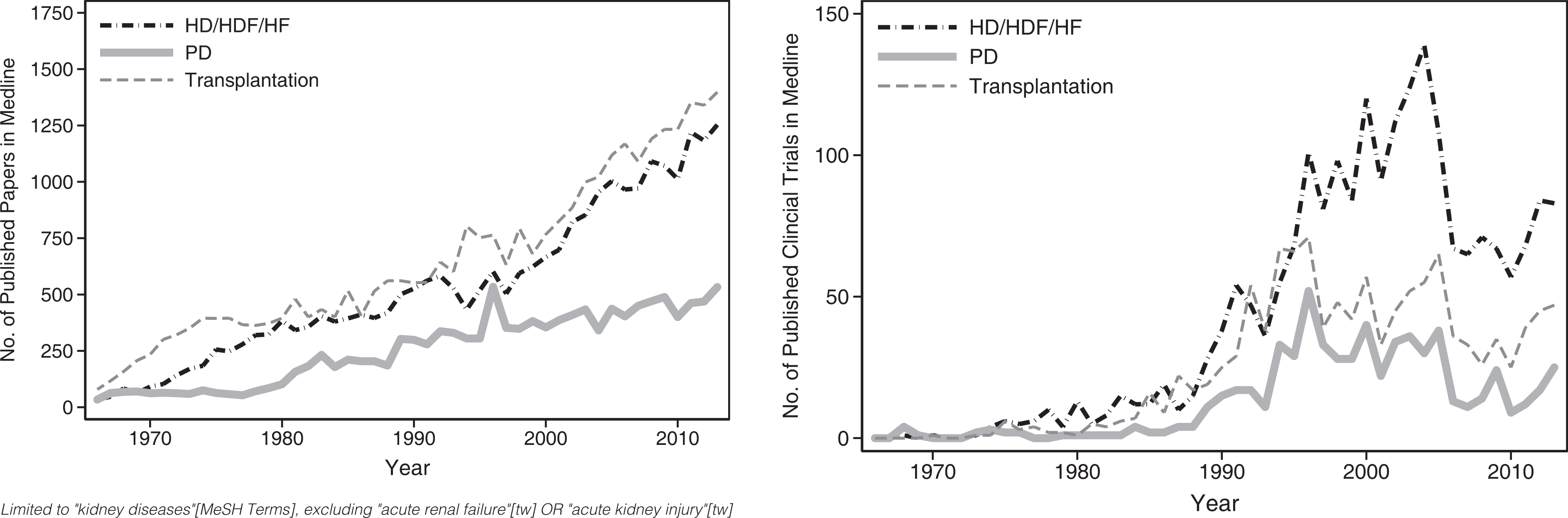
Research output on Medline as of 2016 by kidney replacement therapy modality.
For now, Mak et al. are to be congratulated once again. Their trial focuses on a key question of which device is best, implemented in a study free of industry influence, focusing on what is arguably the most important outcome in PD. It can only be hoped that their spirit of inquiry is infectious.
Supplemental material
Supplemental Material, sj-docx-1-ptd-10.1177_08968608211001262 - Non-polyvinyl chloride peritoneal dialysis sets: A double-edged sword?
Supplemental Material, sj-docx-1-ptd-10.1177_08968608211001262 for Non-polyvinyl chloride peritoneal dialysis sets: A double-edged sword? by Mark Roger Marshall in Peritoneal Dialysis International
Footnotes
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.