
Abstract
Background:
Peritoneal dialysis catheter (PDC)-related infections account for significant morbidity, PD disruptions and costs. Patients with refractory exit-site or tunnel track infections without peritonitis may need catheter removal and reinsertion which can be complicated by bleeding, organ injury, catheter failure or malposition. Some patients may need to switch to haemodialysis in such a setting. An alternative is a salvage procedure. The purpose of this systematic review is to evaluate the safety and efficacy of salvage techniques.
Methods:
A comprehensive search of PubMed, Medline and Scopus databases was performed from inception to December 2021 in accordance with PRISMA guidelines. After a broad search, articles were stratified into two main categories for assessment: (1) cuff-shaving (CS) techniques and its variations of en-bloc resection (BR) and/or catheter diversion (CD) and (2) partial reimplantation with CD.
Results:
A total of 409 patients (445 salvage procedures) from 20 studies were included in analysis. Of 409 patients, 234 patients (57.2%) underwent 251 (56.4%) CS procedures and its variations, 163 patients (39.9%) underwent 182 (40.9%) partial PDC reimplantations with CD and 12 patients (2.7%) underwent local curettage. Overall PDC salvage rate after intervention was 73.2%. Overall PDC removal rate attributable to infection was 26.8%. Overall complication rate attributable to the procedures was 2.7%, with the most common complication being dialysate leakage (n = 10) followed by PDC laceration (n = 1) and subcutaneous haematoma (n = 1). We also included a description of our technique of BR of infected tissue, CS and CD. In a series of six patients, the PDC salvage rate was 83.3% and median PDC survival after intervention was 10 months.
Conclusion:
PDC salvage techniques are relatively safe and provide reasonable catheter salvage rates in selected patients. Results of this review should lend weight to consideration of a salvage-first approach as an option in selected patients.
Introduction
Peritoneal dialysis (PD) is a popular mode of renal replacement therapy but peritoneal dialysis catheter-related (PDC) infections can cause significant morbidity and lead to its inevitable cessation. Catheter-related infections is the Achilles heel of this mode of dialysis and accounts for an overwhelming majority of late complications and catheter removal. 1
According to the International Society for Peritoneal Dialysis (ISPD) 2017 update, 2 exit-site infection (ESI) is defined as the presence of purulent discharge, with or without erythema of the skin at the catheter–epidermal interface. 2 Tunnel infection (TI) is defined as the presence of clinical inflammation or ultrasonographic evidence of collection along the catheter tunnel. 2 Refractory ESI or TI is defined as failure to respond after 3 weeks of effective antibiotic therapy. 2
In the latest ISPD guidelines – 2019 update, 3 the initial treatment for all PDC-related infections is usually culture-directed antibiotics. In the setting of clinical or ultrasonographic evidence of TI with fluid around the deep cuff or concurrent peritonitis, the recommendation is catheter removal, interim haemodialysis and staged reinsertion of the PDC. 3 On the other hand, for ESI and TI without peritonitis or abscess involvement of the inner cuff (for PDCs with a dual-cuff design), a variety of procedures have been described for PDC salvage.
Cuff-shaving (CS) of the external cuff was first described by Nichols in 1983. 4 Variations of this technique include addition of en-bloc resection (BR) of the skin and tissues around the peripheral cuff 5 –7 as well as catheter diversion (CD) via a new subcutaneous tunnel. 8,9
Partial reimplantation (PR) and CD of the PDC using the splicing technique was first described by Roman in 1984 for the main indication of external cuff extrusion. 10 It involved transection of the PDC between two cuffs, removal of the external segment, followed by connection of the remnant PDC to a new external segment using a ridged connector. The new external segment was then diverted via a new subcutaneous tunnel.
ISPD guidelines 3 suggests PR with CD to a more satisfactory exit-site location when ultrasonography shows absence of fluid around the superficial cuff and if the location of the exit-site was a contributing factor to the chronic infection. CS or simultaneous catheter replacement is recommended for clinical or ultrasonographic findings of TI with fluid around the superficial cuff and the intercuff tubing segment.
These procedures have had varying successes in terms of the overall catheter lifespan – defined as duration from attempted salvage to eventual removal of the PDC. However, in the hands of surgeons who are either unaware or unfamiliar with these salvage techniques, upfront catheter removal is commonly favoured over a salvage-first approach.
To date, there is no systematic review of the various salvage techniques and their outcomes. The primary aim of this review is to characterise the safety and efficacy of a salvage-first approach and various salvage techniques in the setting of ESI/TI. We further subcategorise these techniques by the components involved.
The authors also describe the technique used in their institution of BR of infected tissue, CS and CD and present the results from a series of six patients.
Methods
We conducted a comprehensive literature search using electronic databases (PubMed, MEDLINE, Scopus) with no language restrictions, from inception through December 2021. For the search strategy, combinations of the following keywords and MeSH terms were used: PDC, Tenckhoff catheter, catheter-related infection, ESI, TI, cellulitis, salvage, exit-site renewal, CS, diversion, replantation. The search strategy is provided in Appendix 1.
Studies were included for analysis if they used any salvage technique for ESI/TI and reported at least one outcome of catheter survival, perioperative mortality, morbidity. Small studies or case reports with five or fewer patients were excluded. Patients in whom salvage techniques were employed for non-infectious indications were excluded from analysis.
Relevant titles were selected from the first screening and abstracts of citations were reviewed independently by two reviewers (JJYS and NZPN) to identify all potentially relevant articles. Abstracts without associated full texts were excluded from the final analysis. Articles were cross-referenced for additional relevant studies. The reference lists of the relevant original and review articles were searched for additional reports. Full-text articles were retrieved for further consideration for inclusion. In cases of disagreement, the senior author (SQWL) was consulted.
The methodological quality of the studies was assessed independently by the two same authors using the Joanna Briggs Institute (JBI) tool for case series 11 and Newcastle-Ottawa Quality Assessment Scale for comparative studies. 12 Publication bias was considered high since all the included studies were either case series, case–control or cohort studies in design and were small in sample size. The quality of this review was validated using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) tool. 13
The following information was extracted from the included studies: author name, year of publication, country, study design, sample size, salvage technique used, overall catheter survival outcomes, persistent/recurrent infection outcomes, complications, perioperative mortality and morbidity. Where available, data on PDC removal due to recurrent or persistent infection were obtained or extrapolated. Not all studies reported on all assessed variables. Studies that did not report on a specific outcome were recorded as non-reported (NR).
Due to the lack of studies with a design that would allow us to perform a meta-analysis, as well as the heterogeneity of included studies, we opted to perform a narrative synthesis using the Synthesis Without Meta-analysis (SWiM) reporting guideline. 14
The included studies were grouped into two major categories for analysis based on the components involved in the salvage technique: (1) CS with varying combinations of BR of infected tissue and/or CD and (2) PR with CD. One study that did not fall into either category was described separately. Data were summarised using descriptive statistics, with means and standard deviations for continuous variables and frequencies and percentages for dichotomous variables where appropriate and available.
The outcomes from a series of six patients who underwent CS with BR and CD for chronic ESI/TI at our institution from January 2020 to June 2021 were collected prospectively. Data collected includes demographic data, overall duration of PD, causative organism, antibiotic therapy and PDC survival after intervention.
Authors’ technique
The authors’ preferred technique is to perform BR of infected tissue, CS and CD. Eligible patients with refractory ESI and TI undergo preoperative ultrasonography to identify abscesses and collections along the tunnel. If abscess formation involved the internal cuff or if there was PD-associated peritonitis, catheter removal was offered instead.
Intravenous antibiotics were given prior to skin incision. The abdomen is cleaned with povidone-iodine and draped with sterile covers. The external portion of the catheter is then soaked in a gallipot of povidone-iodine while dismantling its components, which includes detaching the transfer set and the catheter adapter.
The steps of the procedure are illustrated in Figure 1. Firstly, an elliptical incision is made around the exit-site with an extension in the direction of the underlying tunnel collections (Figure 1(a);). A cylinder of tissue around the catheter is then excised en-bloc and then freed from the catheter (Figure 1(b); and (c)). It is sent for the relevant cultures and microbiological investigations. The exposed external cuff is then shaved using a sharp blade (Figure 1(d)), taking care not to damage the catheter as that would then result in the need to remove or exchange the catheter. The catheter is then tunnelled subcutaneously to exit through a separate exit-site with the external cuff intentionally left exposed (Figure 1(e)). The cavity in the anterior abdominal wall can then be closed primarily (Figure 1(f)) or allowed to heal by secondary intention depending on the degree of contamination identified intraoperatively.
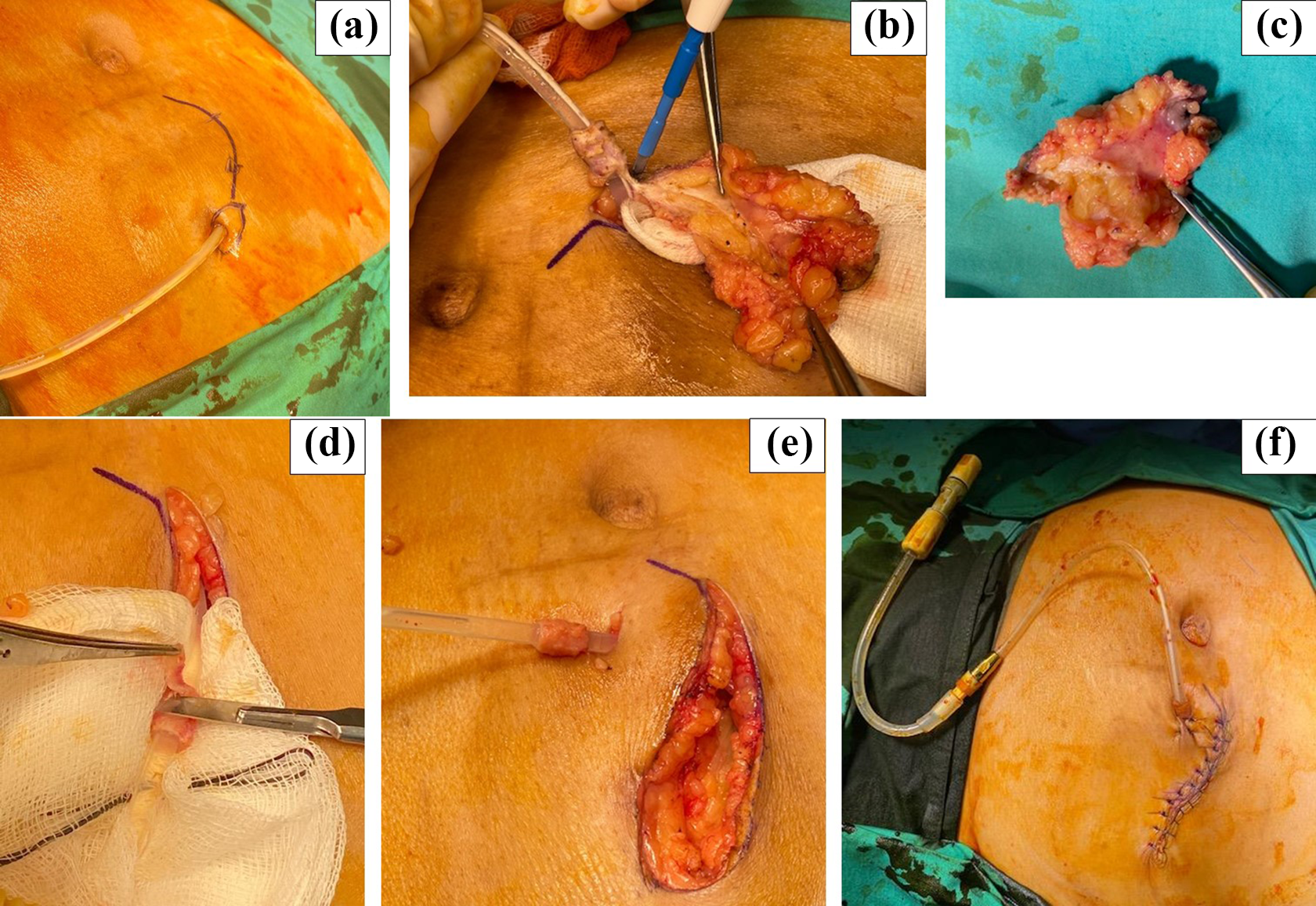
Steps of the procedure: (a) Skin marking around the external portion of a PDC demonstrating the intended incision; (b) cylinder of infected tissue around the catheter and cuff is being removed; (c) excised cylinder of tissue; (d) external cuff is shaved with a sharp blade; (e) subcutaneous diversion of the external portion of the PDC; (f) closure of the wound and the final result after the salvage procedure.
Results
A total of 54 unique citations were initially retrieved, of which 28 were reviewed in full. Twenty articles met inclusion criteria and were included in final analysis (Figure 2).
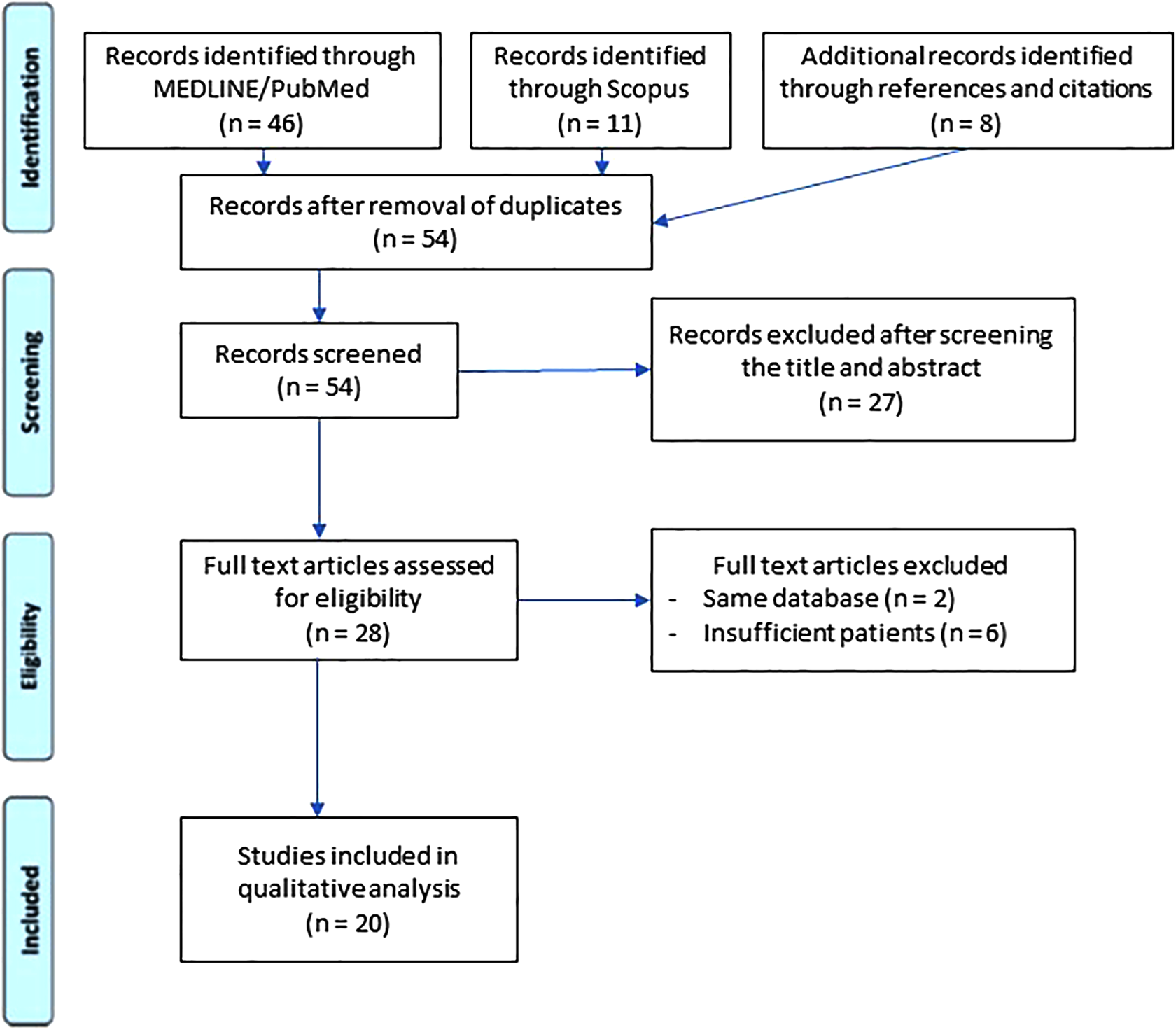
PRISMA flowchart.
Quality appraisal
The overall quality of evidence of the 14 included case series was low, by virtue of study design. Most series had clear patient selection criteria, with clear reporting of clinical information and outcomes pertaining to persistent and reinfection rates. However, the follow-up period was highly variable (range 3–37 months) and was not reported in all studies. This has repercussions on the interpretation of the reported catheter survival rate, median catheter survival time and infection recurrence rates (which was reported in most but not all studies).
Only six comparative (four case–control, two cohort) studies met inclusion criteria and the overall quality of these studies was poor to fair in quality. Cases and controls were matched appropriately in case–control studies. Appropriate statistical analyses were employed. However, most studies did not consider or attempt any strategies to identify or deal with potential confounders, which was potentially difficult in view of the relatively small sample sizes in the studies.
Overall results
From the included studies, a total of 409 patients underwent 445 salvage procedures for ESI/TI. Among whom, 234 (57.2%) patients underwent 251 (56.4%) CS procedures and its variations, 163 (39.9%) patients underwent 182 (40.9%) partial PDC reimplantations with CD, while the remaining 12 (2.7%) patients each underwent local curettage. In the included articles, there were some patients who had more than one PDC insertion, hence the discrepancy in the number of patients and procedures.
Overall PDC removal rate attributable to infection was 26.8%. Overall persistent/recurrent infection rate was 31.5% with 88 episodes of ESI/TI and 52 episodes of peritonitis. Rates of persistent/recurrent infection exceed the catheter removal rate because some infectious episodes were resolved without PDC removal. Overall complication rate attributable to the procedure was 2.7%, with the most common complication being dialysate leakage (n = 10) followed by PDC laceration (n = 1) and subcutaneous hematoma (n = 1). No perioperative mortality was reported by any of the studies. Overall results are summarised in Table 1.
Overall results.
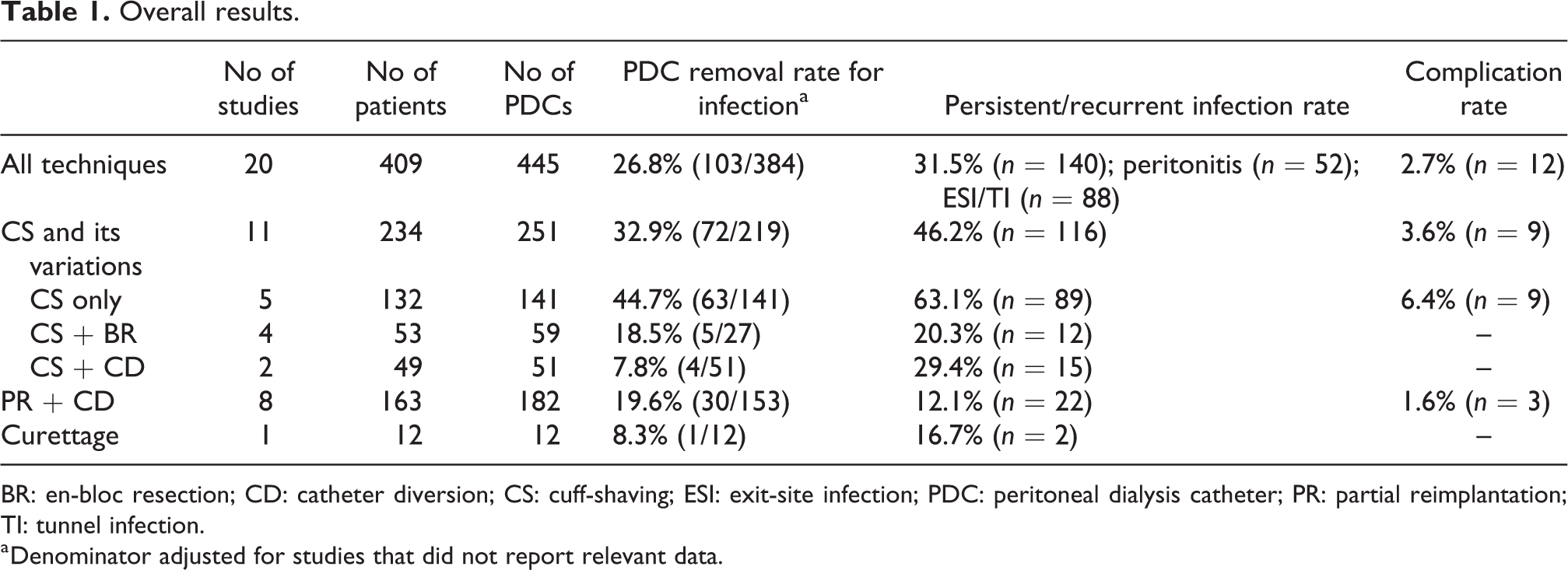
BR: en-bloc resection; CD: catheter diversion; CS: cuff-shaving; ESI: exit-site infection; PDC: peritoneal dialysis catheter; PR: partial reimplantation; TI: tunnel infection.
a Denominator adjusted for studies that did not report relevant data.
Median catheter survival rates were only reported or reached in eight studies, and varied between 1.5 months and 84 months. The results should be interpreted with caution due to the wide variation in length of follow-up between studies and the lack of uniformity of definitions used between studies. The results are summarised in Tables 2 to 4.
Studies describing CS with varying combinations of BR or CD.
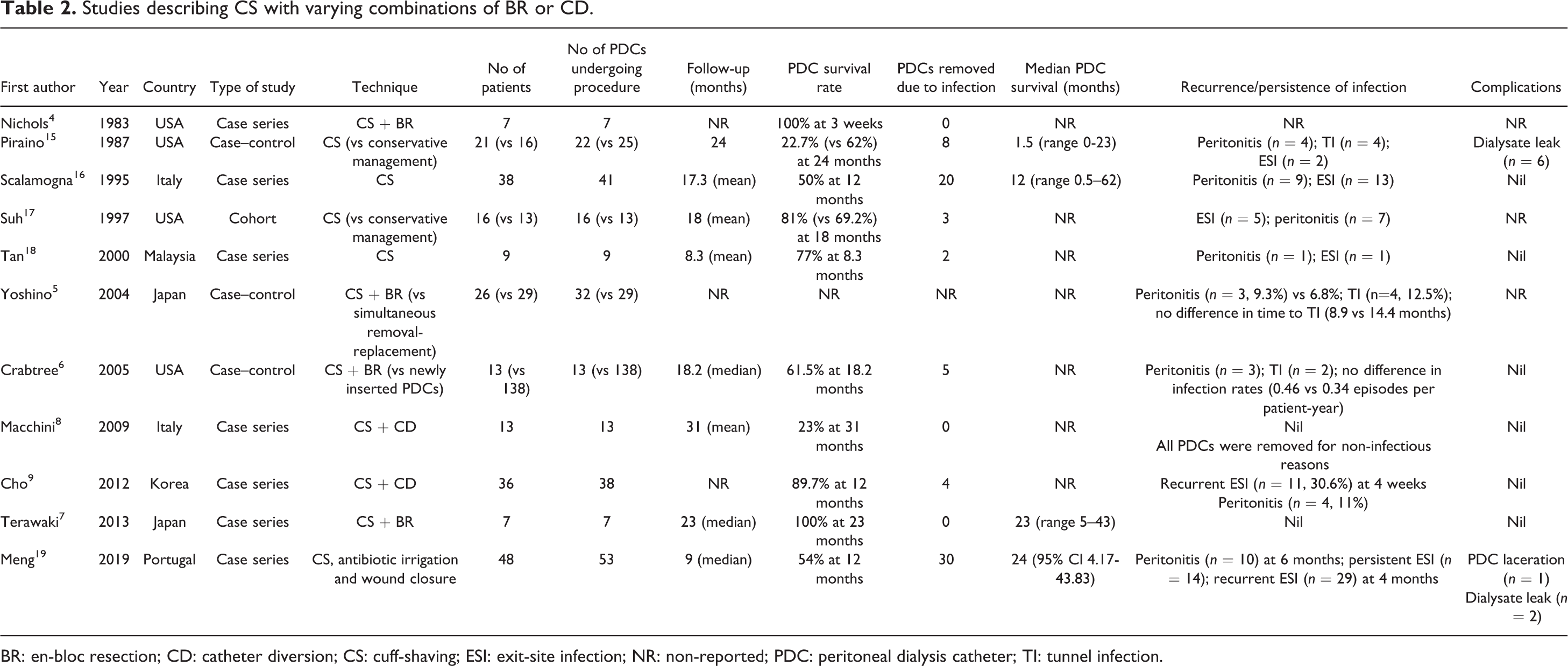
BR: en-bloc resection; CD: catheter diversion; CS: cuff-shaving; ESI: exit-site infection; NR: non-reported; PDC: peritoneal dialysis catheter; TI: tunnel infection.
Studies describing PR with CD.
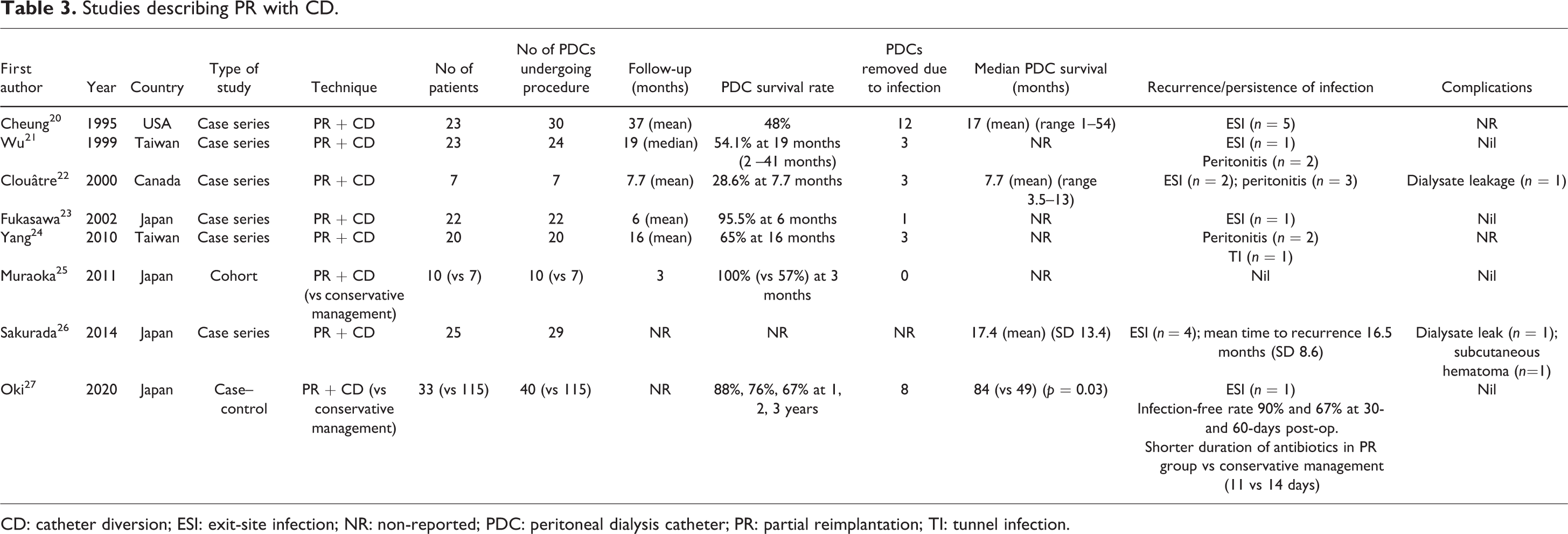
CD: catheter diversion; ESI: exit-site infection; NR: non-reported; PDC: peritoneal dialysis catheter; PR: partial reimplantation; TI: tunnel infection.
Studies describing local curettage procedure.

ESI: exit-site infection; NR: non-reported; PDC: peritoneal dialysis catheter.
CS with or without BR or CD
There were 11 (7 case series, 3 case–control, 1 cohort) studies that described their experience with CS and varying combinations of BR or CD. Data for eventual PDC removal due to infection were not available in one study. Overall, 72 of 219 (32.9%) PDCs were removed due to recurrent or persistent infection after CS and its variations. Subgroup analysis showed catheter removal rates of 7.8% (4/51) for CS + CD, 18.5% (5/27) for CS + BR and 44.6% (63/141) for CS alone. Rates of persistent and recurrent infection were 46.2% overall, 29.4% for CS + CD, 20.3% for CS + BR and 63.1% for CS alone. There were eight cases of dialysate leakage after CS and one case of a lacerated PDC which required removal. The results are summarised in Table 2.
Partial reimplantation with catheter diversion (PR+CD)
There were eight (six case series, one case–control, one cohort) studies that described their experience with PR + CD. Data for eventual PDC removal due to infection were not available in one study. Overall, 30 of 153 (19.6%) of PDCs were removed due to recurrent or persistent infection after attempted salvage with PR + CD. Rates of persistent and recurrent infection were 12.1%. There were two cases of dialysate leakage and a case of subcutaneous hematoma after PR + CD. The results are summarised in Table 3.
Curettage only
There was a case series 28 of 12 patients who underwent exit-site curettage for attempted salvage. PDC survival rate was 83% and 1 PDC was removed due to infection at the end of the follow-up period which ranged from 12 months to 24 months. The results are included in Table 4 and this review for completeness.
Outcomes of authors’ technique
The results from this procedure have been encouraging in our institution. In a series of six patients who underwent the described procedure at our institution from January 2020 to June 2021, only one patient (16.7%) required removal of the PDC at 12 months due to PD-peritonitis from a different causative organism. This translates into an 83.3% PDC salvage rate. At the end of the follow-up period (December 2021), PDC survival after salvage ranged from 4 months to 16 months, with a median PDC survival of 10 months. The characteristics and outcomes of the patients are summarised in Table 5.
Profile of the patients who underwent the described procedure at the authors’ institution.
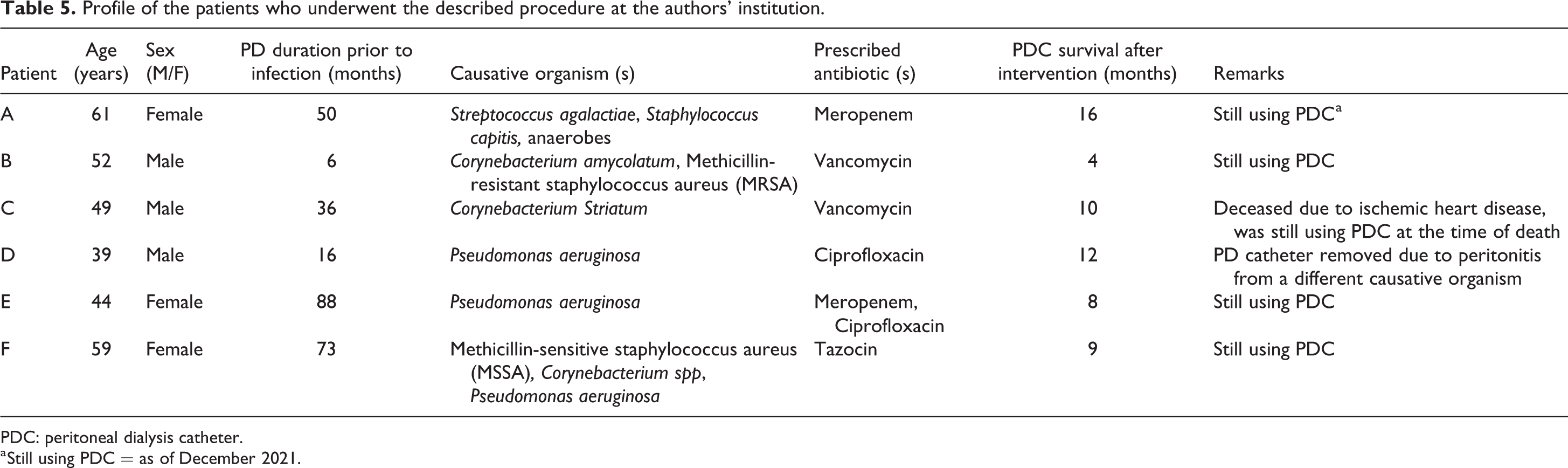
PDC: peritoneal dialysis catheter.
a Still using PDC = as of December 2021.
Discussion
This review assesses the efficacy and safety of the two main salvage techniques employed for PDCs with refractory ESI/TI. While the efficacy of each technique is highly variable between studies with an overall PDC removal rate 26.8% (103 of 384), the techniques are safe with procedure-related complication rates at 2.7% (n = 12).
To provide a meaningful outcome for comparison of efficacy across studies, we defined the PDC removal rate as the proportion of salvaged PDCs removed due to refractory or recurrent infection (if the information was available in the included studies), because PDCs could be removed for non-infectious reasons (mechanical failure, conversion to hemodialysis, transplantation). Nevertheless, there were huge variations in length of follow-up and hence PDC survival between studies. The heterogeneity in terms of reported outcomes, length of follow-up and the relatively lack of comparative studies means that the data were ultimately not amenable to meta-analysis.
Cuff-shaving
Three comparative studies suggest that CS is effective without significant morbidity. Suh et al. 17 demonstrated the superiority of CS over conservative management in terms of incidence of peritonitis and recurrent ESI/TI. Yoshino et al. 5 found no difference in terms of incidence of recurrent ESI/TI or peritonitis between patients who underwent CS + BR compared to simultaneous PDC removal and replacement for ESI/TI. While Crabtree et al. 6 found no difference in the infection rate between patients who underwent CS + BR for ESI/TI compared with a cohort of patients who had newly inserted PDCs (control group). Only one comparative study 15 demonstrated worse outcomes with CS but the results were confounded by a high rate of early technical failure – 6 of 22 PDCs were removed due to dialysate leakage at the end of the procedure – which was absent in other studies.
CS alone appeared to be less efficacious than CS combined with BR or with CD. CS removes the biofilm and planktonic organisms that colonise the Dacron material of the external cuff and addition of BR of infected tissues around the cuff ensures further reduces bacterial burden. CD via a new sterile subcutaneous tunnel theoretically decreases the risk of recolonisation. For these reasons, the authors’ preferred technique is a combination of all the above components.
One of the rare complications noted in this review is dialysate leakage. Sharp dissection of the cuff could result in PDC laceration. CS converts the PDC from a two- to single-cuff design which may increase the risk of dialysate leakage as the PDC now only relies on the deep cuff for support. The risk of leakage is higher if the deep cuff was implanted in the subcutaneous tissues or midline linea alba as the lack of stability of the cuff in these positions would predispose to leak over time. However, if the deep cuff was implanted within the rectus muscle and sheath, the shaving of the superficial cuff would not be expected to increase the risk of leak. The reported incidence of dialysate leakage was low in this review, demonstrating that it is safe if meticulous technique during CS is observed.
Partial reimplantation and catheter diversion
PR and CS were comparable in terms of efficacy and safety. Two comparative studies were in favour of PR + CD compared with conservative management. Muraoka et al. 25 reported a 100% PDC survival rate at 3 months with PR + CD compared with 57% in the conservative management group. Oki et al. 27 reported PDC survival rates of 88%, 76%, 67% at 1, 2 and 3 years, respectively, among the 40 PDCs that underwent PR + CD. Median PDC survival in the PR + CD group was longer (84 vs 49 months) than in the conservative management group. Infection-free rate was 90% and 67% at 30- and 60-days post-operatively and there was also a shorter duration of antibiotics in the PR group versus conservative management (11 vs 14 days).
The benefit of PR is the longer distance from the inner cuff to the new external opening (as compared to after CS). The procedure is also repeatable with recurrent episodes of refractory ESI/TI. The key disadvantage of this technique is the need for splicing of the catheter and the use of a connector which may have a steeper learning curve, lend itself to risk of dialysate leakage and reinfection. Connectors may vary in their propensity for bacterial recolonisation depending on the material used, for example, Teflon, glue and titanium. Notably, connectors other than titanium are not approved for implantation within body tissues in some countries.
Implications on societal guidelines
The ISPD Guidelines (2019 update)
3
outline the recommendations for chronic ESI/TI: – PR with CD if there is no fluid around the superficial cuff and the location of the exit site was a contributing factor to the chronic ESI (GRADE 2C) – CS or simultaneous catheter replacement if there is TI with fluid around the superficial cuff and the intercuff tubing segment (GRADE 1C) – Catheter removal, interim haemodialysis and staged reinsertion of PDC if there is TI with fluid around the deep cuff or concurrent peritonitis (GRADE 1B)
This review finds that CS and PR are both safe and effective salvage techniques in the management of chronic ESI/TI, concordant with guideline recommendations. However, in institutions without the expertise or experience with salvage techniques, patients may only be offered PDC replacement or conversion to haemodialysis. PDC salvage is an invaluable tool in the armamentarium of options for ESI/TI because it allows the patient uninterrupted PD thereby avoiding the risks and expense of haemodialysis.
Patients who are poor candidates for haemodialysis due to logistical reasons or with an expiry of vascular access options may benefit even more from a salvage-first approach. In special populations such as children, it may be impossible to interrupt PD for a prolonged time due to inability to obtain vascular access for haemodialysis.
Authors’ technique
The authors’ preferred technique is a combination of CS, BR and CD. We favour this approach as it harnesses the benefits of all the components and is easily reproducible. CS also does not preclude the possibility of employing PR for subsequent infections. The procedure has a short learning curve and has proven to be effective for the patients at our institution.
Limitations
This review should be interpreted with several limitations. The main limitation is the low quality of included studies which does not allow for meta-analysis or strong conclusions about the superiority of either technique. Only a pooled analysis across all studies was performed, as several studies were lacking in methodologic granularity and baseline patient information. There were also huge variations in reported outcomes which impeded formal analysis of the outcomes. However, despite its limitations, this is the first systematic review of the available literature on PDC salvage techniques in the setting of ESI/TI. Our institution’s results with CS + BR + CD are limited by the small sample size and the lack of a comparator arm.
Conclusion
This review demonstrates that PDC salvage techniques are safe and effective in the setting of refractory ESI/TI. Future prospective comparative trials are required to determine which technique is more effective. We hope that this review can increase awareness and consideration of a salvage-first approach in selected patients who may benefit from more months and years of PD.
Footnotes
Acknowledgements
The authors would like to acknowledge the patient who provided written consent for the photos taken to illustrate the procedure.
Author contributions
JJYS, NZPN, SQWL and SGT conceived the study. JJYS and NZPN were involved in article review and data analysis. JJYS wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
No ethical approval was required for the conduct of this systematic review.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent to participate
No participants were directly included in this study.
Informed consent to publish
Written informed consent was obtained from the patient for the anonymised illustrations published in this article (see acknowledgements).
Trial Registration
Not applicable.