
Abstract
Kidney injury and cardio–renal syndrome is a common complication of end-stage cardiomyopathy and heart failure. Although renal function often improves after placement of left ventricular assist devices (LVADs), this is frequently not sustained, and many patients progress to end-stage kidney disease (ESKD). In-centre haemodialysis (HD) is the most common dialysis modality in patients with LVADs and there are only rare case reports of maintenance dialysis with peritoneal dialysis (PD) in patients with VADs. Barriers to the use of PD as renal replacement modality in patients with LVAD include lack of familiarity with acute-start PD, concerns regarding interruption of anticoagulation for PD catheter placement and historic concerns of PD-associated peritonitis risk causing VAD drive-line infection, though this risk is reduced with modern pre-peritoneal VAD drive-lines. PD may offer advantages in this cohort including improved haemodynamic stability and avoidance of vascular access, with lower rates of bloodstream infections as compared to HD. PD may also aid preservation and restoration of kidney function in patients with LVADs and kidney injury. We report a case of a patient with non-ischaemic dilated cardiomyopathy and existing LVAD, with ESKD managed successfully with maintenance PD. The patient was maintained on PD for 10 months prior to a subsequent successful combined heart–kidney transplant.
Keywords
Introduction
We report a case of a patient with non-ischaemic dilated cardiomyopathy (NIDCM) and left ventricular assist device (LVAD) who progressed to end-stage kidney disease (ESKD), managed successfully with maintenance peritoneal dialysis (PD). The patient was maintained on PD for 10 months prior to successful combined heart–kidney transplant.
Case
A male in his 40s (height 174 cm, weight 96 kg, body mass index 31.7 kg/m2, waist circumference 108.5 cm) with long-standing insulin-dependent diabetes mellitus and significant smoking history was diagnosed with NIDCM in his 20s. His progressive decline in function to New York Heart Association class III symptoms necessitated placement of a biventricular pacemaker and cardiac defibrillator. Despite this, he had repeated exacerbations of heart failure, with multiple hospital admissions involving brief periods of kidney replacement therapy with continuous veno-venous hemofiltration (CVVH) in intensive care.
After a lengthy admission with decompensated heart failure unresponsive to inotrope and loop diuretic infusion, the patient underwent placement of a durable HeartMate III LVAD as a bridge to heart transplant. Acute kidney injury after LVAD insertion was managed with CVVH before kidney recovery. He required high-dose diuretic therapy with furosemide 500 mg oral three times/day, bumetanide 2 mg oral three times/day and hydrochlorothiazide 25 mg oral daily. Heart–kidney transplant workup commenced concurrently with dialysis education and planning. The patient had no prior abdominal surgeries and expressed a preference for PD in the event that kidney transplant did not proceed before requirement for maintenance dialysis.
One year after LVAD placement, the patient was readmitted with refractory fluid overload resistant to intravenous loop diuretic and inotrope infusions. He was admitted to intensive care and commenced CVVH, achieving a net 15-L ultrafiltration to 94 kg. As CVVH failed to achieve further fluid removal due to haemodynamic instability and the patient preferred PD for maintenance dialysis, a 48 cm PD catheter was inserted under fluoroscopic guidance by interventional radiologists. To facilitate PD catheter insertion, usual LVAD anticoagulation was bridged with heparin, ceased 6 h before and resumed 2 h post-procedure. The PD catheter was inserted in the right iliac fossa, away from the LVAD driveline (Figure 1). Three days after PD catheter insertion, continuous automated cyclic PD was commenced with 13 cycles of 1000 ml (90% tidal) 2.5%/4.25% dextrose-based PD solution over 16 h, achieving 2.1–2.8 L ultrafiltration daily. Initial therapy was administered supine and there were neither leaks around the PD catheter nor local complications complicating PD initiation.
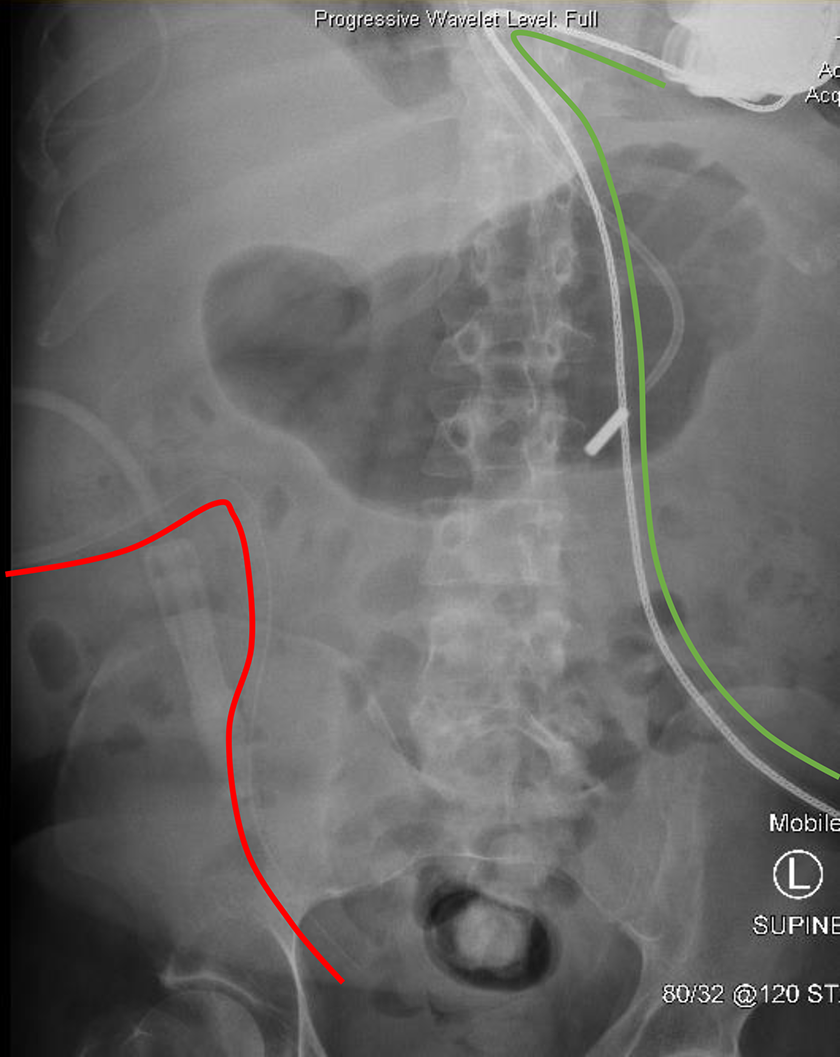
Abdominal xray demonstrating peritoneal dialysis catheter, sited as far as practicable from the LVAD driveline, in order to minimise risk of cross-contamination.
Four days later, PD volume fill was increased to 1600 ml, transitioning 10 days after PD catheter insertion to nocturnal 5 cycles of 2000 ml 2.5% dextrose-based PD solution over 10 h, with 1000 ml icodextrin day fill. One month after PD commencement, urine output was 282 ml/24 h (creatinine clearance 0.82 ml/min), on furosemide 500 mg oral twice daily.
The patient received VAD and PD education and was discharged with continuous milrinone infusion via peripherally inserted central catheter line, at a weight of 71 kg. The patient administered PD at home independently and no episodes of PD peritonitis complicated therapy.
The patient did not experience significant kidney recovery, urine output was 221 ml/24 h (creatinine clearance 0.6 ml/min) 7 months after commencement on PD. Kt/V was 1.55 (1.48 dialysis, 0.07 residual); the prescription achieved 2 L ultrafiltration per day, maintained euvolaemia and was well tolerated in the context of the patient’s lifestyle and restrictions associated with the LVAD. The patient maintained an excellent solute profile, with serum urea <14 mmol/L, normal serum potassium, bicarbonate and phosphate in the 5 months prior to transplant.
Ten months after PD commencement and 2 years after LVAD placement, the patient underwent combined heart–kidney transplant and LVAD explant. A minor peritoneal breach during kidney transplant was identified repaired at the time of surgery. PD was commenced 2 days post-transplant for delayed graft function and hyperkalaemia, with 5 cycles of 1200 ml 1.5% dextrose-based PD solution, over 10 h. Dialysis independence was achieved 10 days post-transplant and the PD catheter was removed 4 weeks later.
Discussion
Kidney injury and cardio–renal syndrome are common complications of end-stage heart failure. 1 Mortality rates are high for patients on long-term dialysis who undergo LVAD placement and accordingly, LVAD placement in this population is typically offered only as a bridge to heart–kidney transplantation, rather than as destination therapy. 2 –4 In patients with kidney failure presumed cardio–renal in nature however, LVAD placement may be considered if dialysis-independence is expected with improved cardiac output. 5
Patients requiring dialysis after LVAD placement include those in whom acute kidney complicated LVAD placement, those who did not make the expected gains in kidney recovery post LVAD placement and those who progressed to ESKD despite LVAD placement. 6,7 In-centre haemodialysis (HD) is the most common dialysis modality utilised in patients with LVADs 8 but has associated risks related to central line infections and LVAD pump failure on HD. As LVADs are unable to upregulate or downregulate in response to haemodynamic demands of HD, hypovolemia on HD is even more significant in patients with LVADs as compared to the general dialysis population, as it causes the LVAD inflow cannula to pull against the interventricular septum and may compromise cardiac output. 5
PD has been commenced in patients with existing VADs for various indications, including lack of options for vascular access, 9 infected HD access, 10 haemodynamic instability on HD 11 and inability to find a HD centre willing to accept a patient with a VAD. 12 PD may offer advantages over HD in patients with LVADs, including haemodynamic stability 5 and avoidance of bloodstream access and lower rates of associated infections. 2,5,10 Additionally, the gentler ultrafiltration on PD may impart a greater chance of improved kidney function when compared to patients commenced on HD post LVAD placement, though numbers are small and outcomes are mixed (Table 1).
Case reports of peritoneal dialysis in patients with existing LVAD.
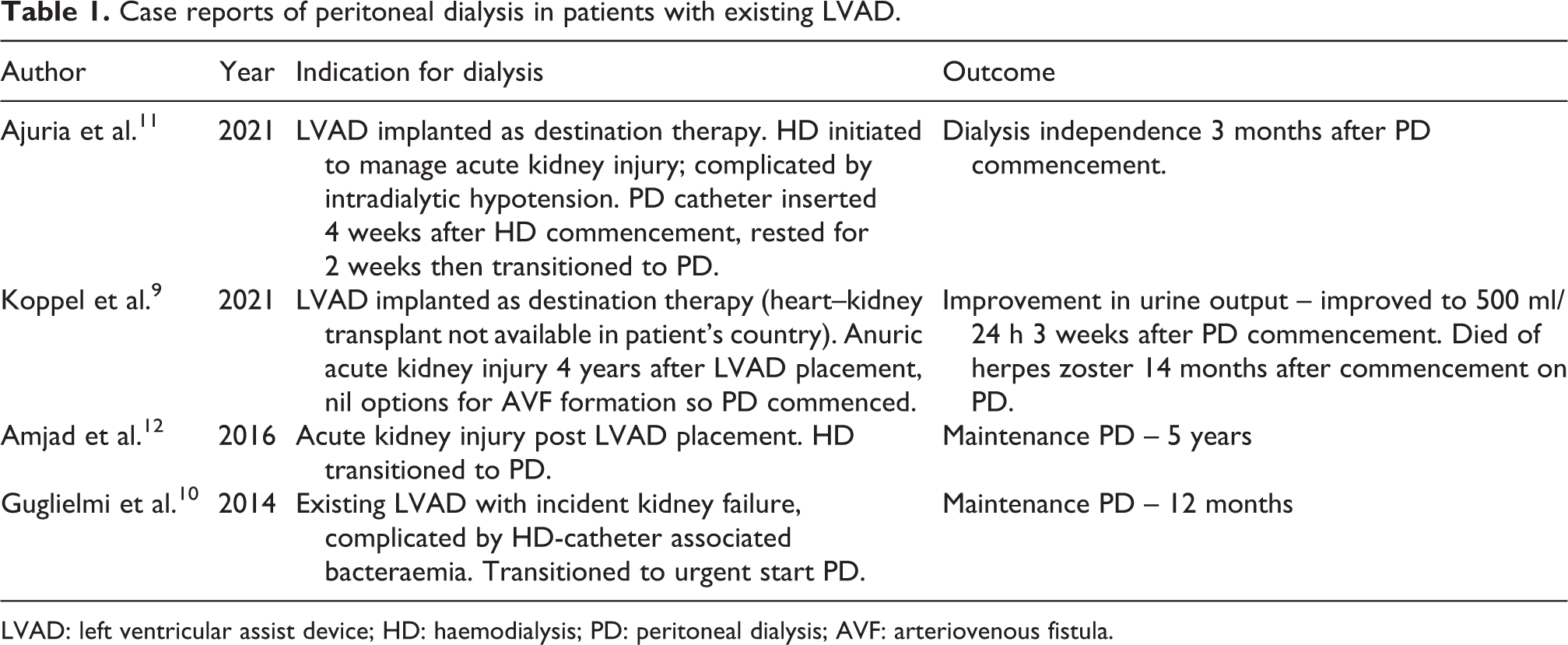
LVAD: left ventricular assist device; HD: haemodialysis; PD: peritoneal dialysis; AVF: arteriovenous fistula.
Barriers to the use of PD as dialysis modality in patients with LVADs include lack of familiarity with urgent start PD, concerns regarding interruption of anticoagulation for PD catheter placement and historic concerns of PD-associated peritonitis causing LVAD drive-line infection. 5 First- and second-generation LVADs were implanted in the pre-peritoneal space, competed for space with the PD catheter and were felt to pose unacceptable cardiac infection risk in the event of PD-associated peritonitis. 13,14 Contemporary LVADs have a pre-peritoneal driveline and are not at the same risk of infection in the event of PD-associated peritonitis as earlier VAD iterations. 10 While data are limited, infection concerns empirically support placement of the PD catheter exit-site as far away practicable from the driveline site.
This report details a patient with LVAD and ESKD, successfully managed with PD until combined heart–kidney transplantation. This case demonstrates that urgent start PD can be effectively and safely be initiated in patients with LVADs, provided that there is facility for acute catheter placement, trained staff to initiate and supervise instillation and cycling of initial low fill volumes and strategies for escalation based on patient tolerance and clearance requirements, both solute and volume.
This case further demonstrates that PD can be successfully maintained in patients with LVADs as a bridge to combined heart–kidney transplant. PD offers many potential haemodynamic and lifestyle benefits in ambulatory heart failure patients in general and patients with LVADs in particular. Though there are no direct comparisons of gains in kidney function with one dialysis modality over another in patients with LVADs, PD may aid preservation and restoration of kidney function in patients with LVADs. 9,11 More data are required regarding outcomes for dialysis-dependent patients with LVADs with regards to infection rates, quality of life and improvement in kidney function, to help inform choice of one dialysis modality over another and better investigate the possible benefits of PD in this patient group. 14
Footnotes
Acknowledgement
The authors thank staff of the Peritoneal Dialysis Unit, Alfred Health for their support.
Author contribution
All authors made a substantial contribution to this case report, drafted or revised the article and approved the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent to participate
Informed signed consent as per Alfred Health guidelines, included in patient electronic medical record.
Informed consent to publish
Informed signed consent as per Alfred Health guidelines, included in patient electronic medical record.