
Abstract
Background:
Early non-infectious complications at initiation of peritoneal dialysis (PD) are a major burden with unknown long-term impacts on individuals.
Methods:
Prospective multicentre cohort study using univariable and multivariable Cox regression to identity mortality risk and PD discontinuation risk in those with and without non-infectious complications. All individuals commencing PD between 1 January 2014 and 31 December 2018, registered in the New Zealand Peritoneal Dialysis Registry (NZPDR) were followed up to 31 December 2020. Early non-infectious complications defined as functional, catheter-related, exit-site dialysate leak or anatomical leak complications occurring within 30 days of initiation of PD. Primary outcomes were patient survival and time on PD therapy. Secondary outcomes were peritonitis free survival, first PD catheter survival and catheter tunnel infection free survival.
Results:
Of 1596 individuals included in the study, 102 experienced an early non-infectious complication. Multivariable analysis demonstrated these complications were associated with higher risk of overall mortality (hazard ratio (HR) 1.71; 95% confidence interval (CI) 1.21–2.44), PD discontinuation (HR 1.84; 95% CI 1.41–2.41) and first catheter failure (HR 2.89; 95% CI 2.28–3.66). No difference was found for risk of development of first peritonitis episode or catheter tunnel infection. Mortality risk was associated with functional and exit-site dialysate leak complications and continued beyond 180 days. Risk of PD discontinuation and first catheter loss were associated with catheter and functional complications in the first 180 days.
Conclusion:
Early non-infectious complications are associated with long-term mortality risk. Further research in risk factors and causes of early non-infectious complications are required.
Introduction
Since the introduction of continuous ambulatory peritoneal dialysis (PD) in the late 70s, it has become increasingly used as a home-based method of kidney replacement therapy. Current estimates worldwide suggest PD represents 11% of the dialysis population with a global growth rate of the number of patients on PD being 8% annually. 1 New Zealand has one of the highest prevalence of PD usage worldwide with 176 individuals per million population in 2019. 1,2 PD has been associated with increased patient quality of life and patient satisfaction compared to haemodialysis. 3,4 Studies examining survival differences between the two modalities however have mixed results. 5 –7
Complications of PD, either due to infectious or non-infectious causes, can lead to transfer to haemodialysis in up to 25% of individuals with more than 70% of them occurring in the first 2 years after initiation of PD, predominantly associated with peritonitis. 8 PD discontinuations caused by non-infectious causes have been reported up to nine episodes per 100 patient-years at 6 months and seven episodes per 100 patient-years at 12 months in Australia and New Zealand. 9 While there has been a focus on predictors of PD discontinuation, such as peritonitis rates, catheter types, insertion techniques and salvage techniques for peritoneal catheters, 8 –16 there has been little focus on the consequences of early non-infectious complications following insertion of peritoneal catheters.
To the best of our knowledge, only one prospective study examined the optimum timing for catheter usage in regard to reducing risk of catheter leakage or primary catheter malfunction. 17 Although prospective data do exist for predictors for PD discontinuation in PD, this does not focus on how early non-infectious complications at the initiation of PD affects either PD discontinuation rate or survival rate. 8 Our study examined the impact of early non-infectious complications at the initiation of PD on individual’s long-term outcomes.
Materials and methods
Study design
This was a multicentre prospective cohort study using individual level data from the New Zealand Peritoneal Dialysis Registry (NZPDR). 18 Permission to analyse the de-identified data was obtained from the NZPDR steering committee. NZPDR prospectively collected data on all PD patients from contributing centres and has ethical approval to collect and analyse the data.
Study population
All individuals who initiated PD between 1 January 2014 and 31 December 2018 and registered in the NZPDR were included in the study and were followed up to 31 December 2020. This included all individuals commencing PD, including those transferring from haemodialysis or returning to dialysis following a failed kidney transplant. All age groups fulfilling criteria were included.
Data collection
All data were collected prospectively by the NZPDR. Baseline characteristics at initiation of PD included sex, age, ethnicity, weight, presence of diabetes, primary cause for kidney disease, PD catheter type (coiled end/straight intercuff, straight end/swan neck intercuff, coiled end/swan neck intercuff, straight end/straight intercuff), operator who inserted catheter, year started PD, number of days post insertion prior to PD catheter use, small solute clearance (Kt/V), total kidney clearance from dialysis and residual kidney function and peritoneal equilibrium testing. Initiation of PD was defined as the first date of PD treatment. Non-infectious complications were grouped and defined as either catheter, functional, exit-site dialysate leak or anatomical leak complications. Catheter complications were defined as solely related to the catheter itself such as migration or damage to the catheter while functional complications were defined as complications with either inflow or outflow of dialysate. Exit-site dialysate leak complications were defined as the appearance of any moisture around the PD catheter exit site identified as dialysate. Anatomical leak complications were defined as loss of dialysate from the peritoneal cavity due to innate anatomical weakness or fistulae. Surgical, infective and other complications were not included in the definition of non-infectious complications. Infective complications were defined as either exit site, tunnel track or peritonitis infections, and surgical complications pertain to either intraoperative or post-operative complications associated with the insertion of the catheter including surgical wound infections. NZPDR complication codes and corresponding subgroups are provided as a supplementary file. Complications that occurred within 30 days of initiation of dialysis were defined as early complications. The first early complication an individual encountered assigned their complication type.
Clinical outcomes
The primary clinical outcomes were patient survival and time on PD therapy. Time on PD therapy was defined as number of days until transfer to haemodialysis therapy for more than 90 days, kidney transplantation or withdrawal from dialysis due to medical or psychosocial reasons. Secondary outcomes evaluated were peritonitis free survival, first PD catheter survival and PD catheter tunnel infection free survival. These secondary outcomes were defined as the period of time until the development of either peritonitis, removal of first PD catheter (whether resulting in or not resulting in PD discontinuation) or development of a catheter tunnel infection respectively.
Statistical analyses
Baseline characteristics that were in categorical form were presented as number of individuals and percentages, while those in continuous form were presented as median and interquartile range (IQR). Follow-up continued until the occurrence of an outcome (see above) or until became censored as appropriate for death, kidney transplantation or discontinuation from the registry. Time from initiation of PD to occurrence of each outcome (primary or secondary) was first compared between those with and without any type of non-infectious complications. This was done by using Kaplan–Meier plots and by estimating hazard ratios (HRs) using univariable Cox regressions. Then, multivariable Cox regressions were used to adjust for confounders. Underlying proportional hazard assumption was assessed by testing for nonzero slope in a generalised linear regression of the scaled Schoenfeld residuals on time, which is equivalent to testing that the log HR function is constant over time. 19 These multivariable models included the covariates of sex, age, catheter type, operator who inserted the PD catheter and primary disease which caused end-stage kidney failure (ESKF). These adjusting covariates were chosen based on association with outcome of interest as per univariable analyses with p value <0.2 threshold and biological plausibility. Diabetes mellitus was not used as a separate adjusting variable due to perfect collinearity with ‘primary cause of ESKF’. Pairwise deletion was used in the multivariable analyses for missing covariate data. To assess longer term effects, sensitivity analyses were then performed using univariable and multivariable models with different two time intervals of 0–180 days and 181 days onwards since initiation of PD to estimate HRs for their respective outcomes.
Then, the same analysis was repeated to compare survival times between those who experienced each type of non-infectious complication (catheter, functional, exit-site leak) and those without that type of non-infectious complication. These latter analyses were confined only to the univariable level to avoid model overfitting due to smaller sample sizes. 20 Anatomical leaks were not analysed in subgroup analysis due to underlying pathological heterogeneity and small sample size. Sensitivity analyses were also performed using univariate models on their respective outcomes to assess statistically significant difference of HRs with two different time intervals of 0–180 days and 181 days onwards since initiation of PD.
Stata/SE16.0 (StataCorp, Texas, USA) was used in all analyses. The findings are reported following the STROBE statement. 21
Results
Individuals
A total of 1596 individuals who were initiated PD between 1 January 2014 and 31 December 2018 and registered in NZPDR were identified (Figure 1). The demographic characteristics of these participants are presented in Table 1. Median age was 60 years (IQR 49–69) and 59.5% were male. Ethnic classification was 40.1% European, 27.8% Māori and 12.5% Pacifica. Diabetes mellitus was the aetiology of kidney failure for 43.4% of individuals. Median number of days after insertion of PD catheter prior to use was 24 (IQR 17–32).
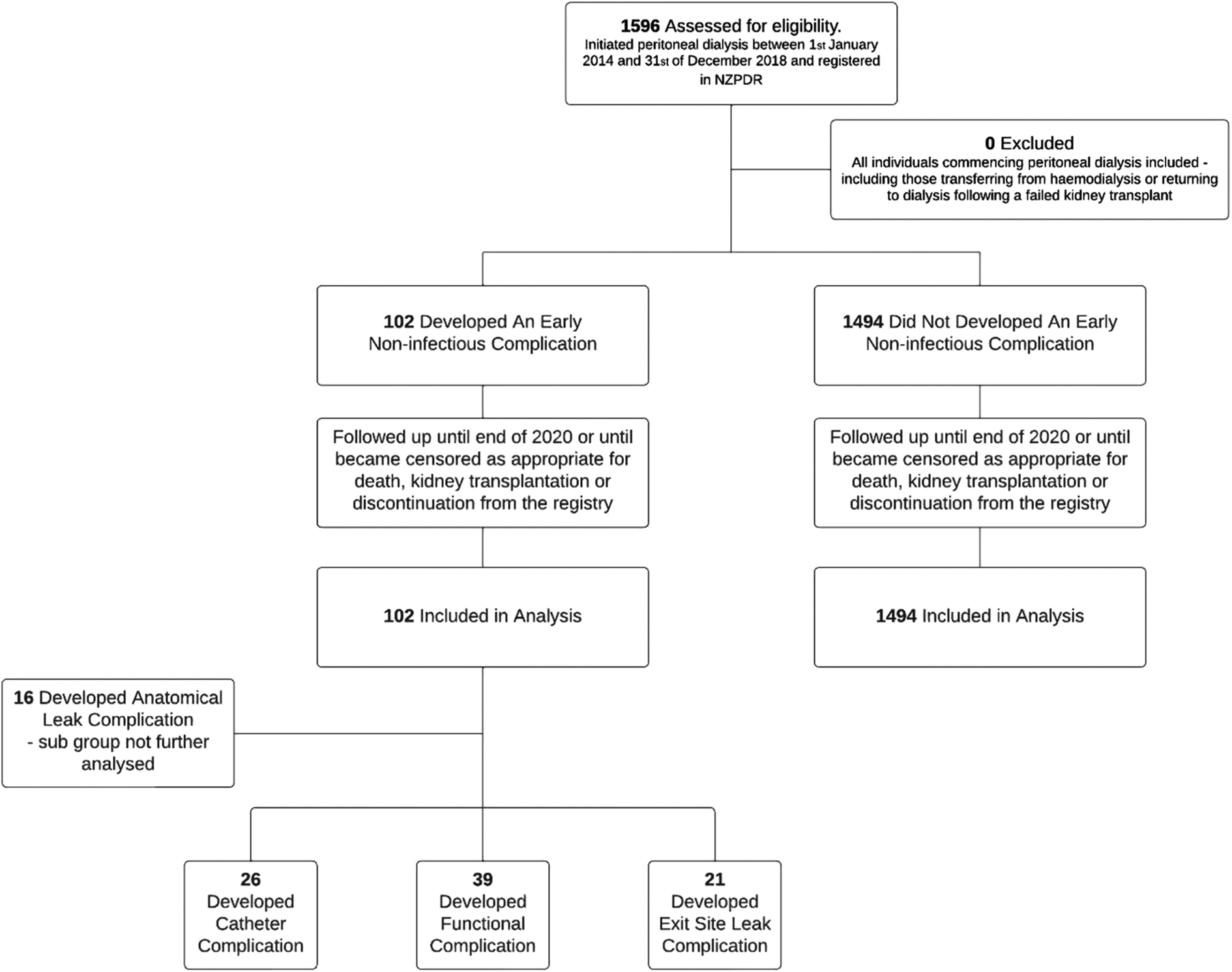
CONSORT flow diagram for multicentre prospective cohort study using registry level data.
Baseline characteristics and covariates of study participants.
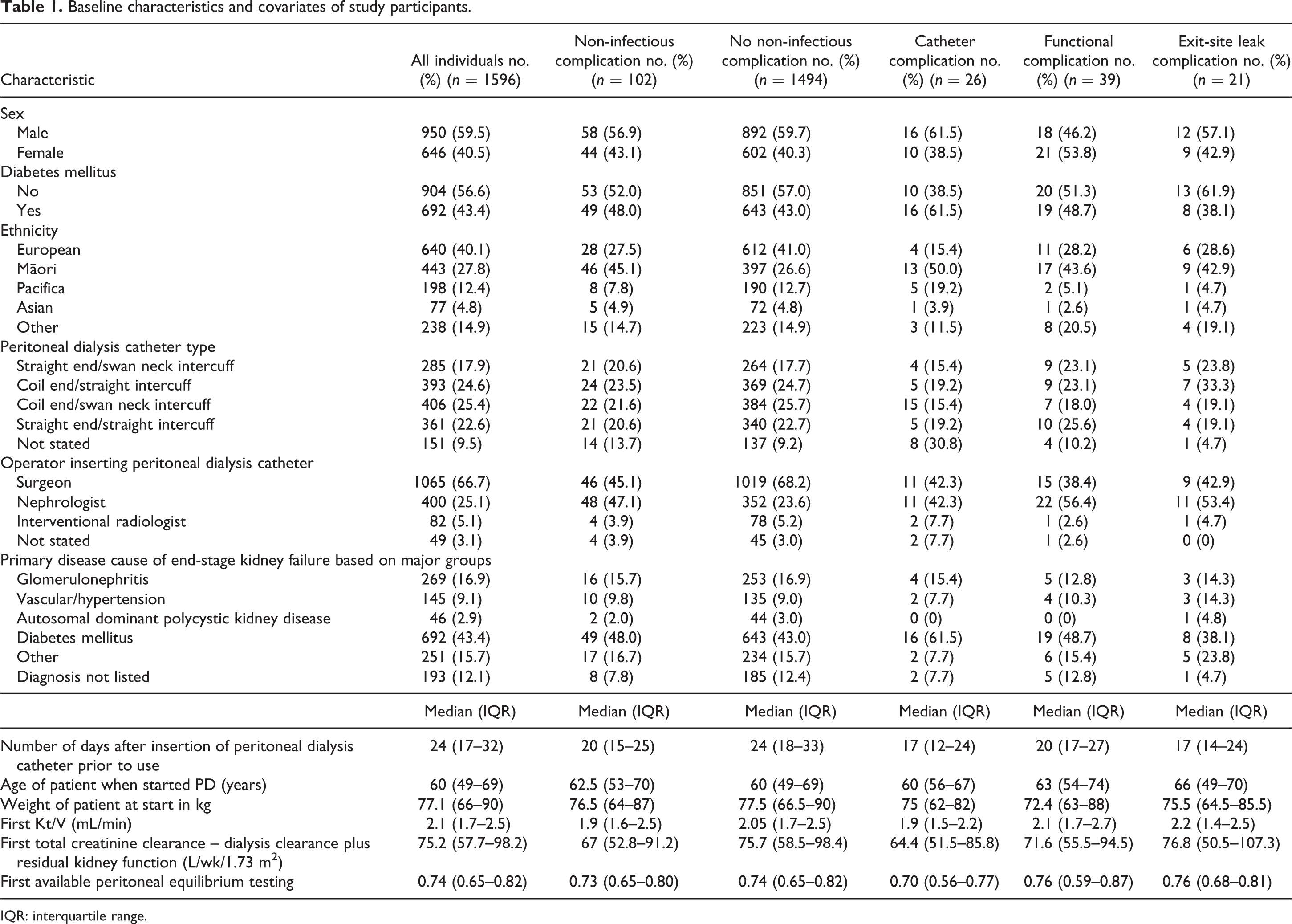
IQR: interquartile range.
Follow-up period during this study varied depending on the outcome measure and associated censoring. For the two primary outcomes of patient death and time on PD therapy, median follow-up days were 730 (IQR 369–1135)/756 (IQR 302–1182) (death/no death) and 450 (IQR 193–814)/983 (IQR 572–1375) (PD discontinuation/no discontinuation) respectively (Table 2).
Outcomes in patients with and without early non-infectious complications and in subgroups.
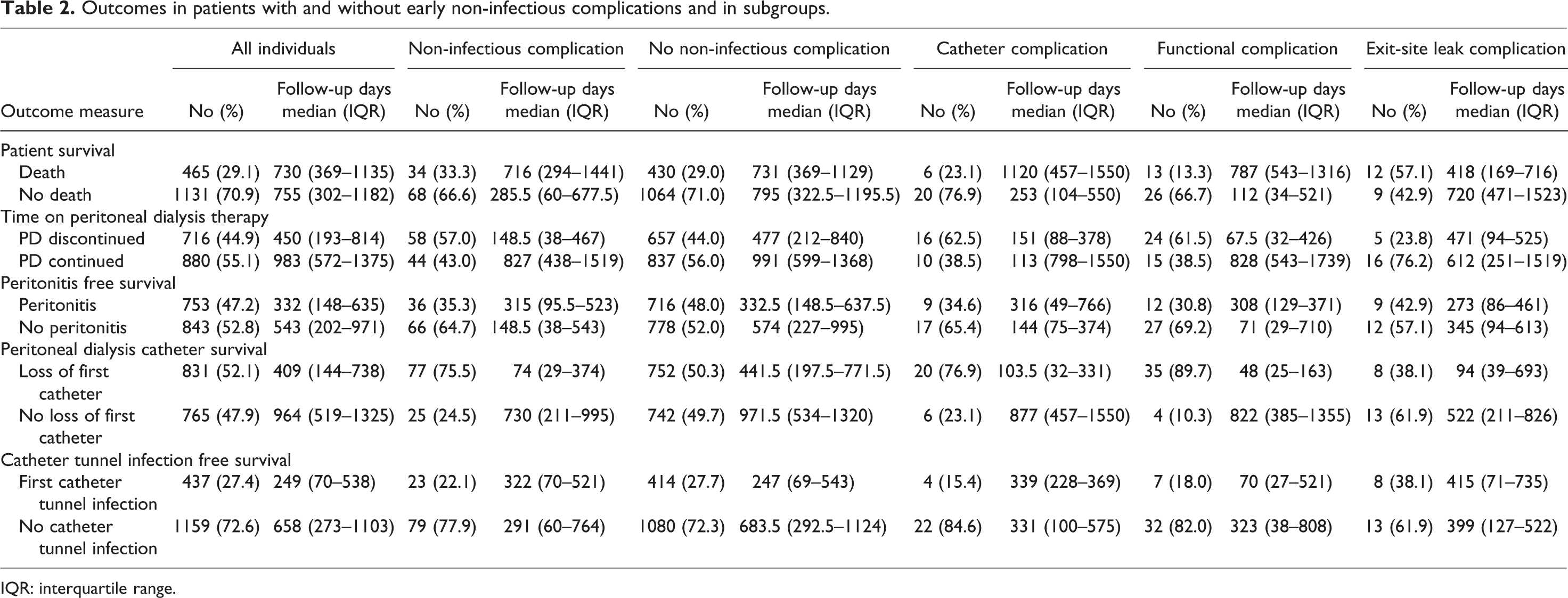
IQR: interquartile range.
There were 1366 individuals who did not experience any early complication following initiation of PD compared to 230 individuals who experienced at least one complication. These included 26 catheter complications, 39 functional complications, 21 exit-site leaks, 16 anatomical leaks, 106 infective complications, 9 surgical and 13 defined as other.
For catheter complications, 14 had catheter tip misplacement/early migration, 4 had catheter break/tear/damage, 1 had cuff extrusion/pulled out and 7 had late catheter tip migration (>4 weeks post-surgery).
For functional complications, 8 had supine and upright flow obstruction, 1 had inflow obstruction, 18 had outflow obstruction, 7 had catheter obstruction and 5 had omental entrapment.
Impact of early non-infectious complications
Out of 1596 individuals, 102 experienced at least one early non-infectious complication. Of these 102 individuals, 34 died during the follow-up period, 58 ended up with PD discontinuation, 36 had at least one episode of peritonitis, 77 experienced first catheter failure and 23 had at least one catheter tunnel infection (i.e. total number of these outcomes exceeded 102 because multiple types of outcomes possible per person).
Based upon Kaplan–Meier plots comparing outcomes between those with and without non-infectious complications (Figure 2), and HRs from univariable Cox regression, there was higher risk among those with non-infectious complications in terms of subsequent patient mortality (HR 1.71; 95% CI 1.21–2.44), PD discontinuation (HR 1.84; 95% CI 1.41–2.41) and first catheter failure (HR 2.89; 95% CI 2.28–3.66) compared to those without such complications. There was no difference in risk in terms of developing first episode of peritonitis (HR 1.12; 95% CI 0.80–1.57) or first episode of catheter tunnel infection (HR 1.08; 95% CI 0.71–1.65).
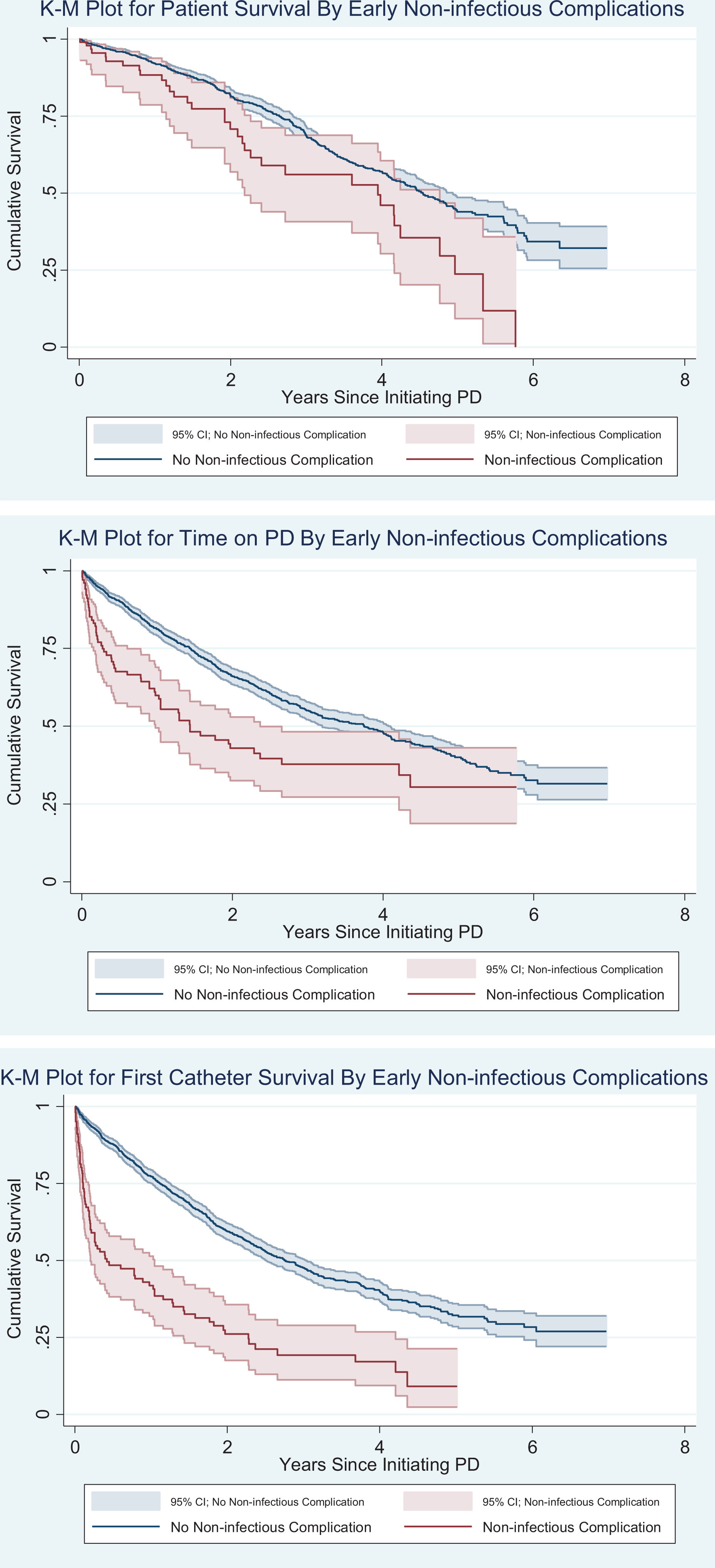
Kaplan–Meier plots for primary and secondary outcomes comparing early non-infectious complications versus those without early non-infectious complications.
The univariable findings did not vary by covariate adjusting (Table 3). Multivariable Cox regressions for each outcome measure using sex, age, catheter type, PD catheter inserter and primary cause for ESKF as adjusting covariates showed those with non-infectious complications had a higher risk of death (HR 1.62; 95% CI 1.11–2.37), PD discontinuation (HR 1.83; 95% CI 1.38–2.45) and first catheter failure (HR 2.70; 95% CI 2.10–3.47) compared to their counterparts without complications, while such a difference was not observed for risk of development of a first episode of peritonitis (HR 1.15; 95% CI 0.81–1.63) or a first episode of catheter tunnel infection (HR 0.99; 95% CI 0.62–1.56).
Multivariate (adjusted) hazard ratios comparing outcomes in patients with and without early non-infectious complication.
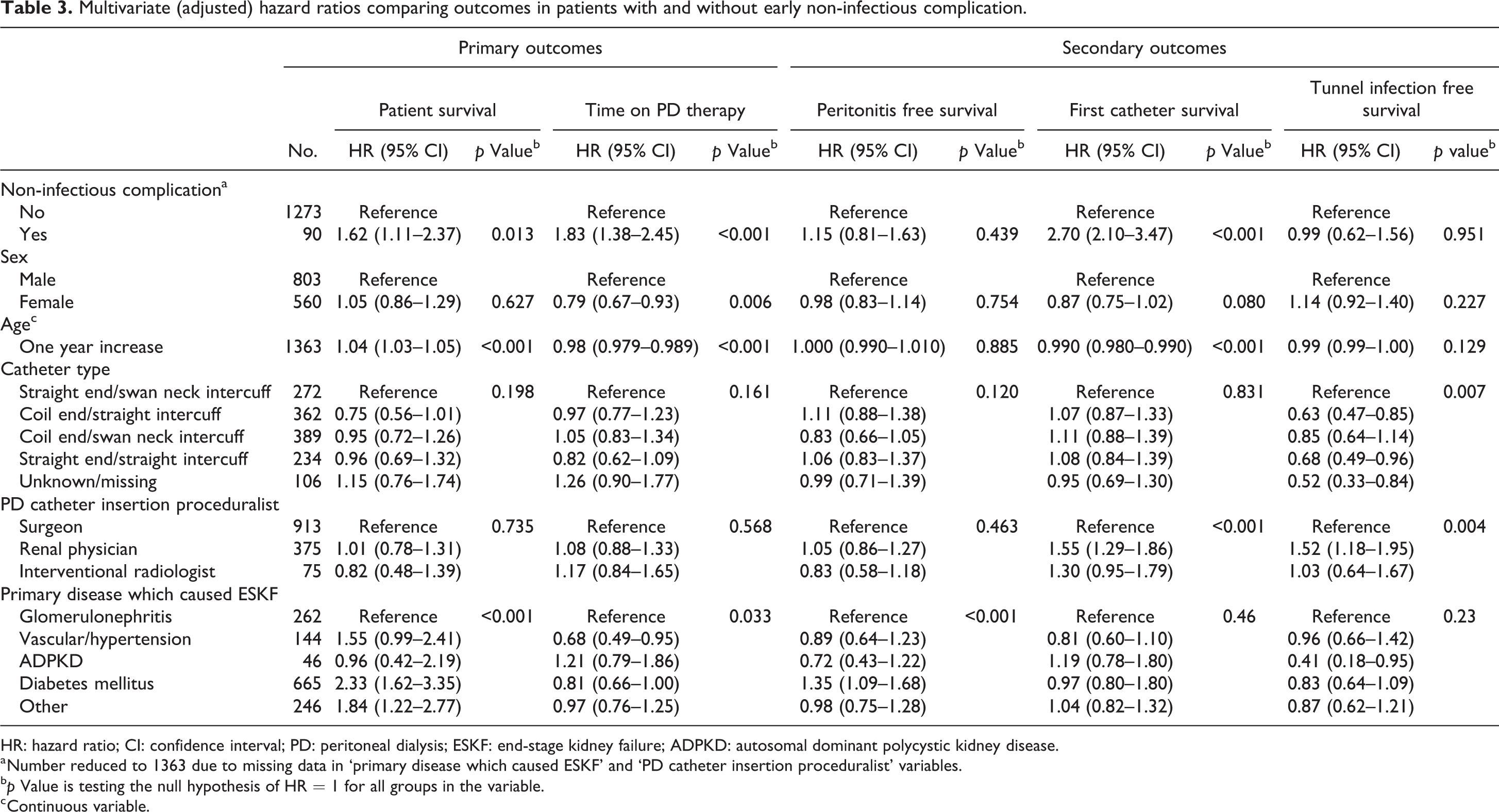
HR: hazard ratio; CI: confidence interval; PD: peritoneal dialysis; ESKF: end-stage kidney failure; ADPKD: autosomal dominant polycystic kidney disease.
a Number reduced to 1363 due to missing data in ‘primary disease which caused ESKF’ and ‘PD catheter insertion proceduralist’ variables.
b p Value is testing the null hypothesis of HR = 1 for all groups in the variable.
c Continuous variable.
As part of the multivariate analysis process, a number of additional observations were noted. The type of catheter inserted did not impact risk of mortality or PD discontinuation but there was a significant reduction in risk of developing a first catheter tunnel infection with the coiled end/straight intercuff (HR 0.63; 95% CI 0.47–0.85) and straight end/straight intercuff catheters (HR 0.68; 95% CI 0.49–0.96) when compared to straight end/swan neck intercuff catheters (Table 3). There were significantly higher risks in terms of failure of the first catheter (HR 1.55; 95% CI 1.29–1.86) and development of a first catheter tunnel infection (HR 1.52; 95% CI 1.18–1.95) among those catheters inserted by a nephrologist compared to surgical insertions (Table 3).
Sensitivity analyses with remodelling with two different time intervals of 0–180 days and 181 days onwards since initiation of PD reaffirmed the aforementioned higher mortality risk for those with non-infectious complications compared to those without such complications continues long-term (greater than 180 days), but not for PD discontinuation nor first catheter failure. Univariable analysis for the first 180 days did not show higher risk for patient mortality (HR 1.81; 95% CI 0.78–4.19) but was significantly higher for PD discontinuation (HR 3.96; 95% CI 2.69–5.81) and first catheter failure (HR 6.01; 95% CI 4.40–8.23). Beyond 180 days, however, higher mortality risk was significantly demonstrated (HR 1.96; 95% CI 1.16–2.50) but not for PD discontinuation (HR 1.12; 95% CI 0.76–1.66). Higher risk of first catheter failure just failed to reach significance (HR 1.46; 95% CI 0.99–2.17). Multivariate Cox regression resulted in similar observations with the first 180 days not demonstrating a higher risk of death (HR 1.37; 95% CI 0.54–3.49) but did demonstrate higher risk of PD discontinuation (HR 4.28; 95% CI 2.84–6.46) and first catheter failure (HR 6.14; 95% CI 4.4–8.57). Beyond 180 days, similar observations were demonstrated with higher mortality risk (HR 1.69; 95% CI 1.11–2.56) seen and no difference in either risk of PD discontinuation (HR 1.04; 95% CI 0.68–1.60) or risk of first catheter failure (HR 1.21; 95% CI 0.78–1.86) observed.
No statistical difference was seen between groups in both univariate and multivariate analysis for either time interval when comparing for outcomes for development of first peritonitis episode and first catheter tunnel infection.
Proportional hazard assumption was not found to be invalid in any of the models (both primary analyses and sensitivity analyses) except the univariable model for the first catheter failure outcome for the 0–180 days time interval. The assumption was met once adjusted for other covariates in the corresponding multivariable model.
Impact of each type of early non-infectious complication
Univariable analysis findings for each subgroup of early non-infectious complication are as follows. There was evidence of higher risk among those with catheter complications in terms of PD discontinuation (HR 1.94; 95% CI 1.18–3.18) and first catheter failure (HR 2.99; 95% CI 1.93–4.66) compared to those without catheter complications, but such a difference was not observed in terms of patient mortality (HR 1.14; 95% CI 0.51–2.56), development of first peritonitis episode (HR 1.13; 95% CI 0.58–2.14) or first catheter tunnel infection (HR 0.70; 95% CI 0.26–1.88). Sensitivity analysis with remodelling with the time interval of 0–180 days since initiation of PD demonstrated similar observations with higher risk of PD discontinuation (HR 3.69; 95% CI 1.88–7.22) and first catheter failure (HR 4.87; 95% CI 2.78–8.52) among those with catheter complications compared to those without. This was however not seen in remodelling for the time interval beyond 180 days for risk of PD discontinuation (HR 1.21; 95% CI 0.57–2.55) and first catheter failure (HR 1.75; 95% CI 0.83–3.70). No difference of risk was seen in either time interval for patient mortality.
For those with functional complications, there was a higher risk in terms of patient mortality (HR 1.74; 95% CI 1.00–3.02), PD discontinuation (HR 2.03; 95% CI 1.35–3.05) and first catheter failure (HR 4.59; 95% CI 3.27–6.45) compared to those with no functional complications. No difference was observed for development of first peritonitis episode (HR 0.93; 95% CI 0.53–1.65) or first catheter tunnel infection (HR 0.86; 95% CI 0.41–1.82). Sensitivity analysis with remodelling in the time interval of 0–180 days since initiation of PD similarly showed higher risk of PD discontinuation (HR 4.90; 95% CI 2.88–8.32) and first catheter loss (HR 9.65; 95% CI 6.44–14.46) but not in patient mortality (HR 0.81; 95% CI 0.11–5.88). Remodelling beyond 180 days, however, showed a higher risk of patient mortality (HR 1.92; 95% CI 1.08–3.41) but not in risk of PD discontinuation (HR 1.03; 95% CI 0.53–1.99) and first catheter loss (HR 1.69; 95% CI 0.84–3.40).
Exit-site leak complications showed evidence of increased risk of subsequent patient death (HR 2.14; 95% CI 1.14–4.01) but not in terms of PD discontinuation (HR 0.62; 95% CI 0.26–1.50), first catheter failure (HR 0.94; 95% CI 0.47–1.89), development of first peritonitis episode (HR 1.35; 95% CI 0.70–2.60) or first catheter tunnel infection (HR 1.76; 95% CI 0.88–3.55) when compared to those without leak complications. Sensitivity analysis showed similar risk with increased mortality in those with leak complications compared to those without in both 0 and 180 days time interval (HR 3.90; 95% CI 1.22–12.42) and beyond 180 days time interval (HR 2.11; 95% CI 1.09–4.08). No difference of risk was seen in either time interval for PD discontinuation (0–180 days: HR 0.93; 95% CI 0.23–3.75, 180+ days: HR 0.81; 95% CI 0.16–1.58) or first catheter failure (0–180 days: HR 1.93; 95% CI 0.80–4.68, 180+ days: HR 0.51; 95% CI 0.16–1.58).
When comparing the aforementioned specific complication groups with corresponding groups without that complication, sensitivity analysis did not identify a risk difference in either time interval for development of first peritonitis episode or first catheter tunnel infection.
Discussion
In this large prospective multicentre registry-base study, we examined the clinical impact of early (first 30 days) non-infectious complications following PD catheter insertion. We demonstrated that these early non-infectious complications were associated with a higher risk of overall subsequent mortality, PD discontinuation and first catheter failure. We demonstrated that mortality risk persisted long term and did not just pertain to higher risk in the short term unlike the risk of PD discontinuation and first catheter failure. This was demonstrated using a sensitivity analysis with remodelling for two separate time intervals with 180 days as a cut-off and the long median time of follow-up of greater than 700 days for patient survival in both with and those without non-infectious complications.
Early non-infectious complications were not associated with increased risks of development of first catheter tunnel infections or the first peritonitis episode. As peritonitis is a leading cause of mortality and PD discontinuation in individuals on PD, 22 –24 it is important to separate increased risk of peritonitis from early non-infectious complications on subsequent outcomes for PD.
The increased risk of mortality may be partially explained by the potential need for interim haemodialysis via haemodialysis catheters which is known to have associated increased risks of infection, cardiovascular events and mortality when compared to other forms of haemodialysis access. 25,26 The need for repetitive intervention for either haemodialysis access or re-establishment of PD access may also play a role due to the inherent associated risk of complications. Dialysis patients are more prone to complications and mortality associated with procedures in general. Studies examining adjusted mortality risks for chronic dialysis individuals report an adjusted risk ratio between 1.6 and 8.3 when compared to individuals with normal kidney function across different surgery types. 27 The increased risk of mortality in individuals with non-infectious complications however appeared predominantly confined to functional and leak complications only. This is likely due to differing underlying factors that predispose individuals to having certain complications and thus an underpinning a role in increased mortality. The lack of significance of higher mortality risk in the first 180 days is at least partly likely be due to the low outcome incidence and associated reduced power related with the small sample size, as evidence by the large confidence intervals. Only 6 out of 101 individuals who had an early non-infectious complication had the outcome of death in the first 180 days.
The risk of any early complications has been associated with diabetes, a history of glomerulonephritis, and has been seen more commonly in males. Previous abdominal surgery with abdominal wall complications and previous abdominal surgery in the setting of urgent start PD 28,29 have also been associated with early complications. Insertion technique of PD catheter (laparoscopic, open surgery and percutaneous insertion) may also play a role in obstruction and/or migration of the catheter risk with a tendency towards lower risk but not statistical significance in meta-analysis. 14 Due to low numbers in the subgroups of non-infectious complications, adjusting for these underlying risk factors was not possible in current study. This however exemplifies the need for further research to identify risk factors for non-infectious complications related to PD catheters and insertion, as little is known other than that reported in clinical trials looking at insertion technique and catheter type. 14 –16
Reduced time on PD therapy following early non-infectious complications was most pronounced within the first 180 days. This temporally matches what is seen with risk of loss of first PD catheter correlating with need for intervention. Data on the specific nature of catheter and functional complications with their potential interactions such as catheter tip migration and flow obstruction are not captured at present by the NZPDR. The short-term nature of higher risk of either outcome due to non-infectious complications is both logical and plausible. These complications may result in PD discontinuation due to requiring intervention for causes which may not be fully amendable to intervention. 12,30 Although radiological manipulation for flow dysfunction has been reported having a 46–75% success rate and laparoscopic rescue procedures have reported 63–100% long-term success rate, 30 these data are not currently recorded by the NZPDR. Repetitive complications and need for intervention may also influence an individual to transition to haemodialysis. This may be the explanation for why the reduced time on PD therapy was driven by catheter and functional complications rather than tunnel leaks. Early leaks are usually managed conservatively and do not often require surgery or removal of the catheter. 12
It was observed as part of the multivariate analysis that renal physician inserted PD catheters may be associated with higher risk of first catheter removal and first tunnel infection episode. This may be driven by how nephrologists inserted catheters, which was still a relatively new practice in New Zealand during this study period time, with the need to consider operator expertise development. An earlier study demonstrated similar first catheter 1 year and overall survival comparing peritoneoscopic (nephrologist) PD catheter insertion to surgical insertion but higher perioperative complications and poorer complication-free survival. 31
The major strength of this study is the prospective multicentre approach for data collection with a large cohort over a significant period of time. Almost all individuals in New Zealand who commence PD during the study time period were included with only 60 individuals missing when compared to the Australia and New Zealand Dialysis and Transplant Registry over the same 5-year time period. 32 Given the inclusion of those transferring for haemodialysis and following kidney transplantation failure, these results are representative of the New Zealand Peritoneal Dialysis population as a whole.
Major limitations include the NZPDR being not set up to record differences of local centre practices and guidelines. Due to this we are unable to examine how this may have affected the results. This study has highlighted some important gaps in the data that is collected as has been discussed above. Feedback to the registry will hopefully lead to improved data collection.
The low incident rate of specific complications did not allow multivariable analyses and adjustments for possible confounding in some of the analyses here. Further, possible contributing factors that may need to be adjusted for but were not available for multivariate analysis include body mass index, previous abdominal surgery, co-morbidity data and treatment interventions. However known factors associated with reduced patient survival on PD (diabetes, advancing age, reduced residual kidney function) and PD discontinuation (diabetes, younger age) were analysed and adjusted for in the primary analysis. Other known associated factors with subsequent mortality, including cardiovascular and peripheral vascular disease, and prior kidney replacement were not available but lack biological plausibility as risk factors for non-infectious complications. 8,9,33 –35
The NZPDR definition of time on PD therapy being defined as number of days until transfer to haemodialysis therapy for more than 90 days does not capture individuals with mild and reversible complications that resulted in temporary transfer to haemodialysis, but overall continuation with PD therapy.
In conclusion, we demonstrated that early non-infectious complications result in significant increased risk of hard outcomes of mortality long term and PD discontinuation short term. This stresses the need for further research in risk factors and causes of early non-infectious complications for risk stratification and prevention purposes.
Supplemental material
Supplemental Material, sj-pdf-1-ptd-10.1177_08968608221132647 - Long-term impact of early non-infectious complications at the initiation of peritoneal dialysis
Supplemental Material, sj-pdf-1-ptd-10.1177_08968608221132647 for Long-term impact of early non-infectious complications at the initiation of peritoneal dialysis by R Chan, RJ Walker, A Samaranayaka and JBW Schollum in Peritoneal Dialysis International
Footnotes
Authors’ note
Dr Chan is currently based at the Department of Renal Medicine, Wellington Hospital, Wellington, New Zealand.
Acknowledgement
The authors acknowledge the help of Dr Gerald Waters, the Director of the New Zealand Peritoneal Dialysis Registry, for his help with accessing the data for this study.
Author contributions
JS, RW and RC were involved in the concept of the study. RC was responsible for obtaining the data from the NZPDR. RC and AS undertook the statistical analyses. RC wrote the first draft of the manuscript. RW, AS, JS and RC were involved in the reviewing and editing subsequent versions of the manuscript. All authors approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not required as it is an audit from the NZ Peritoneal Dialysis Registry. The use of de-identified data from the NZPDR was approved by the NZPDR scientific committee.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
None.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.