
Abstract
Peritoneal dialysis (PD) catheter-related infections are important risk factors for catheter loss and peritonitis. The 2023 updated recommendations have revised and clarified definitions and classifications of exit site infection and tunnel infection. A new target for the overall exit site infection rate should be no more than 0.40 episodes per year at risk. The recommendation about topical antibiotic cream or ointment to catheter exit site has been downgraded. New recommendations include clarified suggestion of exit site dressing cover and updated antibiotic treatment duration with emphasis on early clinical monitoring to ascertain duration of therapy. In addition to catheter removal and reinsertion, other catheter interventions including external cuff removal or shaving, and exit site relocation are suggested.
This is a visual representation of the abstract.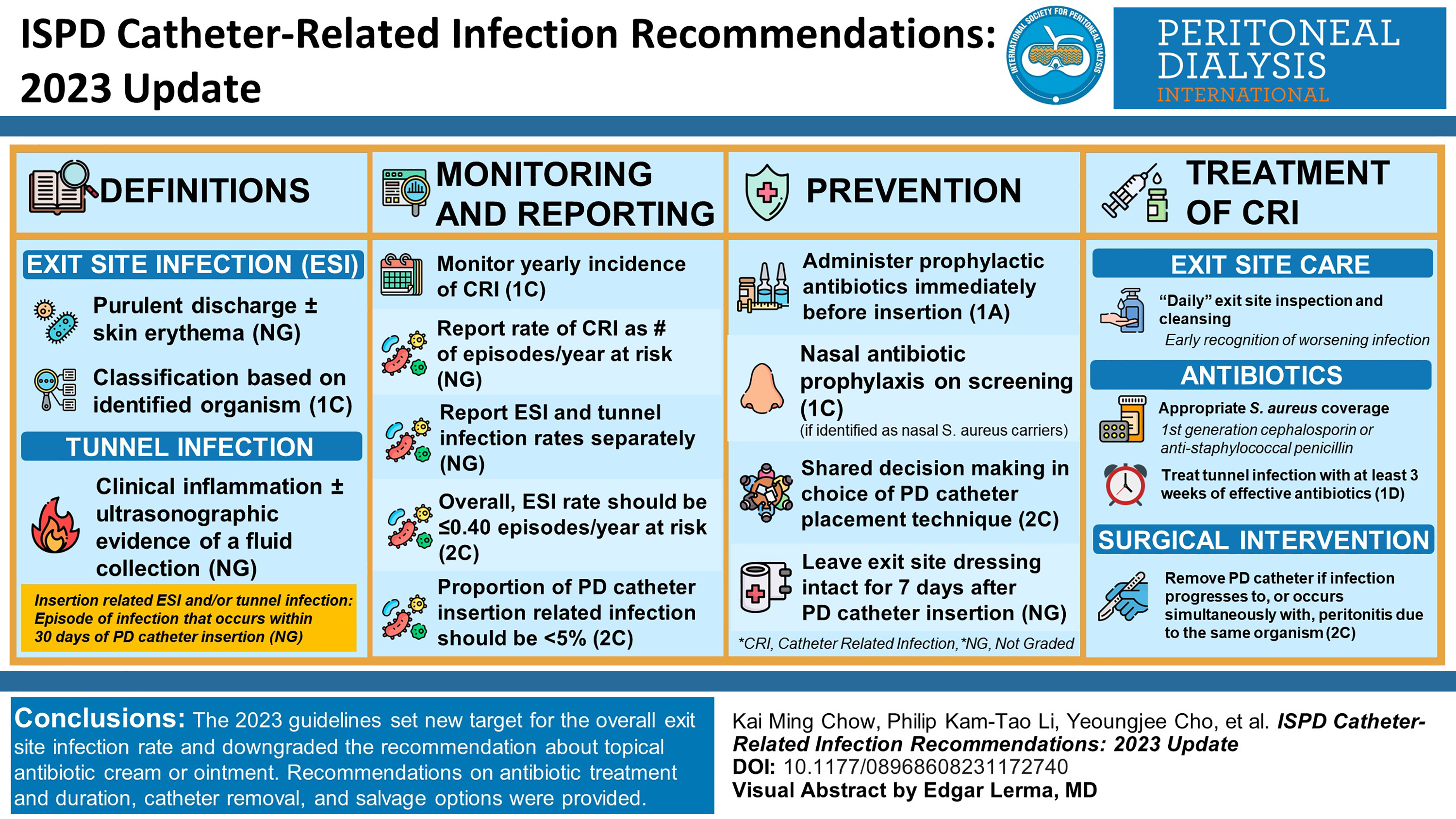
Keywords
What’s new with the 2023 update of the ISPD catheter-related infection guidelines?
Revised, clarified definition of tunnel infection (Page 2-3). New recommendation regarding cause-specific catheter-related infection (Page 3). New definitions of culture-negative catheter-related infection (Page 3), refractory catheter-related infection (Page 3-4), infection-related catheter removal (Page 4). Revised, updated recommendations for monitoring and reporting of catheter-related infections (Page 4). New target recommended for exit site infection rate (Page 4). Downgraded recommendation of topical antibiotic cream or ointment to catheter exit site (Page 6-7). Revised, updated recommendations for topical antibacterial agents (Page 6-8). Clarified suggestion about need of exit site dressing cover (Page 6-8). Revised recommendations for antibiotics treatment duration of exit site infection (Page 9-11). New salvage options suggested for exit site infection other than catheter removal (Page 11-13).
Introduction
Peritoneal dialysis (PD)-related infections have been identified by patients, caregivers and clinicians in the Standardised Outcomes in Nephrology – PD (SONG-PD) initiative as the topmost, critically important clinical outcomes in PD.
1
These include PD catheter-related infections (i.e. exit site infections and tunnel infections), which can potentially lead to PD peritonitis, hospitalisation, transfer to haemodialysis and death. Recommendations on the prevention and treatment of catheter-related infections were published previously together with recommendations on PD peritonitis under the auspices of the International Society for Peritoneal Dialysis (ISPD) for the first time in 1983 and revised subsequently including the latest catheter-related infection guideline from 2017.
2
The present guidelines focus on catheter-related infections, as recommendations pertaining to peritonitis have been updated recently.
3
The recommendations are organised into five sections focusing on: Definitions Monitoring and reporting of catheter-related infections Prevention of catheter-related infections Management of catheter-related infections Future research
These recommendations are based on contemporary evidence when such evidence is available. If there are multiple similar reports available on the same topic, the committee elected to refer to the more recent publications. In general, these recommendations follow the Grades of Recommendation Assessment, Development and Evaluation (GRADE) system for assessing the quality and level of evidence in clinical reports and for the grading of our recommendations. 4 Within each recommendation, the strength of recommendation is indicated as Level 1 (We recommend), Level 2 (We suggest) or Not Graded, and the quality of the supporting evidence if shown as A (high certainty), B (moderate certainty), C (low certainty) or D (very low certainty). The recommendations are not meant to be implemented in every situation indiscriminately. Each PD unit should examine its own pattern of infection, causative organisms and antibiotic susceptibilities and adapt the protocols to local conditions as necessary. Clinicians caring for paediatric PD patients should refer to the latest consensus guidelines for the prevention and treatment of catheter-related infections and peritonitis in paediatric patients receiving PD. 5
Definitions
The definitions pertaining to catheter-related infections can be further classified according to type, cause, timing (in relation to catheter insertion and to previous episodes) and outcomes.
Types of catheter-related infection
Exit site infection We suggest that definitive exit site infection is defined as the presence of purulent discharge, with or without erythema of the skin at the catheter-epidermal interface We suggest that, in the absence of purulent discharge, other signs of inflammation at the exit site (e.g. erythema, tenderness, swelling, granuloma or crust formation) are insufficient to definitively diagnose exit site infection
Tunnel infection
We suggest that tunnel infection is defined as the presence of clinical inflammation (erythema, swelling, tenderness or induration) with or without ultrasonographic evidence of a fluid collection anywhere along the catheter tunnel
The diagnosis of exit site infection is mostly clinical and should be considered whenever there is a change from the patient’s normal healthy exit site. Although exit site infection and tunnel infection can occur on their own, they can also occur concurrently. The diagnosis of exit site infection can be challenging as peri-catheter erythema without purulent discharge can be observed from allergic skin reaction, in the setting of a recently placed catheter or following trauma to the catheter, 6,7 or after a change in the dressing or cleansing materials. 8 Sometimes, erythema alone may be an indication of early infection warranting close monitoring for development of purulent discharge and need for antimicrobial treatment. A positive culture with a normal-appearing exit site (e.g. without purulent discharge) is indicative of colonisation rather than true infection. Although scoring systems 9,10 have been proposed to monitor the exit site, they have not been appropriately validated. We therefore suggest a diagnosis of exit site infection be based on the presence of purulent discharge, with or without erythema of the skin, at the catheter-epidermal interface. Based on a multi-centre study involving more than 30,000 assessments of exit sites in 3297 incident PD patients, the use of a scoring system (incorporating hyperaemia, oedema, pain, scab and granuloma) 2,9 for the diagnosis of exit site infection did not add much information in addition to the presence of purulent discharge. 7
A tunnel infection can present with various components of erythema, oedema, induration or tenderness over the subcutaneous pathway, often with a peri-catheter fluid collection demonstrated using ultrasound. 11
Cause-specific catheter-related infection
We recommend that exit site infections be classified according to organism(s) identified on culture (e.g. Staphylococcus aureus exit site infection)
We suggest that culture-negative exit site infection is defined when exit site infection is diagnosed using the criteria above, but no organism is identified on culture of the exit site swab
The cause of a catheter-related infection can be broadly divided according to the organism(s) to inform treatment. The most commonly isolated organisms reported for exit site infections in the mupirocin and Polysporin Triple (MP3) randomised controlled trial (RCT) were, in descending order of frequency, diphtheroids (20.5%), S. aureus (13.6%), Pseudomonas aeruginosa (13.6%) and fungus (9.1%). 12 In an RCT comparing topical application of mupirocin versus gentamicin at the exit site, the most commonly reported organisms in the mupirocin arm were S. aureus (0.06 episodes per year), other gram-positive organism (0.26 episodes per year) and P. aeruginosa (0.11 episodes per year). 13 There were fewer gram-positive and gram-negative exit site infections but more yeast infections in the gentamicin group. It is likely that the epidemiology of organisms will vary according to region, prophylaxis approach, antibiotic usage and so on. Classifying, monitoring and reporting catheter-related infections according to causative organisms will facilitate benchmarking and continuous quality improvement (CQI) activities, as well as inform more tailored treatment recommendations, as has occurred with the ISPD Peritonitis Guideline Recommendations over the last decade.
When no organism is identified after culture of purulent drainage from an exit site swab, culture-negative exit site infection is diagnosed. In the MP3 study, 12 culture-negative exit site infection occurred in five (11.4%) cases of exit site infection but was less common than culture-negative peritonitis (19.5%). Bernardini et al. reported a culture-negative exit site infection rate of 0.06 episodes per year in the mupirocin arm and 0.03 episodes per year in the gentamicin arm (p = 0.42). 13 Culture-negative exit site infections may occur in the context of recent antibiotic exposure, suboptimal sample collection or culture methods, or misclassification from slowly growing atypical organisms (e.g. mycobacteria, fungus).
PD catheter insertion-related exit site and/or tunnel infection
We suggest that PD catheter insertion-related exit site and/or tunnel infection be defined as an episode of exit site infection/tunnel infection that occurs within 30 days of PD catheter insertion
The use of a 30-day cut-point for defining PD catheter insertion-related exit site and/or tunnel infection was adopted in line with the ISPD Guidelines on Creating and Maintaining Optimal PD Access in the Adult Patient 14 and the ISPD Guidelines on Peritonitis. 3 Infections occurring within this time frame are likely to be related to the surgical procedure and may be associated with different organisms and outcomes.
Outcome-specific definitions of catheter-related infection
We suggest that refractory catheter-related infection is defined as failure to respond after 2 weeks of effective antibiotic therapy and appropriately intensified exit site care, or 3 weeks for infection due to Pseudomonas species
We suggest that infection-related catheter removal is defined as catheter removal due to catheter-related infection not responding to appropriate antibiotic therapy or surgical salvage procedures
A minimum 2-week course of antibiotics has been recommended for most catheter-related infections, except for those caused by Pseudomonas for which a 3-week course is recommended. In the literature, refractory tunnel infection has even been defined as failure to heal within 4 weeks. 15 Catheter-related infections that fail to completely resolve following the recommended antibiotic course duration can be defined as refractory catheter-related infections, thereby necessitating surgical salvage interventions or catheter removal.
Monitoring and reporting of catheter-related infections
We recommend that every programme should measure and monitor, at least on a yearly basis, the incidence of catheter-related infections
We suggest that the rate of catheter-related infection, including organism-specific catheter-related infection, should be reported as number of episodes per year at risk
We suggest that exit site and tunnel infection rates, including organism-specific rates, should also be separately reported as number of episodes per year
We recommend that the overall exit site infection rate should be no more than 0.40 episodes per year at risk
We suggest the proportion of PD catheter insertion-related infection within 30 days of PD catheter insertion should be less than 5% of all catheters inserted
At regular intervals, all PD programmes should monitor the incidence of catheter-related infections as part of a CQI programme. 16 Application of a standardised metric to measure outcome is critical to benchmark performance, monitor progress and implement strategies based on observed findings. Catheter-related infection rates should be measured as number of exit site infection or tunnel infection episodes divided by number of patient years at risk (i.e. number of years on PD starting from the time of PD catheter insertion), reported as episodes per patient years. This is different from the way of calculating rate of peritonitis, which is modified by whether or not PD exchange is being performed. As stated in the ISPD Guidelines on Peritonitis, 3 peritonitis rates are calculated separately for the period between PD catheter insertion and PD commencement (pre-PD peritonitis) and the period following PD commencement (PD peritonitis). Such separation is not applicable in calculating catheter-related infections because it is not modified by whether or not PD exchange is being performed.
Unlike PD-related peritonitis, catheter-related infections (i.e. exit site infections and tunnel infections) are generally not currently captured by kidney registries, including the Australia and New Zealand Dialysis and Transplant (ANZDATA) Registry and the US Renal Data System (USRDS). The PD Outcomes and Practice Patterns Study (PDOPPS) has reported a wide variation in the practice of monitoring for exit site infections across PD programmes from six countries (range: 41–100%/country). 17 Reported incidences of exit site infections have varied largely, ranging from 0.06 to 0.42 episodes per year. 13,18 –24 In the HONEYPOT trial involving 371 PD patients from 26 centres in 3 countries (Australia, New Zealand and Singapore) between 2008 and 2012, the exit site infection rate was 0.29 episodes per year in the standard of care arm using mupirocin versus 0.37 episodes per year in the antibacterial honey arm. 22 However, the incidence rate of exit site infection is expected to be higher in real life than in the setting of randomised trial, where patient selection occurs. We suggest that the overall exit site infection rate be no more than 0.40 episodes per patient years at risk. Although registry data are unavailable, this should be an achievable standard based on published literature and should be used as an initiative to reduce the burden of exit site infection rates globally. We also suggest PD units measure and report the proportion of PD catheter insertion-related infection, which should be less than 5% within 30 days of all catheters inserted in line with the ISPD Guideline on Creating and Maintaining Optimal PD Access in the Adult Patient. 14
Prevention of catheter-related infections
Catheter placement
We recommend that prophylactic antibiotics be administered immediately before catheter insertion for prevention of peritonitis
We recommend the use of nasal antibiotic prophylaxis if patients are identified as being nasal S. aureus carriers on screening prior to PD catheter insertion
We suggest that choice of PD catheter placement technique be left to shared decision-making between the individual clinician and patient as the comparative efficacies and safety of reported catheter placement techniques for the prevention of catheter-related infections are uncertain
We suggest that the exit site dressing should be left intact for 7 days after PD catheter insertion, unless soiled, to immobilise the new catheter and reduce risk of infection
The recommended practice and standard of PD catheter insertion has been detailed in the 2019 ISPD guideline on Creating and Maintaining Optimal Peritoneal Dialysis Access in the Adult Patient.
14
The 2022 Update of the ISPD Guidelines on Peritonitis Prevention and Treatment recommend ‘that systemic prophylactic antibiotics be administered immediately prior to catheter placement
A systematic review of 17 RCTs reported no significant impact of different types of catheter placement techniques on preventing catheter-related infection. However, the number of studies examining the impact of insertion technique or placement on catheter-related infections was small with variable methodological quality at risk of imprecision. For example, laparoscopic insertion compared to laparotomy made little or no difference to the incidence of catheter-related infections (3 studies, 270 participants: RR 1.00, 95% CI 0.43–2.31, p = 0.99). Similar results were observed for the subcutaneous burying or embedding of the PD catheter 6 weeks before initiation of PD (2 studies, 2511 patient-months: RR 1.15, 95% CI 0.39–3.42, p = 0.8), midline versus lateral insertion of the PD catheter (2 studies, 120 participants: RR 0.56, 95% CI 0.12–2.58, p = 0.45) and percutaneous insertion versus open surgical insertion (2 studies, 96 participants: RR 0.16, 95% CI 0.02–1.30, p = 0.08). 28
More recently, a systematic review and meta-analysis that included both observational (non-randomised) studies and RCTs found that, in low certainty evidence, percutaneous PD catheter insertion may have been associated with lower risks of early (within 1 month) exit site infection (7 studies; RR 0.36, 95% CI 0.24–0.53) and overall exit infection (16 studies; RR 0.61, 95% CI 0.46–0.82), but little or no difference in tunnel infection (7 studies; RR 0.76, 95% CI 0.38–1.51) compared with surgical (open and laparoscopic) PD catheter insertion. 29
Prior to catheter insertion, it is advisable to carefully identify the optimal location of the exit site that will allow the patient to be able to see their exit site, clean it and avoid inadvertently traumatising it (e.g. by the belt). 14 An alternative peritoneal catheter exit site location (e.g. upper abdominal, pre-sternal) may be particularly important for patients with morbid obesity, intestinal stomas or urinary or faecal incontinence. Ideally, the location of the exit site should be chosen in advance of catheter insertion with the patient in the seated position. Preoperative mapping with sample catheters or a marking stencil may be helpful for choosing an appropriate catheter type. Following catheter insertion, in keeping with other post-surgical care, the insertion site is covered and left undisturbed to allow wound healing by primary intention. 14,30 The exit site dressing should best be left intact for 7 days unless soiled to immobilise the new catheter and reduce risk of infection. 14,30,31 Cytotoxic agents such as povidone-iodine or hydrogen peroxide are to be avoided till the sinus has healed. 30 In general, PD is recommended to start at least 2 weeks after catheter insertion. 14 Earlier commencement of PD has been shown to increase the risk of dialysate leak (1 study, 122 participants: RR 3.90, 95% CI 1.56–9.78) with uncertain effect on the risk of exit site infection (2 cohort studies, 337 participants: RR 1.43, 95% CI 0.24–8.61; 1 case–control study, 104 participants: RR 1.20, 95% CI 0.41–3.50). 32
Catheter design
We suggest that the type of PD catheter used be left to shared decision-making between the individual clinician and patient as no catheter design has been demonstrated to be superior to another for the prevention of catheter-related infections
The risk of catheter-related infection is not influenced by the type of PD catheter (straight vs. coiled; 10 studies, 826 participants: RR 1.12, 95% CI 0.92–1.34, p = 0.22). However, these studies were of varying characteristics in terms of study duration, types of catheters (double cuff vs. single cuff; Tenckhoff vs. swan-neck catheter) and risk of attrition bias. 28 Use of a double cuff PD catheter has been shown to reduce the risk of peritonitis (RR 0.90, 95% CI 0.80–1.01, p = 0.08), especially S. aureus peritonitis rate (RR 0.46, 95% CI 0.33–0.64, p < 0.001), in a retrospective observational study involving 4247 incident PD patients from Canada. 33 However, the effectiveness of double cuff catheter on reducing the risk of catheter-related infection has not been clearly demonstrated. 34 Alternative catheter designs to decrease bacterial colonisation, such as silver-ion implanted 35 or antimicrobial-impregnated catheters, 36 have not been able to demonstrate consistent effectiveness with limited clinical experience to inform their use in a routine setting.
Training programmes
We recommend that the latest ISPD recommendations for teaching PD patients and their caregivers be followed
We suggest that retraining may reduce the risk of PD catheter-related infections
PD programmes should use the ISPD Training Guideline to implement standardised training for their trainers and patients in the PD unit. 37 However, currently there is no clear evidence to inform the best way to deliver training in terms of place, person or approach, 38 including optimal nurse-to-patient ratios. Recent data from PDOPPS including 1376 PD patients from 120 facilities across 7 countries demonstrated that PD training was most frequently performed at the facility (81%) by facility-affiliated nurses (87%) in a 1:1 setting (79%). 39 There was no convincing type of training-related characteristic that was consistently associated with a reduced risk of peritonitis; catheter-related infection outcomes were not examined. 39
Even though the most optimal way to deliver PD training remains uncertain, PD training has been shown to play a vital role in decreasing the risk of catheter-related infections. A single-centre, retrospective observational study from the United Kingdom has observed a 10-fold reduction in the burden of exit site infection after implementing a preventive programme focusing on training nurses and patients, 40 improving operative aseptic technique and reducing S. aureus nasal carriage. The training curriculum is advised to incorporate general theories of adult learning principles as a lower rate of exit site infection has been observed in association with this practice in a prospective observational study. 41 Currently, research is underway to identify how to best deliver training 42 incorporating an adult learning theory-based curriculum. Until further evidence is available, a dedicated nurse to support individual patient’s training focusing on adherence to guideline recommendations and antiseptic procedures is currently recommended. 43 Following completion of PD training, a home visit by the PD nurse is recommended to identify any environmental issues that may affect the risk of infection as well as confirm ongoing adherence to protocols and an acceptable standard of exchange technique.
In addition to the initial training at the time of PD commencement, regular retraining may be helpful to decrease the risk of catheter-related infection. An RCT of 104 incident PD patients from the Republic of Korea demonstrated that implementing frequent retraining in incident PD patients decreased the incidence of exit site infections over 24 months compared to the control group. 44 The indication, optimal frequency, duration and content of retraining have not been defined. 38
Exit site care
We recommend daily topical application of antibiotic cream or ointment (mupirocin or gentamicin) to the catheter exit site to prevent catheter-related infection
We suggest that the comparative efficacies of topical mupirocin versus topical gentamicin or exit site versus nasal application of mupirocin for preventing catheter-related infection are uncertain
We suggest that no cleansing agent has been shown to be superior to any other with respect to preventing catheter-related infections
We recommend that the exit site be cleansed at least twice weekly and every time after a shower or vigorous exercise, including running, cycling, swimming and water sports
We recommend that PD catheter exit site care be continued after interruption or discontinuation of PD for as long as the catheter remains in place
We suggest that a dressing cover over the exit site is not mandatory after exit site care and topical antibiotic application
We recommend that the PD catheter be immobilised to avoid traction injury of the exit site
Daily application of mupirocin to the exit site has been shown to be a cost-effective strategy to decrease the risk of exit site infection from S. aureus, in observational studies, RCTs and meta-analyses. 45 –47 Application of mupirocin was reported to reduce the risk of exit site infections by 62% among patients undergoing PD (five studies: RR 0.38, 95% CI 0.22–0.67). 46 In this systematic review, three studies involved nasal mupirocin application and two involved exit site application. Indeed, the site, frequency and duration of mupirocin treatment have been highly variable across the studies conducted to date thereby limiting their ability to inform standardised practice. 48 Daily administration is not as likely to induce mupirocin resistance compared with intermittent dosing, but the long-term implication remains uncertain. 49,50 A Cochrane systematic review and meta-analysis reported that topical nasal application of mupirocin had uncertain effects on exit site infection (3 studies, 338 participants: RR 1.34, 95% CI 0.62–2.87). 25 Unfortunately, exit site application of mupirocin was grouped with oral antibiotic prophylaxis (floxacin, cephalexin, rifampin or cotrimoxazole). While the overall analysis showed an uncertain effect of oral or topical antimicrobial prophylaxis on exit site infection (5 studies, 395 participants: RR 0.82, 95% CI 0.57–1.19) with moderate heterogeneity (I 2 = 40%, p = 0.17), the specific effect of topical exit site mupirocin was not evaluated. Obata and colleagues have recently completed an updated systematic review and meta-analysis of RCTs (six studies), examining topical exit site application of mupirocin compared to other exit site care interventions. 51 In contrast to previous findings of superior benefit compared to standard care, their systematic review demonstrated that it was uncertain whether the application of mupirocin ointment prevents exit site infection (RR 0.36, 95% CI 0.13–1.05). This analysis is limited by the moderately high level of heterogeneity (I 2 = 61%, p = 0.07) between the studies. 51 In summary, the available evidence from systematic reviews and meta-analyses of RCTs suggest that topical mupirocin prophylaxis may reduce the risk of catheter-related infections. However, the certainty of this evidence is reduced by indirectness (highly variable approaches to administering the intervention including nasal vs. exit site application), risk of bias and inconsistency. There is also a lack of direct comparison between nasal and exit site application of mupirocin with respect to risk of catheter-related infection. For these reasons, the Guideline Working Group downgraded the strength of the topical mupirocin prophylaxis recommendation from 1A in the 2017 Guidelines to 1C currently. It also was not able to recommend the optimal site of topical application (nasal vs. exit site). Currently, there is a multi-centre, double-blind RCT underway in Thailand (COSMO-PD Trial) examining the comparative effectiveness of local application of chlorhexidine gluconate, mupirocin ointment and normal saline for prevention of PD-related infections. 52 Hopefully, the results from this trial will help guide future recommendations on this topic.
An alternative topical antibacterial prophylactic agent is gentamicin. Daily application of gentamicin to the exit site was shown to be highly effective in preventing exit site infection caused by Pseudomonas species, and as effective as topical mupirocin in reducing S. aureus exit site infections in a three centre, double-blind RCT (n = 133). 13 However, its broad implementation has been restricted by limited availability and concerns of a change in the microbiologic profile of organisms responsible for catheter-related infection, gentamicin resistance 53,54 and development of other atypical infections. 55 Alternating between mupirocin and gentamicin exit site application has been discouraged due to observed increase in the risk of fungal peritonitis compared with gentamicin alone. 56 A recent systematic review and meta-analysis observed no difference in the rate of exit site infection between topical exit site application of mupirocin or gentamicin (2 studies, 228 participants: RR 1.14, 95% CI 0.27–4.81) with high heterogeneity (I 2 = 87%, p = 0.005). 51
Other prophylactic strategies examined include the use of medical-grade antibacterial honey at the exit site, which has been shown to have a similar risk of catheter-related infections to that of patients treated with intranasal mupirocin appointment (incidence rate ratio [IRR] 1.12, 95% CI 0.81–1.53). 57 More importantly, exit site application of honey increased the risk of catheter-related infection and peritonitis among patients with diabetes, thereby precluding its use in this subgroup. 22 There are several other studies showing mixed results pertaining to the use of topical polysporin triple ointment, 58 topical polyhexanide 59 and polyhexamethylene biguanide 60 and nanotechnology antimicrobial spray dressing 61 to prevent exit site infections. Further studies on these agents are required prior to consideration for their broad use in clinical settings.
It should also be noted that contact between ointments/creams and the PD catheter should be minimised as there have been reports that the polyethylene glycol base in mupirocin can damage polyurethane catheters and that gentamicin cream may damage silicone catheters. 62 –64
A PDOPPS study of infection prevention strategies by 170 centres caring for 11,389 patients in 7 countries reported wide variation in exit site cleaning strategies, including antibacterial soap, non-antibacterial soap, chlorhexidine, povidone-iodine, sodium hypochlorite and other agents. 17 Antibacterial soap was used to clean the catheter exit sites in 57% of US, 40% of Canadian and 39% of Australian and New Zealand units. 17 There have been studies comparing its effectiveness against other topical cleaning agents, with varying results. Povidone-iodine, also known as iodopovidone, is an antiseptic commonly used for skin disinfection before and after surgery. Its effectiveness compared to soap and water or no specific care in reducing the incidence of catheter-related infection has been inconsistently demonstrated. For example, in an RCT including 127 patients from 8 hospitals, participants receiving povidone-iodine had a significantly lower occurrence of exit site infection compared to those using soap and water (0.27 episodes/patient-year vs. 0.71 episodes/patient-year). 65 However, similar results have not been observed by others. 66 Moreover, there have been concerns regarding the risk of irritation induced by the regular application of povidone-iodine precipitating secondary exit site infection. 67 Similar concerns of local irritability have been raised for chlorhexidine gluconate (0.05–2% aqueous solution with or without isopropyl alcohol with broad-spectrum antimicrobial activities). As an alternative, chlorhexidine-impregnated sponge dressing has been developed allowing weekly application. A single-centre pilot study of 50 incident PD patients from Singapore using chlorhexidine-impregnated sponge demonstrated low catheter-related infection rates (0.09 episodes/patient-year, 95% CI 0.02–0.22) with 92% 1-year infection-free survival. Although 73% of participants reported these dressings to be acceptable, 12% developed localised contact dermatitis. 68 The outcomes from this study should be interpreted with caution due to the lack of concurrent comparison group and small sample size, warranting further studies to be conducted prior to broader implementation. Another cleansing agent, Amuchina solution, an electrolytic chloroxidizing solution containing sodium hypochlorite (3–10%), has been shown to be effective in preventing exit site infection in paediatric patients 69 without any secondary skin reaction. A retrospective observational study of 83 paediatric PD patients observed a significant reduction in catheter-related infection rates from 1.36 episodes per patient-year with application of mupirocin at exit site to 0.33 episodes per patient-year when mupirocin was augmented with sodium hypochlorite solution (p < 0.0001) without occurrence of mupirocin-resistant organisms. 70 However, these findings should be interpreted carefully due to the limitations of study sample size and design. There have also been inconsistent outcomes among studies in which head-to-head comparisons of different types of disinfectants (i.e. povidone-iodine, chlorhexidine, hypochlorite) were performed to inform clinical decision-making. 71,72 A Cochrane systematic review and meta-analysis reported very low certainty evidence that various dressing systems (chlorhexidine, povidone-iodine, sodium hypochlorite gauze + fixomull, blister film) may make little or no difference to exit site infection rates. 25 New topical antiseptic such as polyhexanide had also been tested, albeit in an underpowered study. 73
In addition to the therapeutic benefit of dressing or antiseptic agents, we should be cautious about contaminated products, especially when they are not considered to be pharmaceutical products. Suboptimal manufacturing practice or preparation could have been the cause of contaminated aqueous chlorhexidine solution, 74 –76 leading to several Burkholderia cepacia complex PD catheter exit site infection outbreaks, as reported in New Zealand 77 and Hong Kong. 74
The optimal frequency of exit site care has not been tested by RCTs. However, exit site care frequency less than twice weekly appeared to be associated with higher odds of catheter-related infections. 78 Exit site care is therefore recommended at least twice weekly, and every time after water contamination or vigorous exercise, to keep clean and dry. 79 Preliminary data suggested avoidance of water exposure to prevent introduction of water-derived organisms. In a small single-centre observational (non-randomised) study, application of a stoma bag during the daily shower was associated with reduction of exit site infection. 80 However, this evidence was very low certainty. Covering the exit site during swimming has also been recommended by the 2022 ISPD Guidelines on Physical Activity and Exercise in Peritoneal Dialysis to protect the exit site from getting wet. 79 These guidelines further suggest that ‘swimming or other water sports should preferably take place in either sea water or swimming pools that are known to be well maintained (private or municipal) to limit exposure to waterborne pathogens. (2D)’ 79 The evidence underpinning this guideline is very low certainty based on anecdotal experience.
Although previous ISPD guidelines have not addressed the care of exit site after PD discontinuation (in the setting of catheter dysfunction, hernia complication or waiting for catheter removal after kidney transplantation or transfer to haemodialysis), we recommend similar intensity or frequency of exit site care. The patient should be given information about the need to cleanse and monitor the exit site even after PD interruption or discontinuation.
Contrary to the previous recommendation to protect the exit site with dressing material such as sterile gauze coverage, continuing this practice beyond the immediate post-operative period is not supported by one RCT 18 and two observational studies. 78,81 A single-centre, open-label RCT involving 97 participants in Malaysia showed that simple washing and cleansing of the exit site followed by topical mupirocin with or without a dressing cover resulted in similar incidences of catheter-related infection. 18 The exceptionally low exit site infection rate in this study, at 0.05–0.11 episodes per year, could have limited the external validity of their findings. Rates of exit site infection were also not associated with application of dressings according to a multi-centre cross-sectional survey of 1204 patients from 12 PD centres in China. 78 Another retrospective study showed that routine dressing of the exit site (n = 54) was associated with higher exit site infection rate than in the non-dressing group (n = 12). 81 Transparent or semi-occlusive dressing material did not appear to be associated with exit site infection rates in 2460 participants in the BRAZPD II study. 82 Taken together, current evidence is not sufficient to support the use of covered dressings. Furthermore, concerns have been raised about the potential for covered dressings to cause local allergic reactions and acceleration of local bacterial growth. This information needs to be balanced against other considerations with respect to dressings, such as mitigating exposure to environmental dusts and animal danders, avoiding staining of clothing by topical antimicrobial ointment, providing extra padding and facilitating catheter immobilisation.
While there is insufficient evidence to support covering the exit site, fixing or immobilising the catheter in place is recommended to prevent traction of or frictional injury to the exit site. The practice of fixing the catheter by waist belt, protective bag or securing the transfer/extension set to the abdomen by adhesive tape is supported by several observational studies on risk factors of exit site infection. A history of catheter pulling injury or traction bleeding, based on multivariate regression analysis, was associated with increased exit site infections in two studies (hazard ratio 1.78, 95% CI 1.02–3.11 19 and 2.44, 95% CI 1.47–4.04 78 ). We believe this recommendation of fixing the PD catheter also aligns with the ISPD and the Global Renal Exercise Network practice recommendations 79 to avoid repetitive rubbing of the catheter site during sports activity, and the use of a belt during sports to provide protection.
Management of catheter-related infections
Clinical assessment
Culture swab should be taken from an exit site with purulent discharge. Gram stain is not routinely performed for exit site swab in most microbiology laboratories, unless there is drainable component. If there is a purulent discharge that can be drained, Gram stain of the drainage can be used to guide treatment.
After examination of the exit site, the tunnel of the catheter should be inspected and palpated. Tenderness over the catheter pathway and drainage from the exit site after milking the track would indicate tunnel infection which, if untreated, can progress to abscess formation or catheter-related peritonitis. Ultrasound examination can be helpful to detect tunnel involvement. 83,84 A positive finding with a sonolucent peri-catheter fluid collection helps to establish a diagnosis of tunnel infection, 83,85 although a negative examination does not rule out the condition. Additional information from colour Doppler and contrast-enhanced ultrasound might provide additional information of hypervascularity, indicative of an inflammatory process. 86,87
Care of the infected exit site
During exit site infection, the frequency of exit site inspection and cleansing is suggested to be at least daily, although there are no data to specifically support this frequency. A major goal of treatment of exit site infection is early recognition of worsening infection, including the concomitant or subsequent development of a tunnel infection. Another major reason to suggest daily care is review of the need for additional therapeutic options. Granulomas over the exit site may require additional exit site care because they are associated with exacerbated breakdown of the exit site. Treatment options include silver nitrate cauterisation, 88 topical chlorhexidine application 88 and silver ion-based dressing. 89 Although silver nitrate cauterisation has been most commonly used, this chemical agent can cause skin burns and pain. A small RCT involving 44 participants showed that chlorhexidine swab stick had similar efficacy of healing rate when compared to silver nitrate but had lower pain scores and less adverse reactions (burning sensation and staining around the exit site). 88
Empirical antibiotic treatment
We recommend empiric oral antibiotic treatment of exit site infections with appropriate S. aureus coverage such as first-generation cephalosporin or anti-staphylococcal penicillin, unless the patient has a prior history of infection or colonisation with methicillin-resistant S. aureus (MRSA) or Pseudomonas species, in which case a glycopeptide such as vancomycin (or clindamycin if known to be susceptible) or antipseudomonal antibiotic, respectively, are appropriate
Oral antibiotic therapy is often used empirically based on convenience and should primarily cover S. aureus (Figure 1). In the absence of RCTs showing head-to-head comparison for empiric antibiotic choices, the recommendation is based on clinician’s preference and patient’s risk profile.
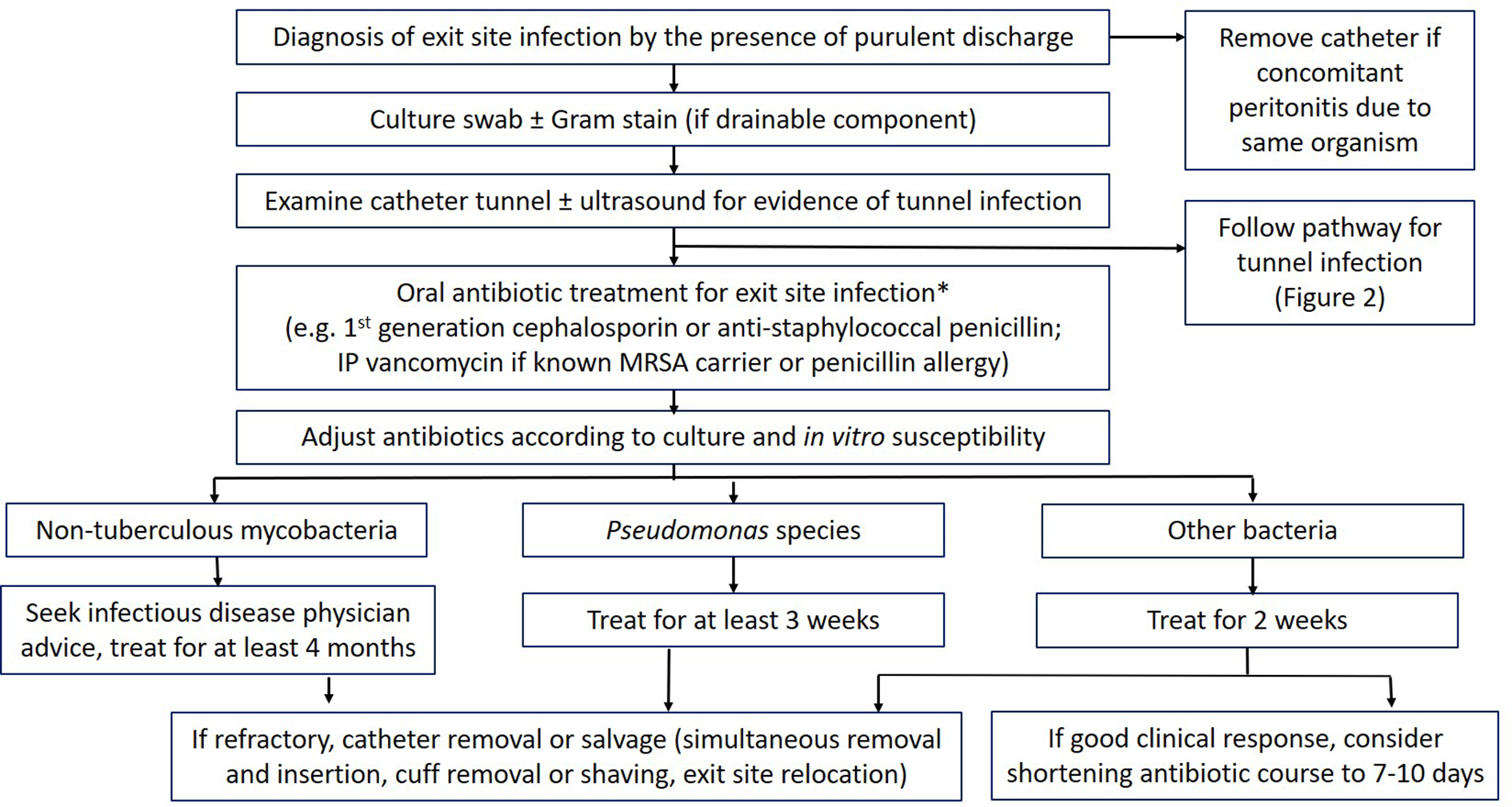
Management of PD exit site infections.
Dosing recommendations for frequently used oral antibiotics are shown in Tables 1 and 2. 77,90 In line with the 2022 Update of the ISPD Guidelines on Peritonitis Prevention and Treatment, concomitant antifungal prophylaxis should be prescribed whenever patients receive antibiotics for any reason to mitigate the risk of fungal peritonitis. 3
First-line empirical oral antibiotics used in catheter-related infections.
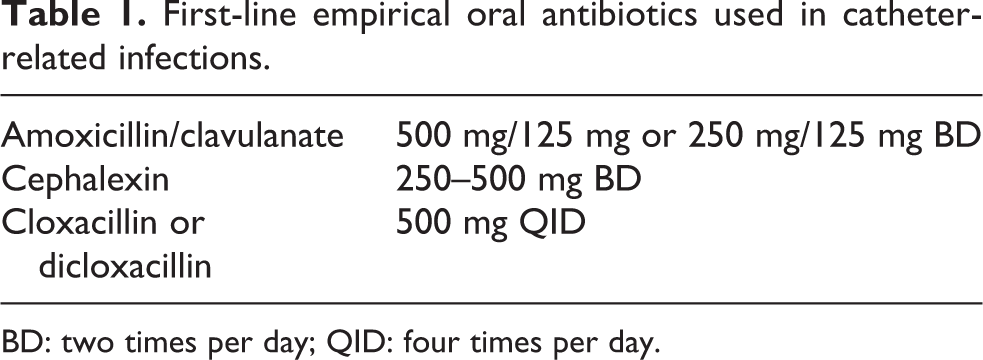
BD: two times per day; QID: four times per day.
Alternative oral antibiotics used in catheter-related infections.
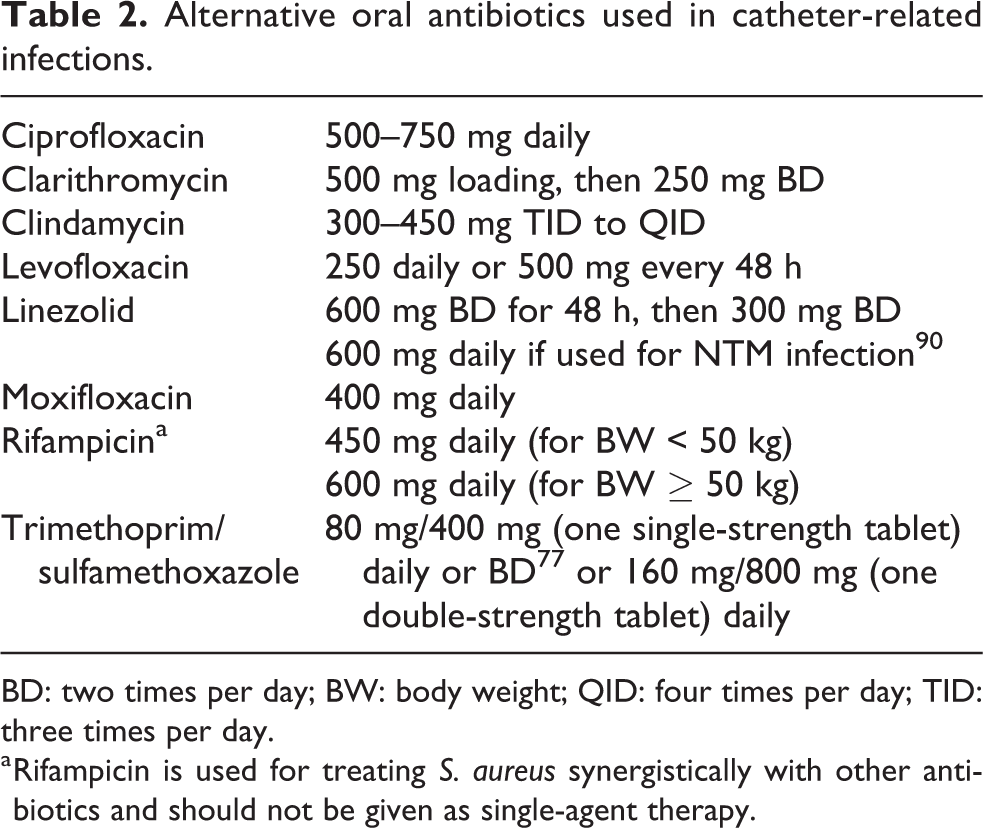
BD: two times per day; BW: body weight; QID: four times per day; TID: three times per day.
a Rifampicin is used for treating S. aureus synergistically with other antibiotics and should not be given as single-agent therapy.
Monitoring and duration of therapy
We suggest that antimicrobial treatment duration for exit site infection be adjusted according to clinical response, swab culture and in vitro susceptibility result
We suggest that a fixed 2-week antibiotic treatment duration for exit site infection can be shortened to 7–10 days if resolution of infection is confirmed by clinical evaluation at around 1 week
We recommend that exit site infection caused by Pseudomonas species be treated with at least 3 weeks of effective antibiotics
We recommend that any tunnel infection be treated with at least 3 weeks of effective antibiotics
The overarching principle is to monitor and adjust according to both clinical response and microbiological results. Patients should be reviewed within 1 week after treatment (Figure 1). Susceptibility testing is important to guide drug modification. The currently recommended first-line oral antibiotics (Table 1) might not work for organisms with increasing resistance. 91,92 The most rational approach is to arrange early review of exit site condition and susceptibility results to guide the choice and duration of treatment.
Within 1 week after initiation of treatment, physical examination of the exit site should be performed by either clinicians or nurses experienced in managing exit site infection. Remote treatment monitoring 93 coupled with real-time high-resolution image of the exit site by zoom device is considered less satisfactory because tunnel infection may need ultrasound examination.
The duration of antibiotic treatment of catheter-related infection used to be guided by entrenched practice rather than informed by high-quality evidence. Given the growing concern with unduly prolonged antibiotic therapy, we believe that duration of antibiotic treatment of exit site infection should be addressed. Although the previous guideline in 2017 recommended a minimum of 2 weeks of antibiotics for exit site infection (graded as 1C recommendation), 2 there is a lack of high-quality evidence for the mandatory 2-week treatment. The majority of the previously published guidelines and recommendations for the management of severe skin and soft tissue infections did not provide specific suggestions on the duration of therapy. 94 The Infectious Diseases Society of America (IDSA) guidelines suggest a 5-day therapy for cellulitis with an extended duration in the absence of improvement, and 7 days for superficial streptococcal and staphylococcal infections. 95 On the other hand, exit site infection of PD catheter is different from simple cellulitis or soft tissue infection because of the presence of foreign material. Since there are no biomarkers to accurately guide discontinuation of exit site infection antibiotic treatment, we believe clinical assessment is an integral basis of decision-making. Definitive antimicrobial treatment and duration are best guided by clinical response and, when available, results of wound culture and susceptibility. Our suggestion to take into consideration the clinical response is aimed to balance the risk of prolonged antibiotic therapy. It should be noted that many observational studies of fungal peritonitis in PD patients confirmed the risk factor of antibiotic use within 1 month of peritonitis onset. 96,97 Recommended treatment duration of exit site infection should count from the day of effective antibiotics. Since there are insufficient data to support a fixed 2-week course, we believe it is reasonable to prescribe antibiotics for a period of 7–10 days (Figure 1), the time required for an uncomplicated acute infection to heal. More prolonged antibiotic therapy is required when there are complicated conditions such as tunnel infection (Figure 2) or virulent organisms such as Pseudomonas species. There is no RCT evidence to guide treatment duration for tunnel infections, so the recommendation for at least 3 weeks treatment with effective antibiotics was assigned a 1D level. Despite previously recommended treatment duration of at least 3 weeks for Pseudomonas exit site infection, 2 there had also been reports of antibiotic treatment for 2 weeks. 98 –100 When there is unsatisfactory treatment response to Pseudomonas exit site infection, a second antipseudomonal drug should be added. In case of S. aureus infection with slow response, oral rifampicin can be considered but should never be given as monotherapy. There is, however, a lack of high-quality studies supporting adjunctive rifampicin therapy for S. aureus exit site infection. Such recommendation is mostly extrapolated from the experience of peritonitis treatment 101 and treatment guidelines of treating S. aureus bacteremia associated with infected prosthetic material. 102
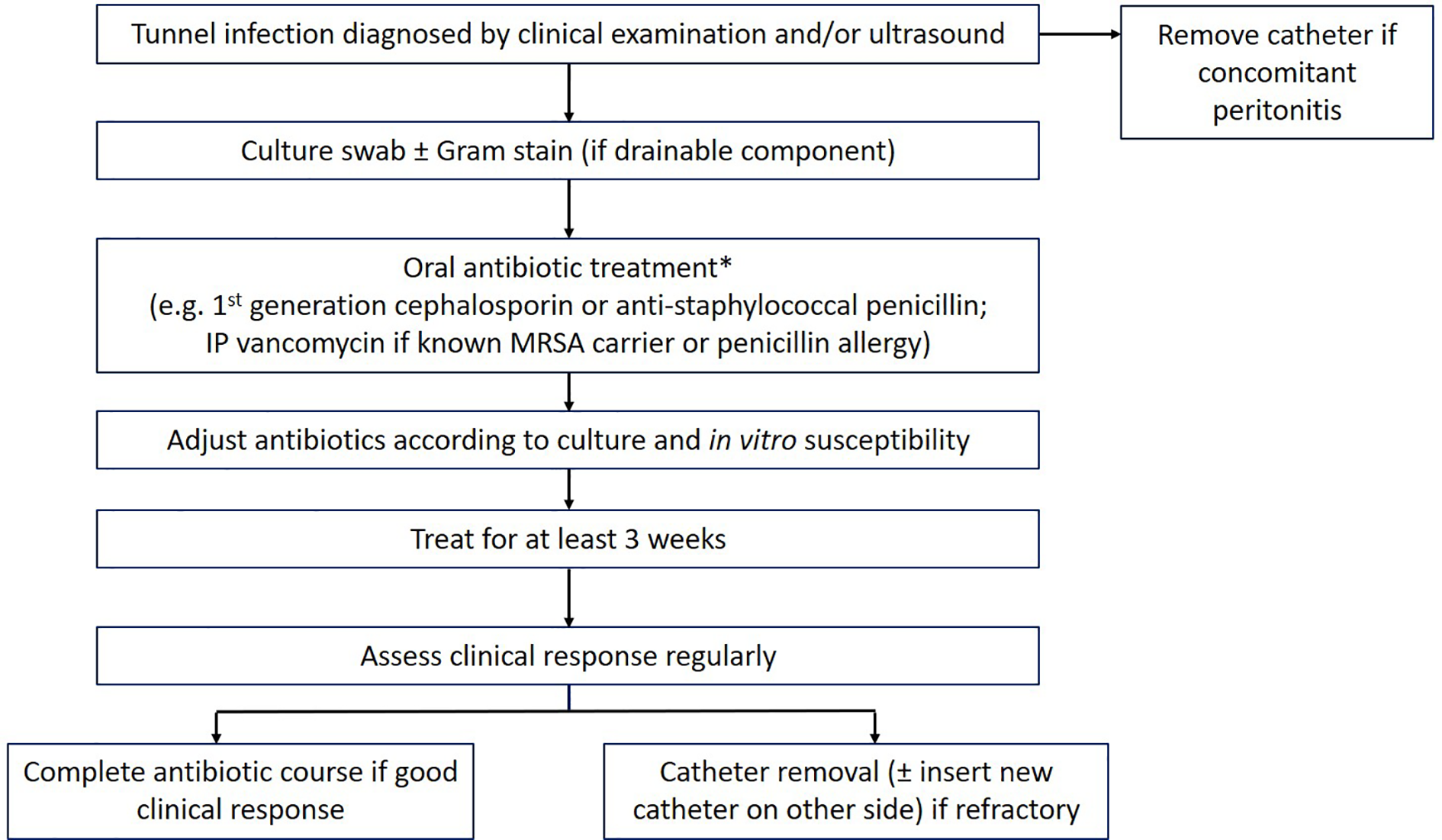
Management of PD catheter tunnel infections.
Refractory exit site infection should raise the suspicion of atypical organisms such as non-tuberculous mycobacteria (NTM). NTM can be misidentified as diphtheroids or Corynebacterium species, leading to delayed diagnosis. When suspected, examination for acid-fast bacilli by Ziehl–Neelsen staining and culture on specific media should be requested. The most common species is Mycobacterium fortuitum, followed by M. abscessus and M. chelonae. 103,104 It is necessary to differentiate isolates identified as ‘M. chelonae/abscessus’ to the species isolated since therapy for M. abscessus is more challenging. 104,105 In general, treatment with two agents with in vitro activity against the clinical isolate for a minimum of 4 months of therapy is needed for NTM infection. There is no standardised treatment recommendation for NTM exit site infection, but the IDSA guidelines highlight the need for removal of any foreign body to provide a high likelihood of cure, especially for M. abscessus. 104
Finally, observational data show the adjunctive role of ultrasonography in evaluation of treatment response. Preliminary findings suggested that a hypoechogenic zone of more than 1 mm thickness around the external cuff 1 week after completion of antibiotic treatment can predict a poor clinical outcome. 85 Another study of 43 patients with tunnel infection of single-cuff catheters showed that significant decline in the hypoechogenic zone at 2 weeks after initiating antibiotics was associated with a lower likelihood of catheter removal. 106
There is no consensus whether routine exit site wound culture should be undertaken 1–2 weeks after completion of antibiotic treatment. However, monitoring culture after primary cure of the exit site infection has been shown to detect persistent colonisation which was associated with higher risks of peritonitis 107 and transfer to haemodialysis. 107,108
Surgical interventions for catheter-related infection
We suggest removal of PD catheter in patients with exit site or tunnel infection that progresses to, or occurs simultaneously with, peritonitis due to the same organism
We suggest simultaneous removal and reinsertion of PD catheters with a new exit site under antibiotic coverage when exit site infection or tunnel infection do not resolve with effective antibiotic therapy
We recommend simultaneous removal and reinsertion of PD catheters be avoided when there is deep Dacron cuff involvement of concurrent peritonitis
We suggest that a surgical salvage procedure can be considered as an alternative to simultaneous catheter replacement in selected patients
We suggest that cuff removal or shaving be considered in PD patients with external cuff extrusion and exit site infection refractory to antibiotics
We suggest exit site relocation be considered in patients with exit site infection refractory to antibiotics
Source control remains the key management strategy for catheter-related infection when there are ongoing infection and infectious foci. As highlighted in the ISPD 2022 updated recommendations for peritonitis, simultaneous removal and reinsertion of PD catheter should not be attempted in the presence of unresolved peritonitis. 3 Catheter removal is suggested when catheter infection occurs simultaneously with peritonitis (Figure 1). This is followed by temporary haemodialysis with no attempted reinsertion of the PD catheter until at least 2 weeks after catheter removal and complete resolution of peritonitis. There are little data on timing of reinsertion of a PD catheter removed for infectious reasons. 109 A minimal wait of 2 weeks seems reasonable.
For catheter infection alone, simultaneous removal and reinsertion of the PD catheter is an option to minimise PD interruptions and alleviate the need for unplanned transfer to haemodialysis. This approach has been supported by observational studies. 110 –114 The feasibility of removal and reinsertion at a single operation has been studied in 37 cases of refractory P. aeruginosa exit site infection. All patients were kept on antibiotics for 1 week post-operatively. At 4 weeks, there was no relapse of P. aeruginosa exit site infection. 110 Post-operative antibiotic coverage duration had been extended to 2 weeks in two other case series in which patients with tunnel infection (majority of the causative organisms being P. aeruginosa and S. aureus) were also included. 112,115 Effectiveness of simultaneous catheter removal and reinsertion was more likely in S. aureus tunnel infection (including cases of simultaneous peritonitis which showed improvement including effluent white cell count). 115 Treatment success, however, was only 50% in relapsing P. aeruginosa peritonitis and tunnel infection. 115
The option of simultaneous catheter removal and reinsertion for resistant organisms including NTM can also be considered, but data for the clinical outcomes remain limited. 112,116 However, M. abscessus infection should be managed by catheter removal given the high failure rate of simultaneous catheter replacement. 104,105,117
Although simultaneous replacement of catheter has high likelihood of resolving catheter-related infection, this procedure is subject to potential complications of a new catheter, such as peri-catheter leaks and flow dysfunction. 14 Other salvage strategies have therefore been proposed. 118
Extrusion of the external cuff through the exit site is a mechanical complication resulting from shape-memory resilience forces induced by bending a catheter in the subcutaneous track that has a straight intercuff tubing segment. 14 Over time, the tubing returns to its native straight configuration with migration of the external cuff towards the exit site. If the extruded cuff is not managed, it can become seeded with bacteria and predispose to exit site infection. For patients with exposed external cuff and persistent exit site infection, removal or shaving of the external cuff can be considered when infection is limited to the exit site. Such practice was initially recommended in patients who developed relapse/repeat of Pseudomonas exit site infection. 119 More data supporting this practice come from observational studies of patients with exit site infection secondary to other causative organisms such as Staphylococcus aureus and/or epidermidis, Corynebacterium and sometimes Gram-negative species. 120 –122 The benefit of external cuff shaving for S. aureus exit site infection has been shown in three studies, in which relapse/repeat of exit site infection or peritonitis occurred in 17%, 120 50% 122 and 44%. 121 There is insufficient evidence to recommend shaving or removing the external cuff in the absence of infection, such as extrusion of cuff after substantial weight loss 122 or shape-memory resiliency forces of the catheter. We also recognise the need to balance the benefit and risk of potential complications of the procedure. In general, shaving or removing the external cuff is performed under sterile condition at the bedside or outpatient office. Techniques commonly practiced include teasing away cuffs from the PD catheters using blunt forceps. 14,120,122 Shaving the cuff using scalpels can also be performed by applying the sharp blade parallel to the exposed cuff. 121,123 Sharp dissection, however, should be cautiously performed by an experienced clinician to minimise risk of catheter damage. The blade has also to be changed often to assure ease of removing the cuff material without undue or excessive pressure from a used blade, that might cut inadvertently into the catheter lumen. Another variation of the procedure consists of deroofing the tunnel, when the cuff is partially exposed. 14 Some nephrologists give prophylactic topical or systemic antibiotics either before or after the procedure to further aid in resolution of infection. 120 –122 If there is purulent discharge at the exposed cuff, specimens should be collected for culture to guide the use of antibiotics.
In addition to removing the external cuff for refractory exit site infection, there is an alternative option of relocating the exit site. Under local anaesthesia, this outpatient procedure is performed after preoperative intravenous antibiotic administration. 124 Exposure of the external cuff is achieved by excising the exit site and the skin overlying the subcutaneous track en bloc with the underlying tissue around the catheter segment. Infected materials adjacent to the exit site and/or tunnel are removed, whereas the exposed catheter is sterilised by covering with gauzes soaked with chlorhexidine 2% solution for at least 5 min. 124 The exteriorised catheter is tunnelled subcutaneously to a new site. 124,125 Alternatively, the extraperitoneal portion of the PD catheter is cut and a new sterile catheter segment with a cuff is connected to the original one (internal cuff side) via a double barbed titanium connector. 126,127 There have been four or more single-centre observational studies that suggest a potential benefit of relocating the exit site in patients with exit site infection refractory to antibiotics. 15,124,125,127 Catheter exit site relocation success, defined as complete remission of infection not requiring additional procedures beyond 1 month after the revision, was 83% out of 52 patients, 15 90% out of 33 patients 127 and 69% out of 36 patients. 125 Although there are no RCTs comparing different strategies, the median PD catheter survival was 84 months, statistically higher than 49 months among a comparative group treated conservatively, in one observational study. 127 Importantly, this procedure allows continuation of PD. The strategy has also been reported to be beneficial in managing NTM exit site infection. 127 Treatment success without removing the entire catheter depends on the level of infection; infection should not go deeper than the superficial cuff. 127,128 In case the inner cuff is involved with infection as shown by ultrasound preoperatively 129 or during the course of operative procedure, the whole PD catheter should be removed.
According to a recent systematic review, 130 as a whole, the quality of published evidence of these salvage interventions is considered low by virtue of study design. Meta-analysis was not possible, such that it remains uncertain as to whether any technique is superior to others. Pooled analysis of cuff shaving or relocating exit site (including en bloc resection of the infected tissue) showed that these techniques are safe with procedure complication rates at 2.7%. 130 Table 3 summarises the reported outcomes of different surgical interventions. 110,112,114,115,125 –138,140,141
Outcome summary of various surgical interventions for isolated catheter-related infection without concurrent peritonitis.
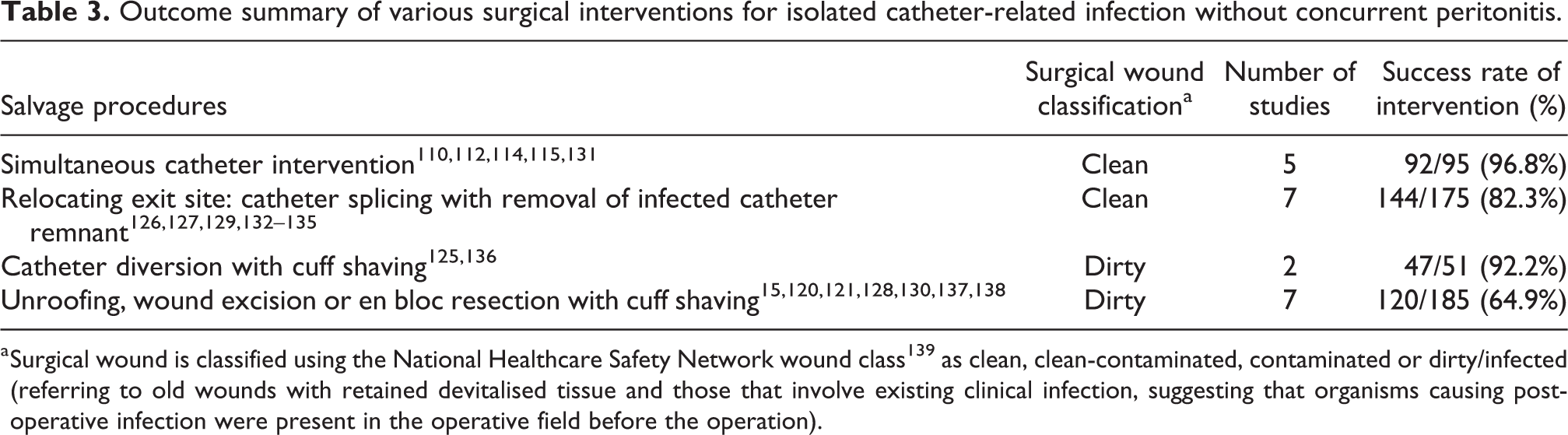
a Surgical wound is classified using the National Healthcare Safety Network wound class 139 as clean, clean-contaminated, contaminated or dirty/infected (referring to old wounds with retained devitalised tissue and those that involve existing clinical infection, suggesting that organisms causing post-operative infection were present in the operative field before the operation).
Future research
The optimal method of exit site care to prevent infection remains poorly defined. Deciphering the risk factors and mechanisms underlying catheter infection and resolution of infection may allow for greater progress in prevention and treatment.
Adequately powered trials are also needed to better define the optimal prophylactic interventions and treatment durations for exit site infections and tunnel infections. RCTs evaluating various antibiotic durations for treating prosthetic joint infection 142 and intraabdominal infection 143 have been previously performed, but this has not yet occurred for exit site infection complicating PD. Preliminary results 144 or in vitro data 145 for novel treatment option such as antimicrobial action of vinegar or its active ingredient acetic acid against Pseudomonas exit site infection should be explored. Emerging techniques, such as salvage with catheter exit site relocation, may improve PD outcomes but have not yet been systematically evaluated. Future improvements in catheter infection treatment may include point-of-care ultrasound assessment and monitoring of treatment response. 86 The incidence and prevalence of NTM catheter infection rate is increasing. 103 Given the persistent nature of the infection, ongoing prospective collection of data from registries should clarify the recommended treatment strategy.
Finally, the benchmark for exit site infection rate, which may in the long run drive the PD community to develop more effective preventive strategies, has not yet been precisely established.
Supplemental Material
Supplemental Material, sj-pdf-1-ptd-10.1177_08968608231172740 - ISPD Catheter-related Infection Recommendations: 2023 Update
Supplemental Material, sj-pdf-1-ptd-10.1177_08968608231172740 for ISPD Catheter-related Infection Recommendations: 2023 Update by Kai Ming Chow, Philip Kam-Tao Li, Yeoungjee Cho, Ali Abu-Alfa, Sunita Bavanandan, Edwina A Brown, Brett Cullis, Dawn Edwards, Isabelle Ethier, Helen Hurst, Yasuhiko Ito, Thyago Proença de Moraes, Johann Morelle, Naomi Runnegar, Anjali Saxena, Simon Wai-Yin So, Na Tian and David W Johnson in Peritoneal Dialysis International
Supplemental Material
Supplemental Material, sj-pdf-2-ptd-10.1177_08968608231172740 - ISPD Catheter-related Infection Recommendations: 2023 Update
Supplemental Material, sj-pdf-2-ptd-10.1177_08968608231172740 for ISPD Catheter-related Infection Recommendations: 2023 Update by Kai Ming Chow, Philip Kam-Tao Li, Yeoungjee Cho, Ali Abu-Alfa, Sunita Bavanandan, Edwina A Brown, Brett Cullis, Dawn Edwards, Isabelle Ethier, Helen Hurst, Yasuhiko Ito, Thyago Proença de Moraes, Johann Morelle, Naomi Runnegar, Anjali Saxena, Simon Wai-Yin So, Na Tian and David W Johnson in Peritoneal Dialysis International
Footnotes
Acknowledgement
None.
Authors’ note
Philip Li and David Johnson are co-chairs of the ISPD Catheter-related Infection Guidelines Working Group.
Author contributions
PKTL and DWJ contributed to the conceptualisation of the guideline. SWY, DWJ, YC, KMC, and PKTL conducted literature search. DWJ, YC, KMC, PKTL wrote the original draft. All authors contributed to the revision of the manuscript and the final approval of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: David Johnson has received consultancy fees, research grants, speaker’s honoraria and travel sponsorships from Baxter Healthcare and Fresenius Medical Care, consultancy fees from Astra Zeneca, Bayer and AWAK, speaker’s honoraria from ONO and Boehringer Ingelheim & Lilly, and travel sponsorships from Ono and Amgen. He is a current recipient of an Australian National Health and Medical Research Council Leadership Investigator Grant. Edwina Brown has received speaker and/or consultancy fees from Baxter Healthcare, Fresenius Medical Care, Vifor, liberDi, AWAK. Yasuhiko Ito has received research funding and/or lecture fees from Baxter, Terumo Corp. and JMS Co., Ltd. Ali Abu-Alfa has received grant support and/or speaking fees from Baxter Healthcare. Philip Li received speaker honoraria from Astra Zeneca, Baxter Healthcare, Kyowa Kirin. Yeoungjee Cho has received research grants and speaker’s honoraria from Baxter Healthcare and Fresenius Medical Care. She is a current recipient of an Australian National Health and Medical Research Council Emerging Leadership Investigator Grant and Queensland Health Advancing Research Fellowship.
Ethical approval
Not applicable.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Informed consent
Not applicable
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.